
Case Report | DOI: https://doi.org/10.31579/2641-0419/150
1 Interventional cardiologist, Erfan General Hospital, Tehran, Iran
2Weill Cornell Medicine
3 Interventional cardiology fellow, Rajaie Medical Cardiovascular and Research Center, Tehran, Iran
*Corresponding Author: Ehsan Khalilipur, Interventional cardiology fellow, Rajaie Medical Cardiovascular and Research Center, Tehran, Iran
Citation: Arash Hashemi, Ashkan Hashemi, Arsis Ahmadye., Ehsan Khalilipur., (2021) When 7 times angioplasty on Saphenous vein graft would not compete the native vessel percutaneous coronary intervention. J. Clinical Cardiology and Cardiovascular Interventions, 4(7); Doi:10.31579/2641-0419/150
Copyright: © 2021 Ehsan Khalilipur, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 February 2021 | Accepted: 24 March 2021 | Published: 02 April 2021
Keywords: coronary intervention; interventional cardiology; coronary artery bypass graft
Coronary artery bypass graft (CABG) has been the first option for revascularization in multiple vessel coronary artery disease.
One of the most major obstacles after CABGs is atherosclerotic changes of SVGand more than 50 percent ofSVGare occluded at 10 years and 25 percent show severe stenosis at angiographic follow-up. Whether native vessel percutaneous coronary intervention (PCI) on native vessel or saphenous vein graft intervention is of benefit in these patients is still a debate. In this case report we want to clarify a common clinical scenario in a patient with prior CABG seven years ago which a proper decision in the right time could save many futile efforts. The patient underwent 7 PCI on the diseased SVG on OM with frequent occlusion due to stent thrombosis and in-stent restenosis which finally native vessel antegrade CTO PCI alleviated the problem and patient followed up 2 months after the procedure without any chest pain in his ordinary activities.
Coronary artery bypass graft (CABG) has been the first option for revascularization in multiple vessel coronary artery disease [1,2]. It has been performed by using saphenous vein graft (SVG) or arterial conduit such as internal mammary or radial arteries [3,4].
The efficacy of coronary artery bypass grafting (CABG) depends on long- term arterial and venous graft patency [5].
One of the most major obstacles after CABGs is atherosclerotic changes of SVG and more than 50 percent of SVG are occluded at 10 years and 25 percent show severe stenosis at angiographic follow-up [3].
SVG failure in these patients is much more troublesome than the deterioration of native coronary artery disease [6]. PCI on native coronary artery is mostly favored to PCI on SVGs because it has been clarified that greater complications are associated with PCI on SVGs [7]. We present a post CABG patient with multiple PCI on SVG attempts and its final PCI on native coronary artery.
The patient is a 68-year-old gentleman known case of diabetes mellitus on oral agent who primarily underwent coronary angiography 8 years ago and was diagnosed with 2 vessel disease with subtotal left anterior descending (LAD) lesion at proximal part and chronic total occlusion (CTO) in dominant left circumflex artery (LCX) at its ostioproximal part and with a diminutive right coronary artery (RCA) which finally heart team decided to perform coronary artery bypass grafting (CABG) that time. Patient was successfully grafted by left internal mammary artery on LAD and saphenous vein graft (SVG) on first optus marginal branch (OM) branch of LCX. Patient was functionally active without any angina for a couple of months but gradually developed angina despite anti-anginal therapy and his cardiologist decided to perform coronary angiography which revealed significant degenerated SVG lesion in its distal part and decided to do percutaneous angioplasty on this SVG with everolimus drug eluting stent (DES) with acceptable final result (figure-1).

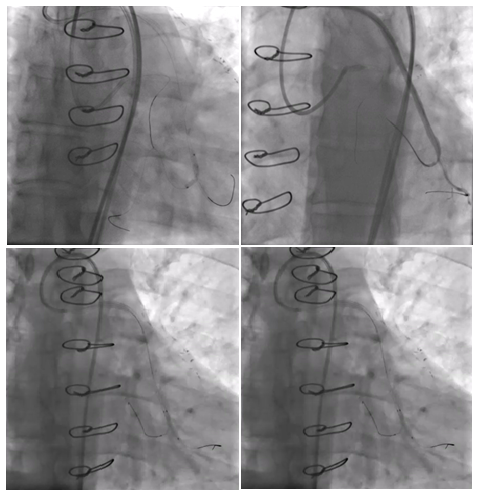
Thereafter, patient frequently developed angina and underwent 7 more times of angioplasty and stenting (twice drug eluting balloon on in-stent restenosis, three times of stenting with everolimus eluting DES and once sirolimus eluting DES) on SVG on OM with failed antegrade and retrograde wiring of native CTO of LCX artery for a couple of times. In one of the procedures, interventional cardiologist decided to do the retrograde bifurcational stenting from SVG to the retrograde part of OM which resulted in occluded retrograde part of native Om branch (figure-2).
Patient subsequently complained of low threshold angina even with 3 antianginal drug (beta-blocker, long acting nitrate and ranolazine) and was referred for more evaluation. Transthoracic echocardiography showed moderately reduced left ventricular systolic function with LVEF 35% with hypokinesia in lateral and inferior wall. Besides, we decided to image coronary artery vasculature with invasive coronary angiography which demonstrated patient LIMA on LAD and degenerated SVG and reduced TIMI flow in its proximal to distal pathway. Since resting LV function was reduced we assessed viability in LCX territory with CMR and it was compatible with a viable tissue in hypokinetic segment. At this point of time, because of metallic layers of previous stent struts in SVG and occluded retrograde route, we decided to try antegrade wire esclalation (AWE) in LCX in order to wire the native artery. We primarily tried low tip wire in proximal cap and then with wire escalation and using a microcatheter for more support, wire could successfully reach the distal part of CTO and with escalation of CTO balloons we managed to prepare the diseased part for stent deployment. Two successive everolimus eluting stents (EES) were successfully deployed (figure-3) and 2 months later patient were free of angina with a beta-blocker and had no complaint in his daily activities.

Chronic degenerative processes affect the intervention of aorto-coronary saphenous vein grafts (SVGs) irrespective of the bypassed arterial territory: about 10 percent of SVGs occlude before discharge or within the first 30 days and about 50 percent occlude within 10 years [8,9]. The best predictors of 30-day MACE of SVG intervention are SVG degeneration and plaque volume [10]. In this clinical condition, PCI on native vessel or grafts have been a debate for 2 decades. The use of PCI on a totally occluded SVG with high degeneration may worsen the condition with thrombosis and distal embolization, which can result in no-reflow phenomenon and more myocardial damage [11].
In a recent meta-analysis and systematic review performed by Mohamed Farag et al. PCI on either native coronary or SVGs were compared. Twenty-two studies comprising over forty-thousand patients with median follow-up of 2 years were included. Compared with bypass graft intervention, native artery PCI was more accessible for interventional cardiologists (61% vs. 39%) and was associated with lower major adverse cardiac events (MACE) (P<0.001), and lower target vessel revascularization (TVR) (OR 0.62, 95%CI 0.51-0.76, P<0.001) with no significant difference in the early incidence of major bleeding or stroke. The more TVR risk in bypass graft PCI group was associated with more MACE [12].
In another cohort study conducted by Ahmad Shoaib et al. with the British Cardiovascular Intervention Society (BCIS) database from 2007 to 2014 of patients who underwent SVG-PCI (n = 8619) or CTO-PCI in native arteries (n = 2513) with median age of 68 years in both groups, patients in group 2 were more men, more report of diabetes mellitus, hypertension, dyslipidemia, previous myocardial infarction. Data analysis revealed no significant difference in mortality (odds ratio [OR], 1.70; 95% confidence interval [CI], 0.63-4.58; P=.29), at 30 days or 1 year, no significant difference also was observed for in-hospital MACE rates (OR, 1.36; 95% CI, 0.85-2.19; P=.19). However, more procedural complications and vessel perforation was reported in CTO-PCI. What was remarkable in this cohort was the risk of target-vessel revascularization at 1 year which was similar (SVG-PCI 5.6% vs CTO-PCI 6.9%; P=.08) [13].
Because of the more anatomical complexity of the native vessels and the longer duration of coronary artery disease, antegrade approach of CTO in patients with prior CABG is more sophisticated [14]. As we depicted in our patient, retrograde pathway was unintentionally inaccessible because of previous procedures and the only route to alleviate the ischemia was antegrade approach. We could precisely escalate wires in order to cross distal part of the CTO with a microcatheter support and finally LCX artery was revascularized by deploying EES with acceptable result in spite of inability to wire OM branch which had a degenerated SVG.
As it is remarkable in recent studies, it is still a debate to decide whether to intervene on native CTO or SVG’s. As we have shown in this case report, native vessel intervention is prerferred approach however, heart-team approach would be as a lighthouse to guide for a better decision making in these patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
