
Research Article | DOI: https://doi.org/10.31579/2768-2757/064
Vascular Surgery, Royal Free Hospital, London, United Kingdom.
*Corresponding Author: Lucinda Cruddas, Vascular Surgery, Royal Free Hospital, London, United Kingdom.
Citation: Cruddas L., Daryll M. Baker. (2023). What is the Relationship between Chronic Heart Failure and operation size? A systematic Review. Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/064
Copyright: © 2023 Lucinda Cruddas. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 December 2022 | Accepted: 04 January 2023 | Published: 09 February 2023
Keywords: heart failure; morbidity; mortality; perioperative risk; surgery
Background:
Heart failure is a chronic progressive failure of the heart muscle to pump blood to meet the body’s oxygen demands. Heart failure impacts on perioperative outcomes of non-cardiac surgery, with higher risks of post-operative complications and mortality. The aim of this study was to review current clinical evidence to assess if there was a relationship between heart failure, operation size and post operative outcomes
Methods:
PRISMA guidelines were implemented to complete a systematic review. The review was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD42022313897). PubMed was searched from 1940 to 2022 using the terms “heart failure”, “noncardiac surgery”, “thyroid surgery”, “breast surgery”, “asymptomatic carotid endarterectomy”, “hernia”, “cholecystectomy”. “laparoscopy”, laparotomy”, “peripheral angioplasty”, “EVAR”, “neck of femur”, “abdominal aortic aneurysm”, and “lower extremity revascularisation”. Inclusion criteria included: experimental and observational studies; pre operative diagnosis of heart failure; 30d morbidity and mortality; non cardiac surgery.
Results:
47 articles relevant to the inclusion criteria were analysed. Five studies assessed low risk operations; 29 assessed intermediate risk operations; 8 assessed high risk operations; 5 assessed intermediate and high-risk operations. For low, intermediate and high-risk operations, heart failure was associated with a statistically significant increased risk of mortality and morbidity (p lessthan0.05).
Conclusions:
Heart failure is associated with increased morbidity and mortality independent of operation size or risk. Challenges remain in assessing the relationship between heart failure and operation outcome due to variations in disease spectrum and the impact of additional co-morbidities.
Heart failure is a physiological failure of the heart pump to meet the body’s demands for oxygen. It is diagnosed as a constellation of signs and symptoms, and a demonstrated reduced left ventricular ejection function (LVEF) or preserved LVEF with structural disease and/or diastolic dysfunction, on echocardiogram [1]. Symptoms include breathlessness, fatigue and reduced exercise tolerance. Clinical signs of right sided heart failure include peripheral oedema, whilst left sided heart failure is characterised by signs of pulmonary oedema including tachypnoea, raised jugular venous pressure and reduced oxygen saturations. Heart failure is common, and in developed countries, affects graterthan10percentage of the population graterthan70 years old [2]. It is a progressive condition although has an unpredictable course [3]. Heart failure can be categorised using either ACC/AHA classification (Table 1) [4] or New York Heart Association (NYHA) functional classification (Table 2) [5].
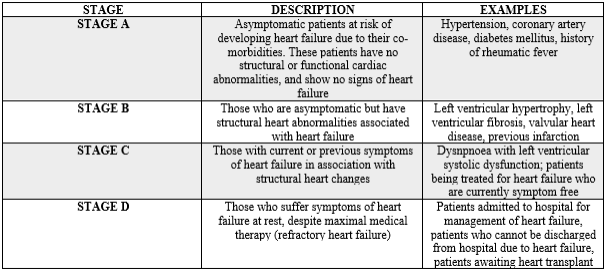
Table 1: American College of Cardiology/ American Heart Association time line classification of heart failure

Table 2: New York Heart Association (NYHA) classification of heart failure
Heart failure impacts on perioperative outcomes of non-cardiac surgery. Patients with heart failure have been shown to have a higher risk of 90-day post-operative mortality and 30-day post-operative complications, than patients without heart failure [6,7,8,9,10,11]. This risk is proportional, and mortality risk increases as systolic function decreases [6,12,13] or in cases of acute heart failure [9]. Increased mortality is also observed in both elective and emergency non-cardiac procedures [7,14]. The rates of post-operative mortality may be higher in woman than men with heart failure [11]. Overall, the mechanism of increased mortality is poorly understood. Alongside increased mortality, patients with heart failure undergoing non-cardiac surgery suffer increased post-operative morbidity. Post-operative cardiac events are more frequent in patients with heart failure [15,16,17,18,19,20]. This is the case for patients with reduced right heart function, as well as patients with lower LVEF [21,22]. Cardiac complications are associated with longer inpatient stays, death and higher costs [16,17]. As well as cardiac complications, patients with heart failure are at increased risk of post-operative pulmonary embolism, acute renal failure, need for mechanical ventilation for over 48 hours, unplanned intubation, cerebrovascular event, pneumonia, urinary tract infection, sepsis and admission to intensive care [20,23,24]. These patients are more likely to require hospital readmission [7]. This highlights the importance of identification of patients with heart failure, and their optimisation during the perioperative period.
A systematic review of articles was performed to assess outcomes of patients with heart failure for different operations, based on the Preferred Report Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. The review was registered with PROSPERO (ID CRD42022313897).
Inclusion and Exclusion Criteria:
In this review, the relationship between heart failure and size of operation was assessed by classifying operations as low, intermediate or high risk (Table 3). The relationship was assessed in the perioperative and immediate post-operative period (30-day post procedure). Patient morbidity and mortality were assessed as opposed to the long-term operative success. Outcomes were assessed in individuals with heart failure, compared to those without heart failure.
Inclusion criteria:
Exclusion criteria:
Search methods and selection of studies:
Pubmed was searched from 1940 to 2022 based on the following search terms: “heart failure”, “ noncardiac surgery”, “thyroid surgery”, “breast surgery”, “asymptomatic carotid endarterectomy”, “hernia”, “cholecystectomy”. “laparoscopy”, laparotomy”, “peripheral angioplasty”, “EVAR”, “neck of femur”, “abdominal aortic aneurysm”, and “lower extremity revascularisation”. These terms were selected following the definition of these surgeries as low, intermediate and high risk (Table 3). Each of these terms was searched independently alongside “heart failure”. No filters or limits were applied. Analysis of paper screening and selection was demonstrated (Figure 1).
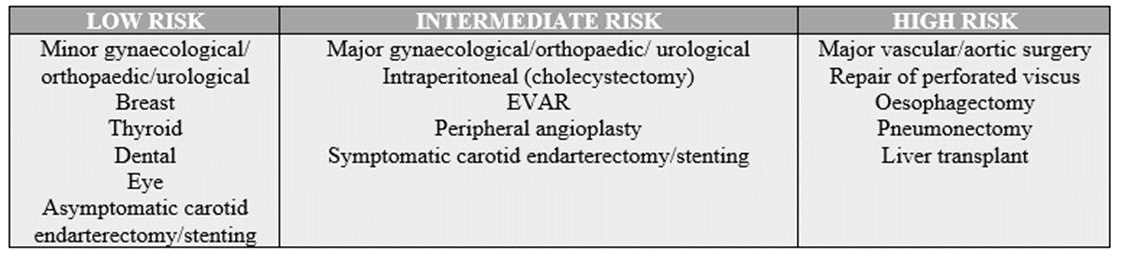
Table 3: Estimation of surgical risk according to procedure [adapted from 30]

Figure 1: PRISMA flow chart for selection of papers for review
Each search was performed independently by the two lead authors to avoid bias, and articles which did not meet the inclusion criteria were rejected. Paper title and abstracts were assessed for relevance independently by the two authors, and full texts were examined in cases where relevance was not clear from this initial screen. Selected articles were read and rejected if they did not meet the inclusion criteria. This data was extracted from included papers and transferred to an Excel spreadsheet, and collated into tables (Tables 4,5,6).
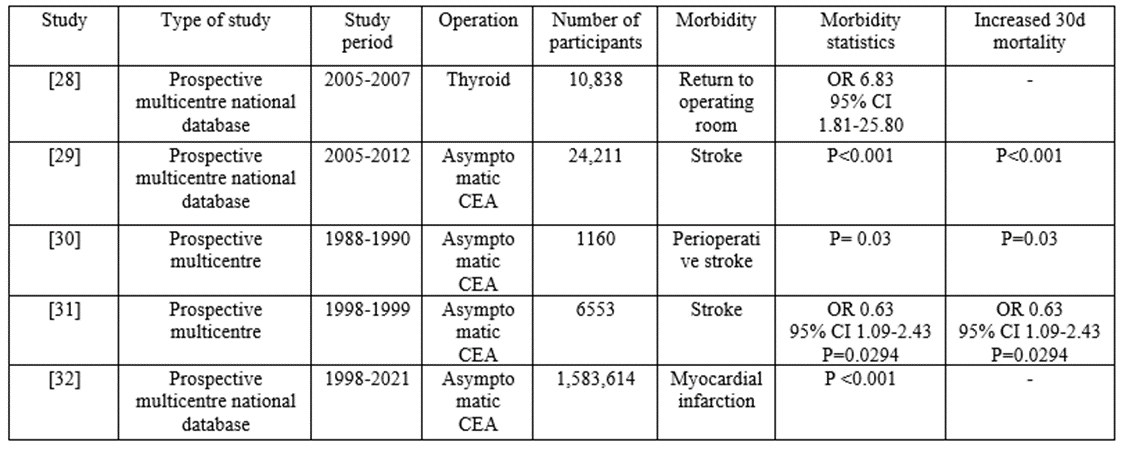
Table 4: Table demonstrating relationship between heart failure and post-operative morbidity and mortality in low risk surgeries
| Study | Type of study | Study period | Operation | Number of participants | Morbidity | Morbidity statistics | Increased 30d mortality |
| [34] | Prospective multicentre national database | 2009-2010 | Ventral and incisional hernia: emergency; elective | 28,286 | Prolonged length of stay for incarcerated/strangulated hernias following ventral/ inguinal hernia repair | Plessthan0.040
| - |
| [35] | Prospective multicentre | 2008-2014 | Elective ventral hernia: open; laparoscopic | 103,635 | - | - | OR= 2.15 95percentage CI 1.32-3.47 P=0.002 |
| [36] | Prospective multicentre national database | 2007-2008 | Inguinal hernia: open, laparoscopic, emergency and elective | 2,377 | Wound complications, pulmonary complications, urinary tract complications, cardiac complications | OR 4.3 95percentage CI 1.5-12.6 | - |
| [37] | Prospective multicentre national database | 2007-2015 | Cholecystectomy: open and laparoscopic | 478,111 | Hospital length of stay | Plessthan0.001 | OR 1.31 95percentage CI 1.16-1.48 Plessthan0.001 |
| [38] | Prospective multicentre national database | 2008-2012 | Elective and emergency laparoscopic cholecystectomy | 143,761 | Pneumonia or reintubation | Plessthan0.01 | Plessthan0.01 |
| [39] | Prospective multicentre national database | 1998-2016 | Cholecystectomy: open and laparoscopic | 282,184
| Pneumonia | OR 1.965 95percentage CI 1.587-2.438 Plessthan0.0001 | - |
| [40] | Prospective multicentre national database | 2009-2010 | Cholecystectomy: open and laparoscopic | 53,632 | 30d readmission | OR 2.1 95percentage CI 1.8-2.4 Plessthan0.0001 | - |
| [41] | Prospective single centre | 1993-2006 | Elective laparoscopic sigmoid resection for diverticular disease | 526 | Post operative medical complications (pneumonia, pulmonary embolism, thrombosis, cardiac failure or infarction, renal failure) | OR 3.27 95percentage CI (1.37-7.8) Plessthan0.008 | - |
| [42] | Prospective multicentre database | 2005-2012 | Bariatric surgery: laparoscopic; open; | 102,869 | Post operative pulmonary embolism (PE) (laparoscopy) | OR 6.03 95percentage CI 1.45-25.10 Plessthan0.014 | - |
| Post operative deep vein thrombosis (DVT) (laparoscopy) | OR 4.64 CI 95percentage 1.13-19.11 Plessthan0.034 | ||||||
| Post operative PE (open) | OR 10.32 CI 95percentage 1.29-82.65 Plessthan0.028 | ||||||
| Post operative DVT (open) | OR 7.72 CI 95percentage (0.97-61.49) Plessthan0.053 | ||||||
| [43] | Prospective multicentre database | 2004-2007 | Elective left-colon resection, colostomy, ileostomy for diverticulitis
| 22,752
| Haemorrhage | OR 1.5 95percentage CI 1.69-2.27 | OR 3.5 95percentage CI 2.59-4.63
|
| Wound | OR 1.9 95percentage CI 1.50-2.39 | ||||||
| Pulmonary | OR 4.2 95percentage CI 3.59-4.85 | ||||||
| Cardiac | OR 4.6 95percentage CI 3.68-5.74 | ||||||
| Sepsis | OR 3.2 95percentage CI 2.53-4.35 | ||||||
| Renal | OR 4.1 95percentage CI 3.22-5.12 | ||||||
| Thromboembolic | OR 1.6 95percentage CI 1.00-2.50 | ||||||
| [44] | Prospective multicentre | 1993-1999 | Elective colectomy via laparotomy | 1721 | Colorectal cancer morbidity | OR 3.0 CI 95percentage 1.42-6.32 P=0.003 | - |
| [45] | Prospective multicentre | 2005-2007 | All abdominal surgeries | 202 | Surigcal site infection | OR 1.9 95percentage CI 1.20-3.04 P=0.011 | - |
| [46] | Prospective multicentre | 1997-2009 | Damage control laparotomy with open abdomen for acute general and vascular | 67 | - | - | OR 11.4 95percentage CI 1.01-128.03 |
| [47] | Prospective multicentre database | 2015-2016 | EVAR, CEA, open AAA, peripheral bypass | 88,791 | Post operative MI | Plessthan0.001 | - |
| [48] | Prospective multicentre database | 2012-2017 | EVAR, CEA, open AAA, peripheral bypass | 26,231 | Post operative MI | OR 1.52 95percentage CI 1.16-1.98 | |
| [50] | Prospective multicentre | 2012-2014 | Infrainguinal endovascualar intervention | 4449 | 30 day redmission | OR 1.6 CI 95percentage 1.1-2.5 | - |
| [51] | Prospective multicentre database | 1997-2010 | Percutaneous angioplasty for peripheral arterial disease | 7568 | - | - | OR 1.62 95percentage CI 1.32-1.98 |
| [52] | Prospective single centre | 2008-2017 | EVAR | 136 | Myocardial injury (post operative rise in troponin) | P=0.016 | - |
| [53] | Prospective multicentre database | 2003-2016 | Elective EVAR | Major adverse event (MI, dysrhythmia, heart failure, leg ischaemia, renal insufficiency, bowel complication, reoperation, surgical site infection, stroke, respiratory complication, no discharge home | OR 1.7 95percentage CI 1.5-1.9 P=0.001 | - | |
| [54] | Prospectivemulticentre database
| 2003-2017 | EVAR | 28,240 | In hospital event (MI, dysrhythmia, heart failure, stroke, pneumonia, respiratory failure, renal failure, lower extremity ischaemia, bowel ischaemia, reoperation | OR 2.20 CI 95percentage 1.64-2.95 Plessthan 0.001 | - |
| [55] | Prospectivemulticentre database | 2003-2014 | Elective EVAR | 3,979 | Prolonged intubation | Plessthan0.05 | - |
| [56] | Prospective two centre | 1995-1998 | EVAR | 113 | Adverse cardiac event | P = 0.005 | - |
| [57] | Prospective multicentre database | 2005-2013 | EVAR | 21,769 | Protracted length of stay | OR 1.8 CI 95percentage 1.4-2.4 | - |
| [58] | Prospective multicentre database | 2012-2013 | EVAR | 3886 | 30 day readmission | Plessthan0.5 | - |
| [59] | Prospective multicentre database | 2012-2014 | EVAR | 120,646 | 30d readmission | OR 1.8 95percentage CI 1.4-2.3 Plessthan0.0001 | - |
| [60] | Prospective multicentre database | 2001-2004 | EVAR | 11,415 | - | - | OR 2.4 95percentage CI 1.8-3.4 Plessthan0.0001 |
| [61] | Prospectivemulticentredatabase | 2005-2010 | Elective EVAR | 11,229 | - | - | Plessthan0.05 |
| [63] | Prospective multicentre database | 2014-2018 | Elective TEVAR | 1469 | Non home discharge | Plessthan0.05 | - |
| [64] | Prospective, multicentre database | 2006-2007 and 2009-2010 | Total hip replacement, total knee replacement, AAA repair | 429,509 | Readmission | OR 1.23 95percentage CI 1.28-1.38 Plessthan0.001 | OR 6.79 95percentage CI 5.48-8.42 Plessthan0.001 |
| Length of stay | OR 2.5 95percentage CI 2.31-2.71 Plessthan0.001 | ||||||
| [65] | Prospectivesingle centre | 2004-2018 | Repair hip fracture | 1992 | - | - | OR 4.01 95percentage CI 1.10-8.78 P=0.009 |
| [66] | Prospectivesingle centre | 2011-2014 | Repair hip fracture | 331 | - | - | OR 6.2 CI 95percentage 1.8-20.9 P=0.003 |
| [67] | Prospectivesingle centre | 2009-2013 | Repair hip fracture | 99 | - | - | P=0.036 |
| [68] | Prospectivemulticentre database | 2005-2016 | Total knee and hip replacement | 537 | Pneumonia | P=0.003 | Plessthan0.001 |
| Renal insufficiency | P=0.040 | ||||||
| Myocardial infarction | P=0.050 | ||||||
| Extended length of stay (graterthan5) | Plessthan0.001 | ||||||
| Readmission | OR 1.23 95percentage CI (1.09-1.39) | ||||||
| [69] | Prospective single centre | 2013-2017 | Repair neck of femur fracture | 285 | Post operative aki | Plessthan0.05 | - |
Table 5: Table demonstrating relationship between heart failure and post-operative morbidity and mortality in intermediate risk surgeries
| Study | Type of study | Study period | Operation | Number of participants | Morbidity | Morbidity statistics | Mortality statistics |
| [27] | Prospective, multicentre database | 1997-1998 | Major non cardiac (abdominal, vascular, orthopaedic) | 23,340 | Readmission | Plessthan0.001 | Plessthan0.001 |
| [47] | Prospective, multicentre database | 2015-2016 | Infrainguinal bypass, open AAA | 88,791 | Post op MI | Plessthan0.08 | - |
| [56] | Prospective two centre | 1995-1998 | Elective open AAA repair | 113 | Adverse cardiac event | P=0.001 | - |
| [60] | Prospective multicentre database | 2001-2004 | Open AAA repair | 11,415 | - | - | OR 2.1 95percentage CI 1.7-2.6 Plessthan0.001 |
| [64] | Prospective multicentre database | 2006-2007 and 2009-2010 | AAA | 14,524 | Increased length of stay | OR 1.78 95percentage CI 1.46-2.16 Plessthan0.001 | OR 3.54 95percentage CI 2.65-4.73 Plessthan0.001 |
| Readmission | OR 1.47 95percentage CI 1.11-1.94 Plessthan0.006 | ||||||
| [70] | Prospective single centre | 1987-1988 | AAA repair
| 72 | Post operative cardiac failure | P=0.004 | Plessthan0.001 |
| [71] | Prospective single centre | 1991-2001 | Open TAA | 854 | - | - | Or 1.85 95percentage CI 1.09-3.15 P=0.03 |
| [72] | Prospective multicentre database | 2002-2014 | EVAR-c and primary open | 6429 | Major adverse cardiac event | OR 1.5 CI 95percentage 0.98-2.34 | - |
| [73] | Prospective multicentre database | 2009-2015 | Open AAA repair and EVAR | 33,332 | 30d readmission | Plessthan0.05 | - |
| [74] | Prospective multicentre database | 2005-2010 | Infrainguinal bypass | 18,645 | Cardiac event | P=0.007 | Plessthan0.0001
|
| Pneumonia | P=0.014 | ||||||
| Prolonged intubation | P=0.011 | ||||||
| Reintubation | P=0.014 | ||||||
| Sepsis | P=0.011 | ||||||
| Re-operation | P=0.022 | ||||||
| LOS graterthan9 days | P=0.0001 | ||||||
| [75] | Prospective multicentre database | 2013-2016 | Arterial reconstruction for revascularisation | 2906 | Major adverse limb event 30d after revascularisation | OR 1.10 | |
| [76] | Prospective multicentre database | 2011-2013 | Infrainguinal bypass | 1,055 | - | - | OR 4.46 95percentage CI 1.20-16.57 Plessthan0.025 |
Table 6: Table demonstrating relationship between heart failure and post-operative morbidity and mortality in high risk surgeries
Data extraction included: study type; study period; operation performed; number of patients; morbidity; and mortality. Association of heart failure and post-operative morbidity and mortality was demonstrated by comparing patients with preoperative heart failure, and those without. Results were assessed for significance based on odds ratio, confidence interval and p value.
PubMed identified 297 articles for “heart failure” and “noncardiac surgery”, 436 articles for “heart failure” and “breast surgery”, 371 articles for “heart failure” and “thyroid surgery”, 86 articles for “heart failure” and “asymptomatic carotid endarterectomy”, 206 articles for “heart failure” and “hernia”, 118 articles for “heart failure” and “cholecystectomy”, 276 articles for “heart failure” and “laparoscopy”, 253 articles for “heart failure” and “laparotomy”, 186 articles for “heart failure” and “peripheral angioplasty”, 90 articles for “heart failure” and EVAR”, 87 articles for “heart failure” and “neck of femur”, 1168 articles for “heart failure” and “aortic aneurysm”, and 145 articles for “heart failure” and “lower extremity revascularisation”. Articles were screened and duplicates removed. This led to the final inclusion of 47 articles. One study was included for thyroid surgery, 4 studies were included for asymptomatic carotid endarterectomy, 3 studies were included for hernia surgery, 4 studies were included for cholecystectomy, 3 studies were included for laparoscopy, 3 studies were included for laparotomy, 2 studies were included for peripheral angioplasty, 9 studies were included for EVAR, 5 studies were included for neck of femur fracture repairs, 4 studies were included for aortic aneurysm (AAA) repair, 3 studies were included for lower extremity revascularisation, and 1 study was included for noncardiac surgery. There were no studies which examined the relationship of outcomes of patients with heart failure undergoing breast surgery. One study assessed the relationship between heart failure and outcomes in both abdominal aortic aneurysm and hip/knee replacement. Two studies assessed the relationship between heart failure and outcomes in both open and endovascular abdominal aneurysm repair. Two papers looked at the relationship between heart failure and outcomes in all vascular operations (EVAR, peripheral bypass, open AAA repair). Results are demonstrated in Table 4 for low-risk surgeries, Table 5 for intermediate risk surgeries, and Table 6 for high-risk surgeries.
Patients undergoing low, intermediate and high risk non-cardiac surgeries are at risk of increased morbidity and mortality [6, 26,27].
Heart failure and low risk surgeries:
There are limited studies on the outcomes of patients with heart failure undergoing low risk surgery. A large prospective, multi-centre national study of patients undergoing thyroid surgery showed that congestive heart failure was associated with increased risk of complications and return to the operating theatre (OR 6.83, 95percentage CI 1.81-25.80) [28]. In asymptomatic patients undergoing carotid endarterectomy (CEA), patients with congestive heart failure have been shown to have an increased risk of post-operative stroke and death [29,30,31]. In a large multicentre national prospective study, congestive heart failure was also a predictor of post-operative myocardial infarction in asymptomatic patients undergoing CEA (Plessthan0.001) [32]. Routine cardiology consultation may be of benefit in patients prior to surgery for asymptomatic CEA to reduce perioperative cardiac complications and mortality [33]. There is no literature to assess the impact of heart failure on the perioperative outcomes of breast surgery.
Heart failure and intermediate risk surgeries:
General surgery:
Heart failure has been shown to be associated with increased hospital length of stay (plessthan0.04) [34] and mortality (plessthan0.002) [35] in inguinal and ventral hernia repairs. One prospective multicentre study demonstrated that heart failure was associated with increased rates of wound, pulmonary, urinary tract and cardiac complications following hernia surgery (OR 4.3 95percentage CI 1.5-12.6) [36]. Heart failure has also been shown to impact on the perioperative and postoperative course of patients undergoing cholecystectomy. Patients with heart failure have been shown to have increased hospital length stays (plessthan0.001) [37], and increased rates of pneumonia and reintubation (plessthan0.01) [38,39] and post-operative readmission at 30 days (plessthan0.0001) [40]. This is the case in both elective and emergency procedures. Individuals with heart failure who undergo elective laparoscopic sigmoid resection for diverticular disease have been shown to suffer greater perioperative complications including pneumonia, pulmonary embolism, thrombosis, cardiac failure or infarction and renal failure (OR 3.27 95percentage CI 1.37-7.8 plessthan0.008) [41]. In a large prospective study assessing the outcomes of bariatric surgery, patients with heart failure have been shown to be more likely to suffer from post-operative DVT and PE [42]. Heart failure is likely to impact on the outcomes of intermediate laparoscopy and laparotomy. A large, prospective, multicentre study revealed that patients with heart failure are more likely to suffer post-operative mortality (OR 3.5 95percentage CI 2.59-4.63) and complications including haemorrhage, wound, pulmonary, cardiac, sepsis, renal and thromboembolic, following elective left colonic resection, with colostomy or ileostomy for diverticulitis [43]. Post-operative morbidity following elective colectomy via laparotomy for colon cancer has been shown to be significantly higher in patients with heart failure (OR 3.0 CI 95percentage 1.42-6.32 P=0.003) [44]. Heart failure may also be associated with a higher risk of surgical site infection following laparotomy (OR 1.9 95percentage CI 1.29-3.04) [45]. In damage control laparotomy, individuals with heart failure may be at higher risk of post-operative mortality (OR 11.4 95percentage CI 1.01-128.03) [46].
Vascular:
In all vascular procedures, classified as high and intermediate risk, patients with heart failure were more likely to suffer post-operative myocardial infarction [47,48]. Pre-operative cardiac assessment does not appear to improve outcomes [49]. Patients with heart failure may be at increased risk of unplanned 30-day re-admission (OR 1.6 CI 95percentage 1.1-2.5) [50] and increased mortality (OR 1.62 95percentage CI 1.32-1.98) [51] following endovascular peripheral angioplasty. In both elective and emergency endovascular aneurysm repair (EVAR), large prospective multi-institutional studies have demonstrated that heart failure is associated with increased risk of postoperative myocardial injury, pneumonia, heart failure, limb ischaemia, renal dysfunction, bowel complications, reoperation, surgical site infection, stroke, prolonged intubation, respiratory complications and discharge to a facility [47,48,51,53,54,55,56,57,58,59]. A large prospective multicentre database study has also demonstrated that heart failure is an independent predictor of mortality in patients undergoing EVAR (Plessthan0.05) [60,61]. Patients who are deemed unfit for open repair of their aneurysm and subsequently have EVAR, commonly have heart failure, and suffer greater post-operative cardiopulmonary complications and perioperative mortality [62]. Patients with heart failure who had a thoracic endovascular aortic repair (TEVAR) have also been shown to be at increased risk of discharge to a facility [63] (plessthan0.05).
Orthopaedic:
In individuals who underwent surgical fixation for a neck of femur fracture, heart failure was a risk factor for 30-day mortality [64,65,66,67,68,69]. Heart failure was also demonstrated as a risk factor for post-operative complications including: pneumonia (p=0.003) [68]; renal insufficiency (p=0.40) [68]; myocardial infarction (p=0.50) [68]; AKI (plessthan0.05) [69]; extended length of stay (plessthan0.001) [68]; and readmission (plessthan0.001) [68].
Heart failure and high-risk surgeries:
Heart failure is associated with significant morbidity and mortality in patients undergoing major non-cardiac surgery. This is despite advances in perioperative care [27]. Patients with heart failure suffer significantly worse outcomes than those patients with coronary artery disease alone [27].
Vascular:
Whilst there is limited evidence that cardiac testing prior to open abdominal aortic aneurysm (AAA) repair may not improve surgical outcomes in patients, large prospective studies suggest that heart failure is an independent risk factor for post-operative mortality (plessthan0.001) [60,64,70]. Pre-operative heart failure is also associated with post-operative mortality in open thoracic aortic aneurysm (TAA) repair (OR 1.85 95percentage CI 1.09-3.15 p=0.03) [71]. As well as mortality, patients with heart failure suffer increased morbidity, as post-operative major adverse cardiac events after emergency and elective open AAA repair, as well as conversion to open AAA repair from EVAR [56,70,72]. Heart failure has also been shown to be associated with post-operative 30-day readmission (plessthan0.05) [65,73] and increased length inpatient stay (plessthan0.001) [64]. The degree of heart failure, and LVEF, may be proportionate to post-operative morbidity and mortality [70]. Heart failure has also been shown to impact on 30-day outcomes of lower extremity revascularisation. In a large, prospective multi-centre study, patients with heart failure are more likely to suffer post-operative complication rates such as return to the operating theatre (p=0.022), prolonged intubation (p=0.011), reintubation (p=0.014), pneumonia (p=0.014), sepsis (p=0.011), extended inpatient stay (p=0.0001) and mortality (plessthan0.0001) [74]. Subsequent below knee or above knee amputation is associated with increased mortality in patients with heart failure (OR 1.10) [75]. Unfortunately, pre-operative identification of cardiac risk scores does not appear to improve outcomes for diabetic patients undergoing lower extremity revascularisation [76]. Large multi-centre studies have demonstrated that patients with heart failure undergoing infrainguinal bypass are at increased risk of mortality (plessthan0.025) [75,77].
Weakness of Evidence:
Patients with heart failure are likely to suffer additional co-morbidities and it is difficult to ascertain the impact of heart failure on post-operative outcomes alone. Additionally, certain combinations of different co-morbidities may be associated with worse outcomes. The term “heart failure” encompasses a wide spectrum of disease, and undoubtedly certain individuals included in this study will suffer more severe disease than others. Different studies have used different definitions of heart failure (grades of NYHA) and different end points. Additionally, immediacy and pre-operative optimisation will impact outcomes. The purpose of this study however was to perform a general assessment and whilst acknowledging these limitations, demonstrating an overarching trend in the existing evidence.
Heart failure is a major risk factor for morbidity and mortality in patients undergoing non-cardiac surgery. Morbidity and mortality appear to be consistent from low to high-risk operations. Heart failure is not binary, but exists on a disease spectrum. Operative risk is therefore a combination of factors including: urgency of surgery; degree of heart failure and opportunity for pre-operative optimisation; additional patient co-morbidities; and intraoperative course including blood loss and fluid shifts. Unfortunately, despite preoperative optimisation, patients with heart failure still suffer higher operative risk than those patients without heart failure. Additionally, current guidelines and risk scores classify heart failure as a binary outcome, and do not account for the breadth of disease under this single label.
No funding was received for the review.
LC: data collection; data analysis and interpretation; drafting article; approval of final version.
DB: study design; data collection; data analysis and interpretation; revising article; approval of final version.
None
Nil.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
