
Reprint | DOI: https://doi.org/10.31579/2690-1919/115
Anthony Bates Foundation, 111 East Dunlap Avenue, Suite 1-291, Phoenix, Arizona 85020.
*Corresponding Author: Sharon M. Bates, Anthony Bates Foundation, 111 East Dunlap Avenue, Suite 1-291, Phoenix, Arizona 85020.
Citation: Sharon M. Bates. What Is a Young Life Worth? What Is My Life’s Work!. J Clinical Research and Reports, 5(4); DOI:10.31579/2690-1919/115
Copyright: © 2020 Sharon M. Bates. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 August 2020 | Accepted: 11 August 2020 | Published: 17 August 2020
Keywords: undiagnosed hypertrophic cardio- myopathy; heart palpitations-racing heart; fatigue; HCM; ECG
Life does not come with the instruction book, “How to Deal with the Death of a Child.” An- thony Bates was 20 years old when he died
July 31, 2000 from undiagnosed hypertrophic cardio- myopathy (HCM). Anthony, my only child, was a col- lege football player. Each year he was required to have a “pre-participation sports physical,” he had at least 20 in his life. Heart examinations were not included. Anthony’s HCM might have been detected if he had had an electrocardiogram (ECG) screening. Anthony never really complained of any symptoms. Sadly, his perfect health was an illusion.
It was 3 days after Anthony died that the coroner explained Anthony had HCM. We had no family his- tory, and Anthony had no symptoms that we were aware of at the time.
However, there was one complaint I remember. Dizziness! While filling out a sports physical ques- tionnaire in 1994, he asked me about the question, “It says—have you ever been dizzy?” He remembered, “When I jump up off the couch to answer the phone, I get dizzy.” “Well, that happens to me, too,” I replied. “It’s probably normal when you lie on the couch for hours and then jump-up.” So many times since, I’ve recalled that scene in my head.
Life does not come with the instruction book, “How to Deal with the Death of a Child.” An- thony Bates was 20 years old when he died
July 31, 2000 from undiagnosed hypertrophic cardio- myopathy (HCM). Anthony, my only child, was a col- lege football player. Each year he was required to have a “pre-participation sports physical,” he had at least 20 in his life. Heart examinations were not included. Anthony’s HCM might have been detected if he had had an electrocardiogram (ECG) screening. Anthony never really complained of any symptoms. Sadly, his perfect health was an illusion.
It was 3 days after Anthony died that the coroner explained Anthony had HCM. We had no family his- tory, and Anthony had no symptoms that we were aware of at the time.
However, there was one complaint I remember. Dizziness! While filling out a sports physical ques- tionnaire in 1994, he asked me about the question, “It says—have you ever been dizzy?” He remembered, “When I jump up off the couch to answer the phone, I get dizzy.” “Well, that happens to me, too,” I replied. “It’s probably normal when you lie on the couch for hours and then jump-up.” So many times since, I’ve recalled that scene in my head.
How can we put the symptoms of heart disease into a simpler form? Parents and children need to understand in simple terms that “dizziness-faint- ing, heart palpitations-racing heart, chest pains, or fatigue” are signs of a possible heart problem. These are also signs of being a teenager. Do we just ignore these signs, or screen everyone? Both examples have consequences.
To help with their grief after Anthony’s loss, I con- nected with the players, university employees, and coaches of Kansas State University. It was then I con- nected with Lisa Salberg, the President and Founder of the Hypertrophic Cardiomyopathy Association, to learn about the disease. Subsequently, I met Holly Morrell, Executive Director of A Heart for Sports, and now the founder of Heartfelt Cardiac Projects, who taught me a lot about heart screenings. She advocated for screening for youths, after losing 6 family mem- bers, cousins, uncles, and grandparents to HCM. Holly connected me to Arista, who had founded the Chad Foundation for Athletes and Artists after the loss of her son from HCM. Arista’s and Holly’s were the first community screening programs.
Linette Derminer lost her son to HCM, too, and she was keeping track of those stories in the media. Linette built the first database of these stories and the reasons given at death. Another mother, Rachel Moyer, connected us all. Rachel also lost her son to HCM. We were all advocating for the same things: better tracking of sudden cardiac death, automatic external defibrillators (AEDs) in schools; and heart screenings for children.
When I first discussed Holly and her screening program with Coach Bill Snyder, he said to me, “Sharon, you need to do the screenings. You have the story and the connection to K-State.” That is how the Anthony Bates Foundation (ABF) got started. The California screening Holly had hosted was big and exciting. Philips Medical was a sponsor and did a big media blitz, too. I learned about controlling the me- dia, screenings, echo stations, and the flow of par- ticipants. From the event experiences, I vowed to help as many people as I possibly could to create screenings in the United States. This was just the beginning. The second screening I attended was also in California. Our first several years of screenings
| FIGURE 1: ABF Overall Screened |
  |
| ABF ¼ Anthony Bates Foundatiozn; ECG ¼ electrocardiogram; PLT ¼ possibly life-threatening. |
were with ultrasound only. After 2006, we added ECGs for all participants screened. We found echo machines from the sales reps of several manufac- turers. With only 3 organizations hosting screenings in our country, the “ask” to borrow ultrasound equipment on the weekend was met with open arms. After that event over the first 5 years, we organized 17 heart screening events and screened 3,071 young hearts, finding 190 (6%) problems, with 60 (2%) of those screened to be possibly life-threatening prob- lems (Figure 1). In 2002, ABF became an official 501(c)(3). Subsequently, our moms team created our first collaborative organization, the National Coalition of Parent Network. We added 1 more mother, Laura Friend, to our network of influence. Laura’s daughter died in 2004 from HCM. All 4 of us grieving mothers traveled to Las Vegas in 2005 to meet with the Med- tronic Foundation and create what is today Parent Heart Watch (PHW). Then, with a small grant from the Medtronic Foundation, I created my first edition of “How to Host Community Cardiac Screening Events.” Screenings were beginning to grow, and I needed more cardiology support. There was an American Heart Association paper regarding screenings in Italy.
| FIGURE 2: ABF Teams’ Screening Numbers |
 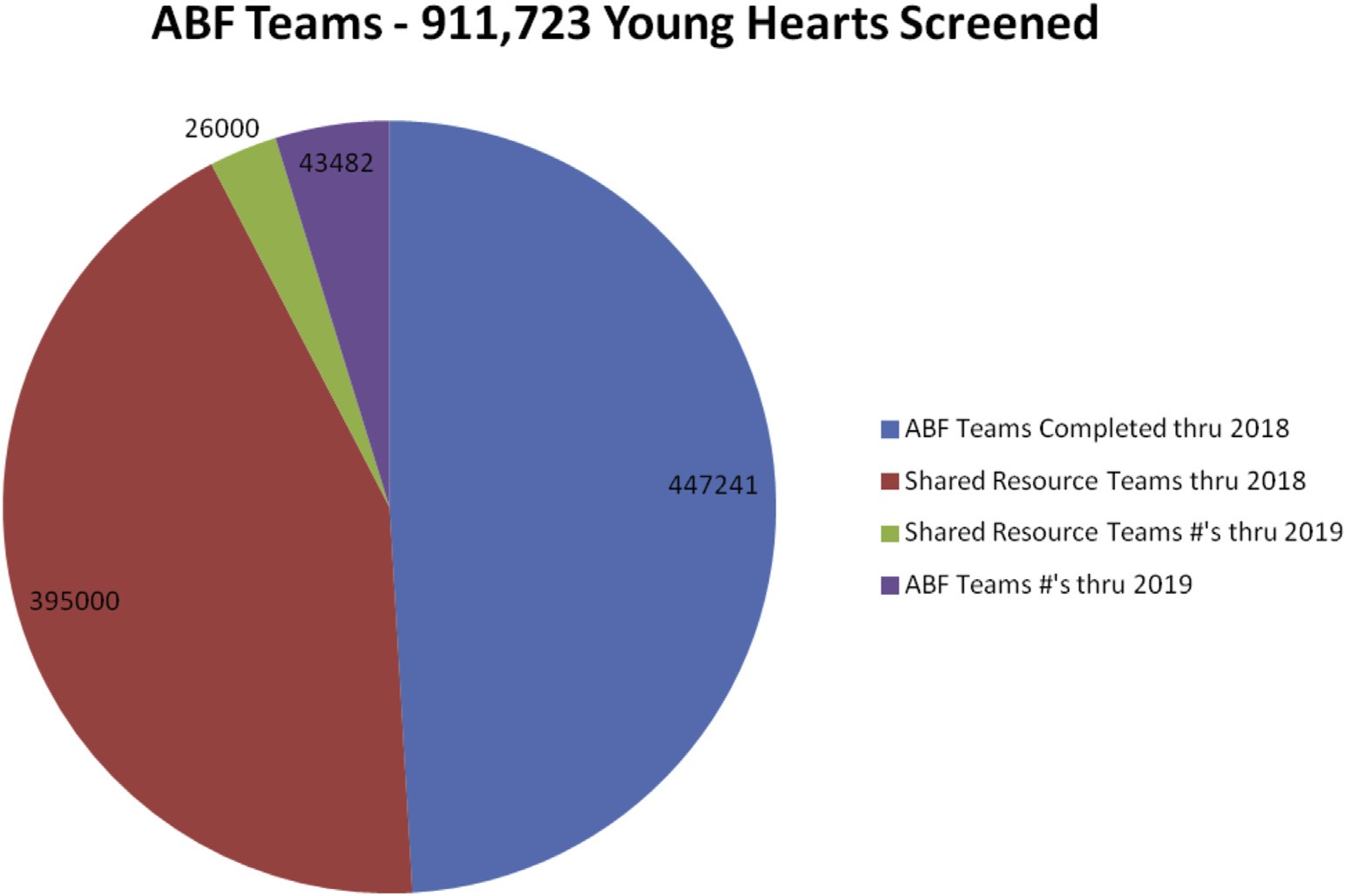 |
| ABF ¼ Anthony Bates Foundation. |
One of the authors was Dr. Antonio Pellicia. I emailed him asking for help to connect to other U.S. doctors. He replied within 24 h that as a “scientist” he did not know what he could do. I responded, “I’ll be in Rome on these dates, what works for you?” Before traveling to Rome, I invited 2 other European mothers, who had both lost sons to HCM. They shared my purpose and passion to help save more children’s lives from sudden cardiac death.
Dr. Pellicia was impressed with our ABF statistical screening numbers. They matched the findings in Italy. In 1984, Italy passed a law to screen all their athletes up to 35 years of age. They reduced the death rate by 89%. He shared a few names of U.S. doctors interested in heart screenings. Dr. Jon Drezner of the University of Washington and doctors at Stanford University were advocates for heart screening U.S. athletes. Unfortunately, according to Dr. Pellicia, many U.S. doctors had not accepted the Italian find- ings. It seems that modern medicine has its own roadblocks and politics.
PHW was a huge undertaking. Many of the parents who helped launched the group had no experience how to “run a Grassroots Movement,” but we perse- vered, as the effort was heartfelt and meaningful. We found and helped other parents who had lost children. The second version of the ABF Training Program was self-published in 2008, with the third version in 2014. This included a DVD of the process, a CD with all the digital documents, and a more comprehensive 150-page binder full of details.
PHW taught me a lot about AEDs in schools. That seemed a way to grab their attention. Not all schools had AEDs, and many were also resisting getting the equipment. Over time, the AED became a “standard of care” for the schools, and they were eager for funding sources. Screenings for AEDs were booming for a few years. By 2010, the economic downturn had slowed the effort of fundraising and heart screenings. By the end of 2014, I was able to retire from my contractor/ computer programming job and concentrate full time on screening, training, and placing AEDs.
Starting in June of 2015, summer interns started digitizing our database. The purpose of digitizing all the papers was to make the screening results clearer and more professional for research. We completed digitizing the papers by the summer of 2019. In early 2014, I approached the Cardiac Safety Research Consortium (CSRC) connected with Duke University.
From 2014 to 2017, I met with these doctors, researchers, and pharmaceutical partners in hopes to build a research network and funding source for the nonprofits doing the majority of screenings in the United States. Many of the researchers within the CSRC wanted “long-term studies.” During the 4 years I worked with the CSRC, there was no funding, no research, no white paper on screening position, and no cooperation. The new PHW leaders came on board and I stepped back.
In 2019, our intern, Martie Combs, DNP, MSN-Ed, RN, worked on her Doctorate of Nursing Practice project with the ABF data to improve the quality of our ECGs. She discovered a rate of artifact in our ECGs at 30%. Dr. Combs created an online course that we required our ABF volunteers to take when they work the ECG stations at our heart screening events. Through the ABF ECG Certification Training course, ABF volunteers were able to improve their electrode placement and reduce the artifacts on the ECG tracings by 25%. Our quality improvement course is available to our ABF teams. We hope to remove the “roadblock” in the medical community as it relates to “false positives” in screenings. The key to quality of tests is proper ECG electrode placement. I am proud to report that our 75 trained teams and teams with shared resources in the United States are hosting community heart screenings, with 2019 estimates of more than 911,000 (Figure 2).
The impacts of life’s unexpected events are truly immeasurable. It takes a village to save 1 life, and the whole country of ABF teams of screeners has amassed more than 18,000 lives saved and counting. The ABFtrained teams are training others, who, in turn, are training and empowering others.
We continue to “screen more young hearts and save more young lives.”
We will reach our 2020 goal to screen over 1 million hearts!
If you believe in our ABF mission, and if you believe that more children should and can be saved through proper heart screenings, then, will you join us to make a difference?
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
