
Research Article | DOI: https://doi.org/10.31579/2641-0427/023
*Corresponding Author: Badara Dembélé, Department of Orthopedic and Traumatology DANTEC Teaching Hospital Dakar Senegal
Citation: Dembélé.B., Mayaki A.H., Daffé M., Diouf. A.B., Dia. R., Sarr L. et al, (2020) Volleyball Technopaths in Senegal .J. Orthopaedics and Surgical Sports Medicine, 3(1): Doi: 10.31579/2641-0427/023
Copyright: © 2020 Dembélé. B, this is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 January 2020 | Accepted: 31 January 2020 | Published: 10 February 2020
Keywords: volleyball; technopaths; ankle sprains; anticipation; spectacular sources
Introduction
Sport anticipation, address and opposition in two separate spaces. Volleyball knows a frantic expansion with more and more spectacular gestures sources of various traumas. Our study is to analyse the trauma related to the volleyball game; relative to our context.
Patients and Methods
We collected 69 injuries from 63 licensed players of the Senegalese Volleyball Federation and who had regularly played the Championship and the National Cup for the 2016-2017 season. Data collection was carried out through a completed closed questionnaire.
Results
Forty (40) boys and twenty-three (23) girls, volleyball players, participated in this study. The average age was 23.6 years old. The average weight was 68.63 kg. The average height was 184.36 cm. The average age of the onset of the practice was 14.79 years. The average duration of practice was 8.67 years. The incidence of lesions was 1.84 per 1000 hours of play with 90.5% of players reporting injury. The 50.7% lesions were on the lower limb. Sprain accounted for 62.3% of the lesions; musculotendinous lesions 14.5% and bruises 11.6%. The majority of lesions, 53.6%, occurred during training. The net area was the site of 50.7% of the lesions. Physical contact accounted for 59.4% of the lesions. The balloon was involved in 33.3% of the lesions. The fall on the playground was responsible for 33.3% of the injuries. Receiving an opponent's weight on the ankle accounted for 76.06% of ankle sprains. The management was functional in 81.2%. It was satisfactory in 89.5%. The average rest period was 4.4 weeks.
Conclusion
Although considered a non-contact sport and therefore less virulent, relative to other team sports; volleyball is also a source of trauma. Beyond its originality to be realized in a sub-Saharan country; this study confirms the universality of the trauma related the volleyball, a sport that continues to take off.
Volleyball game is a sport of anticipation, skill and opposition in two separate spaces. His practice knows a frantic expansion with gestures more and more spectacular sources of various traumas. The majority of these injuries include sprained fingers and ankles in the foreground; occur around the net. Despite the extent of practice on the continent; African studies devoted to this subject are rare. Our study is to analyse the trauma related to the volleyball game; relative to our context.
1. Study material:
1.1. Framework of study:
He was represented by the two major volleyball competitions of the 2016 - 2017 season (National Championship and Volleyball National Cup) of the Senegalese Volleyball Federation.
1.2. Type of study:
This was a descriptive study for analytical purposes from March to April 2018 or 02 months.
1.3. The study population:
Players from three (3) senior clubs of the senegalese volleyball federation, men and women, who play in the national championship, have been targeted. Our players have been chosen from these clubs for two reasons:
2.1. Instrument:
As part of our research, we opted for an approach that relied on a survey. This approach was based on a single instrument: the questionnaire. We chose closed questions because they have a simplicity of data processing.
2.2. Production:
Players of the aforementioned clubs, holders of a license of the Senegalese Volleyball Federation; having played previously and regularly during the 2016 - 2017 season were selected for this study.
For the realization of this study we presented ourselves at the training places of the clubs to administer the questionnaire to the players for the clubs of ASC Police and DUC. As for the players of the UGB, we met them during a trip to Dakar as part of a national championship game.
Twenty-five (25) questionnaires were distributed in each club. This makes a total of seventy-five (75) questionnaires. Five (5) are lost and seven (7) insufficiently completed. What counts for our counting is a total of sixty-three (63) questionnaires, including twenty-three (23) girl players and forty (40) boy players.
2.3. Data Processing
Data entry was done on Word and Excel software. Statistical analysis was performed using SPSS20 software. The chi-square test was used to compare the data (significance threshold, p <0.05).
For each question asked in the survey, the results are tabulated or graphed.
1. Descriptive results:
1.1. Epidemiological data:
1.1.1. Depending on the genre:
Our study population consisted of sixty-three (63) volleyball players including twenty-three (23) women and forty (40) men representing a sex ratio of 1.73.
The figure below represents their distribution
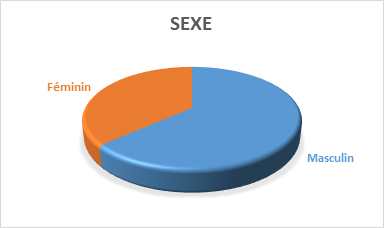
Sexe = Gender, Féminin = female, Masculin = Male)
Figure 1: Distribution by gender
1.1.2 According to age:
The average age was 23.6 years with extremes of 17 years and 38 years and a standard deviation of 3.79. The 21 to 25 age group was the most represented at 55.6%. The following table represents their distribution.

Table I: Distribution by age group
1.1.3. According to the weight:
The average weight of our population was 68.63 kg with extremes of 45 kg and 100 kg and a standard deviation of 11.20.
1.1.4. According to the height:
The average height was 184.36 cm with extremes of 160 cm and 202 cm and a standard deviation of 9.08.
1.1.5. According to the level of study:
The breakdown by level of study indicated that 84.1% of the players had a higher level; 12.7% secondary and primary level represented 3.4%.
The following table represents the level of study.

Table II: Distribution of patients by level of study
1.1.6. According to the profession:
The different professions occupied by our volleyball players are shown in the table below.
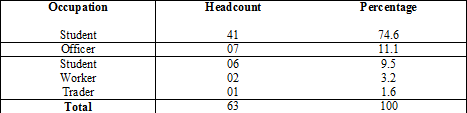
Table III: Distribution of patients by occupation
1.2. Sports data:
1.2.1. Age of beginning of practice:
The mean age of onset is 14.79 years with extremes of 9 years and 22 years and a standard deviation of 3, 14.
1.2.2. Average duration of practice:
The average practice duration was 8.67 years with extremes of 2 years and 28 years and a standard deviation of 4.56.
1.2.3. Game post:
Our population included 73% attackers; 15.9% smugglers and 11.1% of liberos.
The figure below represents their distribution.
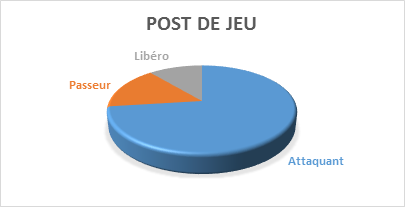
Figure 2: Distribution according to the game station
1.2.4. Level of practice:
All the players who participated in this study were semi-professionals.
They were all playing in the first division.
1.2.5. Duration of play:
The average hour per training session listed was 2.17 hours with extremes of 01 hour and 03 hours and a standard deviation of 0.45.
We found an average of 1.05 training sessions per day with extremes of 01 session and 02 sessions per day and a standard deviation of 0.21.
The average number of training days per week was 4.98 days with extremes of 03 days and 06 days.
The number of matches delivered per week was 01 match among all players.
1.2.6. Playground:
The type of hard ground (tarmac) was found in 100%.
1.2.7. Other sports practiced:
Apart from volleyball, 54% of the players did not practice any sport. In addition to volleyball; 17% of the players played football; 9.5% basketball; 4.8% handball and swimming 4.8%.
The table below represents their distribution.
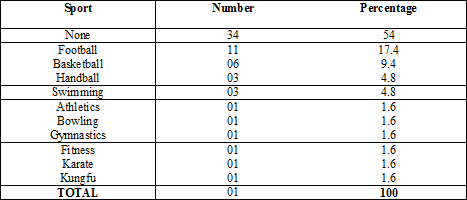
Table IV: Distribution by Other Sporting Disciplines
1.3. Lesional data:
13.1. Nature of the lesion:
All lesions reported in this study are acute.
1.3.2. Frequency of the injury:
The lesions were found in 90.5% of the players in our study population. The number of lesions per player averaged 1.23 with extremes of 01 and 02 lesions and a standard deviation of 0.42.
The following figure shows their distribution.
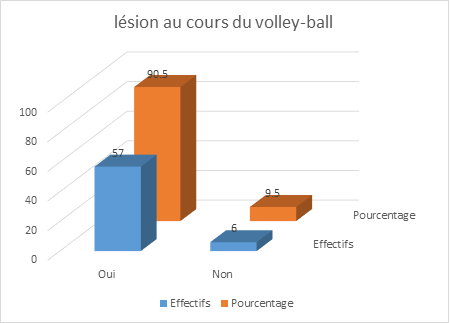
Figure 3: Distribution according to the frequency of the lesions
1.3.3. Injured segment:
50.7% of lesions sit on the pelvic segment against 39.1% for the thoracic segment. The ankle was the most affected followed by the hand with respectively 30.5% and 21.7%.
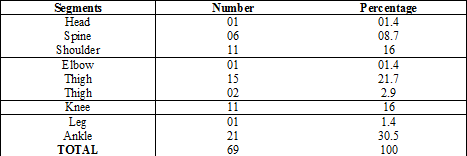
Table V: Distribution according to the injured segment
1.3.4. Type of lesion:
The sprain was reported in 62.3% of cases. It was more common in the ankle, ie 30.5%; followed by the fingers in 17.4% and the knee in 14.5% of cases. Of the eight (08) cases of contusion noted; the six (06) were on the lumbarregion. All elongation cases were at the shoulder level are 10.2%.

Table VI: Distribution by type of lesion
Capsulo-ligamentous lesions

Musculotendinous lesions

1.3.5. Time of injury:
Of the fifty-seven (57) players who suffered at least one injury; twenty-nine (29) affirmed to have injured themselves during the training period, ie 50.9%; twenty-one (21) during the competition i.e 36.8% and seven (7) in training and the competition i.e 12.3%.

Table VII: Distribution according to the time of occurrence of the lesion
1.3.6. Mechanisms and areas of injury occurrence:
Forty-one (41) of the injuries recorded (59.4%) were caused by physical contact with an opponent or teammate.
The fall with reception against the ground following a slip in 33.3% of the cases.
In twenty-three (23) cases the ball was challenged with "the counter or block" in twelve (12) cases during the "attack or smash" in seven (07) cases and the defense in four (04) cases.
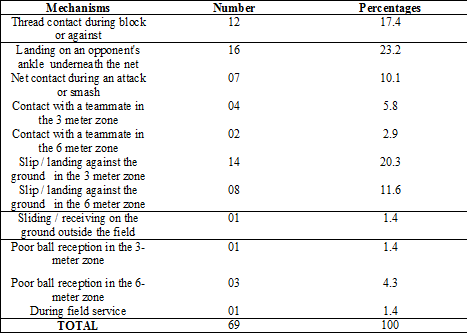
Table VIII: Distribution according to the mechanisms and the zone of occurrence of the lesion
1.4. Therapeutic data:
1.4.1. The existence of a medical staff:
Of the three (03) teams taking part in this study, only one has a medical staff. This medical staff is represented by a nurse who manages a staff of 21 players.
1.4.2. From the medical examination of aptitude:
No player has performed a fitness check before the start of the season.
1.4.3. Follow-up by the team during the injury:
Twenty-five (25) of the fifty-seven (57) players i.e 43.9%; having reported an injury during the game; assert to have been followed by their club.
1.4.4. Paraclinical assessment:
A paraclinical assessment summarizing by radiography of the injured segment was performed in 14% of cases.
1.4.5. Therapeutic methods:
The functional treatment that consisted of the establishment of a strapping and resting lesions was essentially observed. It was applied to fifty-six (56) lesions, ie 81.2%.
Surgical management by trimming, sutures and local care was recorded in 8.7% of cases.
Orthopedic treatment with two (02) boots and two (02) splint-boots i.e 5.8% was the third therapeutic method observed. This treatment is completed with rehabilitation in 3 patients.

Table IX: Distribution by type of treatment
1.4.6. Treatment results:
89.5% of injured players were satisfied with their management, compared to 10.5% who complained of chronic functional discomfort, including 02 knee sprains and 04 ankle sprains.
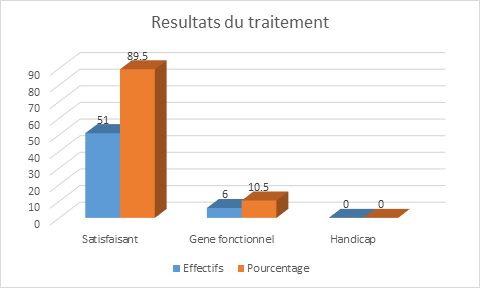
Figure 4: Distribution according to the result of the treatment
1.4.7. Rest time:
The rest time due to injury is shown in the table below. The average is 4.4 weeks with extremes of two (02) weeks and twelve (12) weeks.

Table X: Distribution by rest time
Due to its main character (two teams facing each other and separated by a net) Volleyball is long considered as a sport causing less trauma. If the world literature on the studies of its traumas would be summed up essentially with that of the West; in Africa it is almost impossible to find [18, 35]. In this context, it is imperative to report the African experience on the subject; because of the unbridled expansion of his practice on the continent.
These traumas related to the volleyball game concern all the musculoskeletal system and are grouped mainly in acute and chronic lesions or wear.
Our discussion will first focus on the general considerations of our study population, before addressing the links between certain parameters and the occurrence of these traumas related to the volleyball; the quality and results of their care.
Epidemiological data:
The average age was 23.6 years with extremes of 17 years and 38 years and a standard deviation of 3.79. The 21 to 25 age group was the most represented with 35 people (55.6%). Ben Ibn Abasse DIEDHIOU had noted an average age of 25.89 years in his series [7]. COLLET and COLL [16] reported an average age of 22.2 years for African-Caribbean volleyball players and 21.2 years for European volleyball players. With a proportion of 35%; T Puckree had a majority of "20-24" age groups in KwaZulu-Natal, South Africa [35]. As for Hung-Yu Huang; he had found an average age of 23.22 years in China [25].
It appears that our results are close to those of T Puckree in age group and those of Hung-Yu Huang in average age. On the other hand, our volleyball players are younger than those of Ben Ibn Abasse DIEDHIOU series but older than those of COLLET and COLL series.
The average height of the players in our serie is 184, 36 cm with extremes of 160 cm and 202 cm and a standard deviation of 9.08. This average is lower than that of Ben Ibn Abasse DIEDHIOU [7] and Hung-Yu Huang [40] who reported respectively an average of 187 cm and 187.06 cm. It is below that established by CARDINAL for a group of volleyball players considered to be elite, which is 191 cm [14]. It is also lower than the average height of the best teams in the world who participated in the "World League 2000"; which was greater than 195 cm [7].
The average weight of our population is 68.63 kg with extremes of 45 kg and 100 kg and a standard deviation of 11.20. Ben Ibn Abasse DIEDHIOU had reported in his serie an average weight of 75.86 kg for extremes of 61 kg and 93 kg [7]. As for Hung-Yu Huang and Anastasia Beneka [4] reported average values of 84 kg and 86.4 kg respectively.
Our result is far inferior to those of the literature [4,7,18]
Sports data
The average duration of practice is 8.67 years with extremes of 2 years and 28 years and a standard deviation of 4.56. Aagaard H, Jorgensen U [1] in their series had reported an experience of 10.6 years. Hung-Yu Huang had found an average of 11.67 years of experience. E M Verhagen et al [17] reported an average of 12.9 years.
It turns out that our players have less gaming experience than others.
The average hour per training session listed was 2.17 hours with extremes of 01 hour and 03 hours and a standard deviation of 0.45. We found an average of 1.05 training sessions per day with extremes of 01 session and 02 sessions per day and a standard deviation of 0.21. The average number of training days per week was 4.98 days with extremes of 03 days and 06 days. Also the average duration of training game per year would be (2.17 × 1.0 × 4.98 × 52); i.e 590 hours. Volleyball being a winning three-set open game, it is impossible to predict the duration of a match. Nevertheless, in our context an estimated time of one hour and a half was observed by the technical direction of the National Federation. Each player affirmed to play one game per week (1.5 × 52) corresponding to 78 hours of match play per year. In total, the average value of hours of play per year in our series would be (590 + 78) or 668 hours. R Augustsson had reported an average value of 31,972 hours among Swedish elite players[29].
All our players practiced on hard ground. Although we have not registered any; this could promote the occurrence of wear injuries including the different segments of the lower limb (knees and ankles) and the dorso-lumbar spine as demonstrated by the studies of Briner Ww [11] and Ferretti A et al [21] .
In addition to volleyball, 46% of players played at least one other sport. S. Augustsson found a proportion of 43% [34]. As for Ephrem Tamrat; he reported a proportion of 9.17% [18]. Aagaard H and collaborators reported a correlation between the practice of several sports disciplines and the occurrence of wear injuries in elite players [1].
3. Lesional data:
The majority of our players i.e 90.5% reported at least one lesion with an incidence of 1.23 lesions for 668 hours or 1.84 lesions per 1000 hours of exposure. Briner Ww in the United States had found 81.7% of injured volleyball players in a season [11]. T Puckree in South Africa had found 73% of volleyball players reporting at least one injury in one season [35]. Ephrem Tamrat in Ethiopia reported a proportion of injured players in the order of 17.22% with an incidence of 3.57 lesions per 1000 hours of exposure [18]. Anastasia Beneka in Greece found 46.4% injured volleyball players with an incidence of 2.4 lesions per 1000 hours [4]. S. R. Augustsson in Sweden found 52% of players who had a lesion with an incidence of 0.77 lesions for an exposure of 24,632 hours [34]. Schafle and al reported in their series an incidence of 2.3 lesions per 1000 hours of exposure in the United States [31]. Bahr R in his study found an incidence of 1.7 ± 0.2 per 1000 hours in Norway [6].
Yde J reported an incidence of 1.5 ± 0.2 per 1000 hours in Denmark [36]. Also in Denmark, Aagaard H reported an incidence of 3.8 lesions per 1000 hours of play [1]. In their series William W and al found a proportion of 81.7% of players reported injury in the United States [13]. Watkins and Green in Scotland reported a proportion of 53% injured players [37].
Although consisting of semi professional players and for the same duration of exposure; our incidence of lesion (1.84) broadly matches those reported in the literature as reported by Anastasia Beneka [4] or between 1.7 and 4.2 lesions per 1000 hours of exposure. However, the proportion of our players who have suffered a lesion is higher than those reported in the literature.
Recorded lesions; 50.7% were on the pelvic segment. Tamila AIT-Belkacem found a proportion of 51.3% of the lower limb. Aagaard H and al reported 51% lesions of the pelvic limb [2]. Ephrem Tamrat in his series reported a lesion proportion of 62.9% on the pelvic limb versus 37.1% on the thoracic limb [18]. Erin Cassell in a research study of injuries related to the practice of volleyball in Australia, reported 86.2% of lesions sitting on the lower limb [19]. Goodwin-Gerberich reported 90% lesions on the pelvic limb [23].
The predominance of lesions on the pelvic segment found in our study; joins those reported in the literature in varying proportions.
We found a predominance of ankle lesions followed by that of the hand in the proportions of 30.5% and 21.7%. Ankle sprain by forced supination is the most common traumatic injury in volleyball, representing 15 to 60% of acute injuries [6, 13, 19, 20, 27,31, 33,37].
With a value of 30.5% our result merges with those of the literature and close to that of T Puckree which brought 30% to KwaZulu-Natal in South Africa [35]. On the other hand, it is well below the 56.45% reported by Ephrem Tamrat in Ethiopia [16].
Among all sports, volleyball is by far the leading cause of digital trauma [5]. Lesions on the counter are more frequent in the competitors, while lesions on the receiving end are more likely to be recreational. The hand lesions recorded in our study represent 21.7%. Our lesional value of the hand is higher than that reported by T Puckree, lower than those of Ephrem Tamrat, Bhairo NH and Tamila AIT-Belkacem [10,27].
On the shoulder, the position of "arming the arm" and the striking force during the "pendulum" service may be responsible for antero-superior conflict, which is by far the most common technopathy. This pathology of the shoulder is linked to the repetition of movement [3]. We recorded 16% of lesions on the shoulder, consisting mainly of muscle damage (elongation and tearing) and all acute. Thus we found more shoulder lesions than Tamila AIT-Belkacem and Tamrat but less than T Puckree.
The knee may be the seat of (or especially) chronic lesions of repetitive use or acute traumatic ligament and / or meniscal lesions [3]. All knee injuries reported in this study were benign sprains. They accounted for 16% of the lesions recorded.
Our result is close to that of Briner and Bere 15% and 15.2%; higher than Talima, Bhar and Verhagen but lower than Puckree who had reported in addition to acute lesions 20%; chronic tendon diseases of the knee in his series [6,9,12,17,27,35].
The sprain represents 62.3% of our lesions followed by musculotendinous lesions with 14.5% and contusion at 11.6%. In this study we had no fracture or dislocation. However, as reported in the literature sprain was the first injury in the volleyball. With a value of 62.3% we reported fewer sprains than Talima AIT-Belkacem (75.7%); but more than Bere T (32.5%), Erin Cassell (46%); Ephrem Tamrat (46.78%) and Aagaard H (53.4%) [1,9,18,19,25,27].
Bere T reported a proportion of 14.1% of musculotendinous lesions. This value is close to ours, which was 14.5%. Erin Cassell and Tamila AIT-Belkacem respectively reported the proportions of 13.1% and 2.4%. These proportions are lower than our 14.5%. On the other hand, the 18.1% and 42.94% reported respectively by Aagaard H and Ephrem Tamrat are far superior to ours.
Our contusion rate of 11.6% is higher than that of Talima AIT-Belkacem which was 4.8% but lower than that reported by Bere T who reported 12.7%.
The majority of injuries occurred during training, 53.6% versus 46.4% during competitions. Several authors have reported a predominance of lesions during competitions [8, 22, 26, 28, 31]. Sibel KUCUK reported a predominance of lesions during training in the proportion of 62.1% [32]. S. R. Augustsson and al reported 47% of lesions that occurred during training, 41% of lesions that could not be specified, 7% injuries during competitions and 5% during warm-ups [34]. Christopher J. Sole and colleagues reported 75.2% of injuries that occurred during training; 20.2% injuries during competitions and 4.5% injuries during warm-ups [15].
We recorded more lesions during training than S.R. Augustsson and less than Sibel KUCUK and Christopher J. Sole.
Several studies have shown that the majority of acute volleyball injuries (finger sprains but especially ankles) occur at the net during the jump and landing; during physical contact and blocking gestures [1, 2, 6, 13, 6, 17, 21, 23, 31, 34, 37]. These authors reported proportions ranging from 52% [13] to 92% [23].
With values of 59.4% for the physical contact which incriminated in 76,06% of sprains of the ankle; our proportions are similar to those of literature.
The block and the attack were respectively reported in 17.4% and 10.1% of cases as vectors of lesions of the thoracic segment, particularly the fingers are in 27.5%. Six (06) studies in four (04) different volleyball populations; related to the mechanism of onset of lesions (Schafle and al., 1990 [31], Watkins & Green, 1992 [37], Bahr et al., 1995 [30], Bahr & Bahr, 1997 [6], Aagaard & Jorgensen, 1996 [1996]. 1], Aargaard et al., 1997 [2] noted that attack and blocking actions accounted for at least a quarter (25%) of volleyball injuries. Our proportion of 27.5% agrees with those of the aforementioned authors. These authors also reported that the defense on the playground would be associated between 6% -11% lesions and service between 2% - 4%. In our study defense accounted for 5.7% and service 1.4%. Our values are slightly lower than those reported in the literature.
Therapeutic data:
In this study the functional treatment was instituted in 81.2%. Bhairo NH and al reported 52% functional treatment. Solgard L and al. Reported in their series that 63% of lesions were managed outside the hospital [33]. In their study, Roald Bahr and al reported that 95% of lesions had "icing" as first aid [30].
Far below our result of 89.5%; Solgard L reported only 26% of volleyball players who were satisfied with the quality of their treatment [33]. However, he found unmet patients among those with ankle and knee injuries; which is also evident in this work.
During this work we found an average rest time of 4.4 weeks with extremes of two (02) weeks and twelve (12) weeks. This proportion is close to those reported by Bhairo NH [10] and EALM Verhagen [17] who reported an average of 04 weeks and 05 weeks, respectively.
The majority of volleyball players, ie 26.3%, had an absence duration of less than or equal to 02 weeks. These results are consistent with those of the literature through which several authors [1, 9, 13, 18, 24, 34] reported in proportions ranging from 24.5% to 85%; a duration of absence of 04 to 15 days.
According to the results reported in the literature [10, 30, 33]; functional treatment was by far the first therapeutic method in the management of acute lesions in volleyball as evidenced by our result (81.2%).
Volleyball is a game that opposes two (02) teams of six players on a field defined and shared by a net in two (02) playgrounds. It is one of the few collective sports that are practiced without there being any contact between the opponents. Renowned not traumatic, it is nevertheless provider of many traumatic pathologies; this especially as the techniques evolve in favor of a more spectacular game.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
