
Research | DOI: https://doi.org/10.31579/2693-4779/065
Naschitz, Bait Balev Nesher and the Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
*Corresponding Author: Jochanan E. Naschitz, Bait Balev Nesher and the Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: Jochanan E. Naschitz, N Zaigraykin, E Zlotover, F Neime. (2021) Vitamin K deficiency under enteral feeding: real or imagined threat. Clinical Research and Clinical Trials. 4(4); DOI: 10.31579/2693-4779/065
Copyright: © 2021 Jochanan E. Naschitz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 September 2021 | Accepted: 27 September 2021 | Published: 08 October 2021
Keywords: vitamin K; enteral nutrition; palliative care; prothrombin time; hemorrhage; bleeding
Patients receiving enteral feeding may develop vitamin K deficiency if the nutrition formula does not meet their daily vitamin K requirement. Vitamin K is essential for clotting factors II, VII, IX and X to be released in their functional form. Under vitamin K deficiency a coagulopathy may develop which is marked by prolongation of the prothrombin time (PT). There might be a need, unrecognized to-day, for monitoring the PT in patients receiving enteral feeding to unmask a latent coagulopathy. We assessed the prevalence of a prolonged PT in patients receiving enteral feeding for 3 months of more with one or a combination of the enteral formulas Osmolite®, Jevity®, Easymilk®. Twenty-three residents in long-term hospital care received solely enteral feeding for an average of 37 months, SD 21 months. The median daily vitamin K supplied by enteral feeding was 96.8 mcg (average 103.3 mcg, SD 28.8); this does not satisfy the 150 mcg of vitamin K required by the Food and Drug Administration. In 21 patients the PT-INR was 1-1.2 (normal). The PT was prolonged in two patients. In one of the latter, prolongation of PT-INR was not confirmed two days later. In the second case, the patient having repeatedly a PT-INR 1.4 (and a normal APTT), administration of vitamin K did not correct the PT. In conclusion, long-term vitamin K-deficient nutrition did not affect the vitamin K-dependent coagulation. This data may argue against the supposed need to monitor the PT in patients receiving long-term enteral nutrition.
Does vitamin K deficiency evolve under prolonged enteral feeding? This question was raised during a challenging clinical encounter. A 63-year-old man admitted to hospital with an ischemic stroke was diagnosed with a left ventricular mural thrombus. Enoxaparin treatment was started. Over 6 weeks there were two episodes of major hemorrhage needing brief discontinuation of anticoagulation. During this hospitalization a previously normal prothrombin time, PT-INR 1.02, became lengthened to 2.5. Intravenous administration of 10 mg vitamin K provided within 2 days normalization to PT-INR 1.1, upon which vitamin K deficiency was diagnosed [1]. Vitamin K deficiency in the patient was ascribed to enteral feeding with Osmolite® a formula which does not contain the daily requirement of vitamin K [2]. The patient was not receiving any medication known to interfere with vitamin K-dependent gamma-carboxylation of glutamic acid [3, 4] which may modify the PT.
Scrutiny of the literature provided no conclusive answers to the questions a) whether there is need for monitoring the PT in patients receiving enteral feeding, b) more so in patients receiving enteral feeding along with low molecular weight heparin or a direct oral anticoagulant, c) is there a need to fortify feeding formulas with vitamin K? [2, 5, 6]. We designed the present study in an attempt to address these issues.
Within the framework of a retrospective observational study approved by the Institutional Review Board data of routine coagulation tests were reviewed. Included in the study were 23 three residents of a department designed for long-term mechanical ventilation, those who were receiving enteral feeding for three months or longer. Excluded were residents eating by mouth, those who were supplementing enteral feeding with oral meals, and residents having had a bleeding event during a 28-day period before the coagulation tests were taken. Demographical and clinical patient data were searched in the electronic data base: age, gender, length of stay in the ward, length of enteral feeding, brand of enteral formula, content of vitamin K in the enteral formula, minor and major bleeding events, coagulopathy, bariatric surgery, chronic diarrhea, arterial hypertension, ischemic heart disease, congestive heart failure, diabetes mellitus, COPD, cancer, liver disease, antiphospholipid antibody syndrome, systemic lupus erythematosus, tracheostomy, mechanical ventilation, use of anticoagulant medication. The following enteral feeding formulas were in use: Osmolite HT® (Abbott nutrition, USA) which contains 61 mcg/L vitamin K, Jevity® (Abbott nutrition, USA) containing 61 mcg/L vitamin K, Easymeal-k2® (Easyline, Israel) containing 110 mcg/L vitamin K. The vitamin K supplied daily by enteral feeding was calculated and referred to the FDA recommended dose [2].
The PT-INR and APTT were assessed according to the standard method [7] with PT-INR in the range 1 to 1.2 is accepted as normal. When the PT-INR was >1.2 and confirmed on a second examination, the patient's data were reviewed for possible cause of hypoprothrombinemia: liver disease, chronic bleeding disorder, malabsorption, diet low in vitamin K, disseminated intravascular coagulation, medications interfering with vitamin K activity. If neither was detected, a single dose of 10 mg vitamin K1 was administered by feeding tube and the PT-INR was reassessed 72 hours later. If the PT-INR was not corrected the procedure was repeated. The prevalence of a prolonged PT-INR (>1.2) correctable by administration of vitamin K was assessed and related to the patients’ clinical background and daily vitamin K supplied.
Twenty-three patients constitute the study cohort (Table 1).
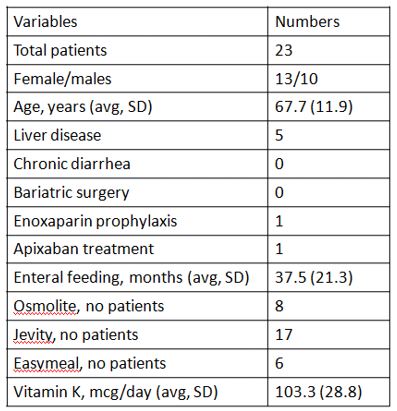
There were 13 women and 10 men, median age 68 years, all having failed to be weaned from mechanical ventilation. Enteral feeding was supplied by gastrostomy. The diagnoses, more than two in each patient, were: unaware wakefulness state in 16 patients (following anoxic brain damage or traumatic brain injury), cerebrovascular accident 7, neurodegenerative disorder 5, diabetes mellitus 8, arterial hypertension 12, ischemic heart disease 6, chronic obstructive lung disease 2, chronic liver disease 5 (in all cases asymptomatic), rheumatoid arthritis 1, cancer in 1 patient. The median length of hospitalization in our ward was 36 months. Bleeding events during hospitalization in our ward were minor bleeding events (BARC type 2) witnessed in 9 patients (epistaxis, mild hemoptysis, colostomy related maceration of the skin) and major gastrointestinal hemorrhage (BARC type 3a) in one patient [8].
Enteral feeding consisted of one or a combination of the following: Jevity in 17 patients, Osmolite HT in 8 patients, and Easymeal in 6 patients. The median daily vitamin K supplied by enteral feeding was 96.8 mcg (average 103.3 mcg, SD 28.8), that is less than the FDA recommended minimum of daily 150 mcg [2]. There were two exceptions, one patient received 169 mcg vitamin K/day and another 176 mcg vitamin K/day.
In 21 patients the PT-INR was 1 - 1.2 (normal); it was prolonged in two patients. In one of the latter, prolongation of the PT-INR was not confirmed on duplicating the test 3 days later without having supplemented vitamin K. In the other case, the patient having repeatedly PT-INR 1.4 and normal APTT, administration of vitamin K did not correct the PT; this patient had no features of systemic lupus erythematosus, other rheumatic disorders, or malabsorption. He was not receiving any medication known to cause hypoprothrombinemia [3,4]. A prolonged PT which was not correctable by administration of vitamin K could not be attributed to vitamin K deficiency. The patient’s general condition did not allow for a detailed work-up of other possible causes of prolonged PT.
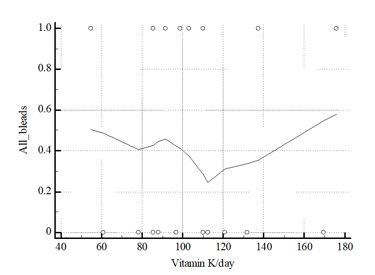
In the patients of this study there was no correlation between the daily total vitamin K supplied by enteral feeding and occurrence of bleedings (Figure 1).
Vitamin K is obtained from green vegetables contained in the food and by bacterial synthesis in the gut. Vitamin K deficiency arises when the vitamin K content in the diet is persistently low or when the absorption of vitamin K is defective. The latter occurs in obstructive jaundice where bile cannot reach the duodenum [9], as well as after bariatric surgery [10]. Patients receiving enteral nutrition or total parenteral nutrition if it is not adequately fortified with vitamin K may develop vitamin K deficiency [5]. The requirements of the Food and Drug Administration for an effective adult parenteral multivitamin drug product specify addition of 150 microg of vitamin K [2]. However, according to a dedicated study, none of 62 nutritionally complete enteral formulas contained the daily vitamin K requirements [3]. Neither did the enteral formulas the patients were receiving in our study.
The PT is a single-stage coagulation screening test for extrinsic and common pathways. An abnormally long PT is caused either by low plasma levels of one or several of coagulation factors II, V, VII, X and fibrinogen, or by inhibitors against these factors [7]. Vitamin K is essential for the posttranslational gammacarboxylation of clotting factors II, VII, IX and X (and the natural anticoagulants protein C and protein S); in the absence of vitamin K these factors are released from the liver in a non-functional form. As a result, the PT is prolonged. On this basis the PT is used as an indicator of the vitamin K status. At present, the dietary recommendations for vitamin K intake are based on the dose required to prevent bleeding. Indeed, the importance of vitamin K for hemostasis is determined by the fact that vitamin K deficiency may cause life-threatening bleeding.
However, the physiological roles of vitamin K are numerous, widely beyond synthesis of coagulation factors. So, vitamin K carboxylates osteocalcin which is important in transporting calcium to bone. Vitamin K activates matrix Gla protein an inhibitor of vascular calcification. Vitamin K carboxylates Gas6 protein which is protective against cognitive decline and neurodegeneration. Vitamin K exerts antiproliferative, proapoptotic, autophagic effects and has been associated with a reduced risk of cancer [11, 12]. While conventional recommendations are based on the dose of vitamin K required for preventing bleeding, there is a call to provide higher doses of vitamin K for the benefit of several chronic conditions, especially among elderly people [11].
Vitamin K is poorly retained in the body. Studies with [3H]-labeled phylloquinone indicated that 60–70% of doses in the range of 45–1000 microgram of vitamin K1 were excreted within 5 days (6). Patients of the present study, by receiving enteral nutrition deficient in vitamin K and no other supplements of vitamin were most likely in a vitamin K deficient state. Yet their PT-INR did not signal a coagulopathy. The dissociation between a deficient bodily vitamin K status and the normal PT might be explained by the “triage theory” which states that during a poor dietary supply vitamins are preferentially utilized for functions which are essential for immediate survival (12); such is synthesis of coagulation proteins. Hence, the PT is not a sensitive indicator of the body's vitamin K status. Ideally, undercarboxylated prothrombin (Protein Induced by Vitamin K Absence/antagonism, PIVKA-II) is used as an accurate indicator of the hepatic vitamin K status [13, 14].
In our study the PT-INR correlated neither with the history of bleeding nor with the deficient vitamin K status assumed to exist. Accordingly, monitoring the PT-INR in patients receiving enteral nutrition does not appear to be practical for preventing bleeding. Rather, fortifying feeding formulas with higher doses of vitamin K might be useful in virtue of the numerous beneficial effects of this vitamin.
There are limitations to our study related to the small number of patients assessed, the study cross-sectional design, and unavailability of high-sensitivity vitamin K assays. The strength of the study consists in recruiting the most severe patients, long duration of enteral feeding, accurate and prolonged medical observation, and the confident assessment of vitamin K supplied.
Long-term vitamin K-deficient enteral nutrition did not affect the vitamin K-dependent coagulation. This data argues against the need monitoring the PT in patients receiving long-term enteral nutrition.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
