
Research Article | DOI: https://doi.org/10.31579/2643-6612/029
1 Department of Oral and Maxillofacial Surgery, Leiden University Medical Center, Leiden, the Netherlands.
2 Mathematical Institute, Leiden University, Niels Bohrweg 1, 2333 CA Leiden, the Netherlands.
3 Medical Statistics, Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, the Netherlands.
4 Department of Oral and Maxillofacial Surgery, Amphia Hospital, Breda, the Netherlands.
*Corresponding Author: JP Richard van Merkesteyn, Department of Oral and Maxillofacial Surgery, Leiden University Medical Center, Leiden, the Netherlands.
Citation: Jeroen G van Rijsse, Jop P Verweij, M Fiocco, G Mensink, J P Richard van Merkesteyn. (2022). Visible Soft Tissue Contour Change of the Mandible Associated with Osseous Inferior Mandibular Border Defects after BSSO. Dentistry and Oral Maxillofacial Surgery. 5(2); DOI: 10.31579/2643-6612/029
Copyright: © 2022 JP Richard van Merkesteyn, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 December 2021 | Accepted: 02 February 2022 | Published: 18 February 2022
Keywords: sagittal split; osteotomy; orthognathic; complication; inferior border
Purpose: Visible soft tissue contour changes of the mandibular inferior border can cause an unaesthetic outcome after bilateral sagittal split osteotomy (BSSO). In some cases, even secondary reconstruction of the mandibular inferior border is needed. The aim of this study was to determine the percentage of unwanted visible contour changes of the inferior mandibular border after BSSO. The impact of potential risk factors for the outcome of interest were also assessed.
Methods: In this retrospective study, consecutive patients who underwent mandibular advancement through BSSO were included. The primary outcome parameter was the presence/absence of a visible contour change at the inferior border of the mandible one year after BSSO. Risk factors of interest included the presence of a radiographic osseous inferior border defect, the amount of mandibular movement, rotation of the occlusal plane, postoperative proximal segment position, pattern of lingual fracture, occurrence of bad split, and presence of third molars during BSSO.
Results: The study sample consisted of 147 patients with a mean follow-up of 13.2 months. A visible contour change was present in 2% of patients (1% of sagittal splits). No secondary reconstructive procedures were performed. A bony defect (osseous inferior border defect) was present in 7% of the sagittal splits. There was a significant association between a visible contour change of the mandibular border and an osseous inferior border defect (p <0.001). None of the other risk factors in this study showed a significant association with soft tissue contour changes.
Conclusion: Visible contour changes of the inferior border of the mandible are a rare complication after BSSO. Osseous inferior border defects of the mandible are a significant risk factor for soft tissue changes.
Bilateral sagittal split osteotomy (BSSO) for mandibular advancement is a procedure that is widely used to treat patients with a class II malocclusion. Well-known complications are bad splits, damage to the inferior alveolar nerve and postoperative infection. (Jop P Verweij et al., 2016). A much less known complication after BSSO is a visible soft tissue contour change located at the inferior border of the mandible (Figure. 1) (Wolford, 2015), (Agbaje et al., 2013)(Agbaje et al., 2016), (Bouwman et al., 1995). Such a contour change can cause an aesthetically unpleasing result of BSSO that could even necessitate secondary reconstruction of the mandibular inferior border in some cases (Agbaje et al., 2013), (J P Verweij et al., 2017).
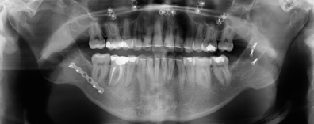
Most authors hypothesize that a visible contour change is caused by a persistent osseous defect of the inferior border of the mandible after BSSO (Figure. 2). These osseous inferior border defects are present in 5.1-36.5% of the sagittal splits one year after BSSO (Agbaje et al., 2013)(Agbaje et al., 2016)(J P Verweij et al., 2017). Known risk factors for these persistent osseous defects of the inferior border include a large mandibular advancement, a large rotation of the occlusal plane, cranial rotation of the proximal segment, and splitting the full thickness of the inferior cortex (Agbaje et al., 2013)(Agbaje et al., 2016)(J P Verweij et al., 2017). However, to our knowledge, no reports are present regarding the association between visible contour changes and osseous inferior border defects. It is unclear in how many percent of cases an osseous defect leads to a visible contour change at the inferior border of the mandible.
The purpose of this study is to determine the incidence of a clinically visible contour change of the inferior mandibular border after BSSO and analyze the association between bony defects and visible contour changes. Possible risk factors for soft tissue contour changes after BSSO are furthermore analyzed.



Study design and inclusion/exclusion criteria
A retrospective cohort study was implemented. The records of consecutive patients who underwent BSSO or a bimaxillary procedure with or without genioplasty to correct a class II malocclusion (mandibular advancement) were reviewed. All patients that received treatment between July 2006 and March 2015 at the department of Oral and Maxillofacial Surgery of the Leiden University Medical Center were included. Patients that received bilateral sagittal split osteotomy to correct a class III malocclusion (mandibular set-back) were not included. Patients were excluded if the follow-up was less than 6 months, if not all radiographs or clinical photographs were present, or if the contour of the mandible could not be assessed by inspection (for example because of a beard).
Variables of interest
The primary outcome of interest in this study was the presence/absence of a visible contour change at the lower border of the mandible after BSSO. A contour change was defined as a deformation of the soft tissue of the inferior border of the mandible, located near the caudal end of the vertical osteotomy site. This was categorized in three groups: (1) no visible contour change; (2) dubious contour change; (3) an evidently visible contour change. Only for group 3, soft tissue contour changes were defined as ‘present’.
Furthermore, a set of specific predictor variables was used to investigate risk factors for visible contour changes at the lower mandibular border. The presence of osseous inferior border defects was defined as a defect in the inferior cortex of the mandible of more than one cortical thickness measured at the osteotomy site. Other predictor variables included presence/absence of third molars during surgery, the occurrence of bad splits, the amount of mandibular movement (mm), the rotation of the occlusal plane (degrees), the postoperative position of the proximal segment, and the pattern of the lingual fracture. The postoperative position of the proximal segment was defined as either a good anatomical position without proximal segment rotation, a slight rotation of the proximal segment (less than one cortex thickness), or significant rotation of the proximal segment (more than one cortex thickness). The lingual fracture pattern was defined as either a type I or type II split. A type I split consisted of a split where the inferior border had split with caudal cortex on both the proximal and distal segment. A type II split consisted of a split that did not run through the caudal cortex, but started in the lingual cortex (including the full thickness of the inferior border), keeping the complete bilateral caudal cortex attached to the proximal segment (J P Verweij et al., 2017).
Data collection
Clinical photographs were taken by a professional medical photographer under standardized conditions before surgery, 6 and 12 months after BSSO. To detect a contour change of the inferior border of the mandible, the postoperative clinical photographs that were taken minimally 6 months after BSSO were analyzed and compared with the preoperative clinical photographs. The defects were diagnosed by one observer and confirmed by two other oral and maxillofacial surgeons.
The occurrence of osseous inferior border defects was analyzed using preoperative radiographs and postoperative radiographs (orthopantomographic images) acquired at the latest follow-up (minimally 6 months after BSSO). A tangential line to the inferior mandibular border was visualized to assess whether a contour change was present near the vertical osteotomy site. This contour change of the inferior mandibular border was measured relative to the thickness of the inferior cortex (i.e., more or less than one cortical thickness) (6).
The presence of third molars and occurrence of bad splits was recorded intra-operatively by the surgeon and noted in the surgical report. The amount of mandibular advancement and rotation of the occlusal plane were calculated after performing cephalometric measurements using the preoperative and postoperative lateral cephalogram. The postoperative proximal segment position was analyzed using the panoramic radiographs or cone-beam computed tomographic images that were performed one week after surgery. The type of split was also analyzed using these images.
The study was performed in accordance with the guidelines of our institution and followed the Declaration of Helsinki on medical protocols and ethics. Because of the retrospective nature of this study, it was granted an exemption by the Leiden University Medical Center institutional review board.
Surgical protocol
BSSO was performed according to the Hunsuck modification (Hunsuck, 1968) using a splitter (Smith Ramus Separator 12 mm, Walter Lorentz Surgical, Jacksonville, FL, USA) and separators (Smith Sagittal Split Separators, curved, Walter Lorentz Surgical, Jacksonville, FL, USA). Six oral and maxillofacial surgeons supervising a resident on the contralateral side used the same surgical technique and surgical protocols, as reported in previous papers (Merkesteyn et al., 2007)(Mensink et al., 2012).
After incision of the mucoperiosteum and exposition of the mandbular bone, the horizontal osteotomy was placed just above the mandibular foramen. The sagittal osteotomy was placed over the anterior side of the ramus ascendence to the distal border of the second molar. The vertical osteotomy was placed just posterior of the second molar, perpendicular to the inferior border of the mandible. An inferior border cut was made completely through the inferior cortex, reaching into the lingual cortex.
The split was performed using splitter and separators. The splitter was placed in the sagittal osteotomy and the separator in the verical osteotomy, in order to guide the split. After a succesful split, the distal segment was placed in the planned position using an intermaxillary wafer. The proximal segment was placed in position using a Luniatschek to secure the condyle in to the mandibular fossa. Simultaneously, the inferior border was palpated to align the inferior border of the distal and proximal segment. Rigid fixation was performed by three bicortical screws.
Follow up included standardized clinical and radiological evaluation and took place at 1 week, 1, 6 and 12 months postoperatively.
Statistical methods
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS version 23.0 for Mac, IBM, Armonk, NY, USA). Patient characteristics and surgical specifics were reported. To study the association between risk factors and soft tissue defects, generalized linear mixed models (GLMM)(Jiang, 2007) were employed to account for the correlated nature of the data (repeated measurements design consisting of right and left side within one patient). To analyze the association between the presence of a visible soft tissue defect and an osseous inferior border defect the chi-squared test was used.
The medical records of 219 patients, who underwent BSSO-advancement were investigated. Of these patients, 147 could be included in the study. Exclusion was performed because of follow-up of less than six months (10 patients), incomplete radiographs (9 patients) or incomplete or incorrect clinical photographs (53). The mean follow-up time was 398 days (SD 138 days; range 163 - 1164 days). Table 1 shows the patient characteristics.

* Data are represented as number of sites (%).
In the 147 included patients (294 sagittal split sites), the mean mandibular advancement was 5.7mm (range 1-11mm). Third molars were present during the sagittal split in 126 sites (42.9%) and absent in 168 sites (57.1%). Bad splits occured in 8 out of 294 sites (2,7% per site). No bilateral bad splits occurred. Postoperative radiographs showed a significant rotation of the proximal segment in 9 sagittal split sites (3%). Minimal rotation (less than one cortex thickness) was present in 86 sagittal split sites (29.3%). In 199 sides (67,7%) there was no rotatation of the proximal segment. After 257 sagittal splits (87.4%), a type 1 split was present and after 37 sagittal splits (12.6) a type 2 split including the full thickness of the inferior border was present.
An osseous mandibular border defect was present in 21 sagittal split sites (7.1%). Visible contour changes of the soft tissue at the inferior border of the mandible were present in 3 sides (1.0%). An osseous inferior border defect was present in the radiographs of these clinically visible soft tissue contour changers in all 3 patients. In 14,29% of the patients with an osseous mandibular border defect a visible contour change was seen. Table 2 shows the evaluation of soft tissue contour changes.
GLMM were used to study the association between predictor variables and visible contour changes of the inferior mandibular border. There was a statistically significant association between radiographically diagnosed osseous inferior border defects and clinically visible soft tissue contour changes (p lessthan 0.001). No significant associations were recorded for the presence of third molars, the presence of bad splits, the amount of mandibular movement, the rotation of the occlusal plane, the postoperative position of the proximal segment, and the pattern of the lingual fracture with the outcome.

The purpose of this study was to estimate the percentage of a visible contour change of the inferior border of the mandible after BSSO. We furthermore analyzed the association between a clinically visible contour change of the mandible and an osseous inferior border defect and evaluated possible risk factors associated with this clinically visible contour change.
In our study group of 147 patients, a visible contour change after bsso was present in 2% of the patients and 1% of the surgical sides. There was a significant association between the visible contour change of the inferior border of the mandible and an osseous inferior border defect (p lessthan 0.001). No other significant risk factors could be found in this study.
In the current available literature, there is little information available about the incidence of a visible contour change of the inferior border of the mandible after BSSO advancement. Even though many authors have described the contour change as a complication after BSSO, which sometimes can even necessitate secondary reconstruction using bone products or allogeneic implants(Agbaje et al., 2013)(Bouwman et al., 1995)(J P Verweij et al., 2017)(Wolford, 2015). Few studies describe the osseous inferior border defect as a possible cause of a visible contour change, but a correlation was never investigated (Agbaje et al., 2013)(Agbaje et al., 2016)(J P Verweij et al., 2017). In comparison to the osseous inferior border defect, which is present in 5.1-36 percent of the operation sides after BSSO, a visible contour change is quite rare (1-2%).
This is most likely explained by the fact that an osseous inferior border defect is covered by soft tissue that hides the contour changes in most of the cases. Subcutaneous fat can for example fill up the osseous defect. In the older population, the jowl fat pads move caudally towards the inferior border of the mandible and can hide the osseous defect even more (Reece & Rohrich, 2008). In this study group, the vertical osteotomy was placed behind the second molar, and therefore also the masseter muscle could cover the osseous defect, which is typically located near the vertical osteotomy (J P Verweij et al., 2017)(Jop P. Verweij et al., 2015). Possibly an elevated prevalence of visible contour changes of the inferior border of the mandible can be detected after BSSO, when the vertical osteotomy is placed more anteriorly. To enlarge the covering effect of the masseter muscle, Verweij et al. suggested the angled osteotomy concept, where the vertical osteotomy and the inferior border cut is placed more posteriorly (near the masseteric tuberosity). Using this technique, the masseter muscle probably could mask even more of the osseous inferior border defects, but we should notice this study was performed on cadaveric mandibles, so the results must be extrapolated to the clinical setting carefully.
Previous research has identified significant risk factors for osseous inferior border defects in radiographs, including: the amount of advancement, rotation of the occlusal plane, rotation of the proximal segment and whether or not the full thickness of the inferior cortex was completely attached to the proximal mandibular segment (Agbaje et al., 2013)(Agbaje et al., 2016)(J P Verweij et al., 2017). In this study, no significant risk factors (other than the present of an osseous inferior border defect) could be identified for clinically visible inferior border defects or contour changes. This is possibly caused by the low incidence of a visible contour change. Since there is a significant correlation between the osseous defect and a visible contour change, we would expect the same risk factors are valid for a visible contour change, however in this population that could not be proven.
Because of the association between the osseous inferior border defect and a visible contour change, most of the treatment options are aimed at preventing osseous inferior border defects. Wolford et al. and Agbaje et al. described an inferior border osteotomy to perform a split situated in the inferior border to create a continuous inferior border after the advancement (Wolford et al., 1990)(Agbaje et al., 2016). Other authors suggest using bone substitute as grafting material at the osteotomy site in patients treated with large mandibular advancements (>8mm) (Trevisiol et al., 2012)(Raffaini et al., 2020). However, to our knowledge, no reports are present in the current literature that show a lower incidence of visible mandibular border defects after bone grafting during BSSO.
In our clinical experience, visible contour changes are rare after bsso, and even if a contour change is visible, correction is not often necessary. However, when a visible contour change is present after BSSO, the defect can be treated by secondary reconstruction. A possible option is to place bone products or allogeneic implants to fill up the osseous defect and support the soft tissue to improve the visible contour (Agbaje et al., 2013)(J P Verweij et al., 2017)(Wolford, 2015).
We believe our findings represent a reliable estimate of the incidence of soft tissue contour changes in a relatively large group of patients. Some aspects of this retrospective study need to be addressed. The retrospective character of the study and exclusion of 72 patients (because of incomplete data, lack of follow-up or incorrect photographs) is a disadvantage. Several male patients had to be excluded because of wearing a beard and a few female patients had to be excluded because their hair made assessment of the mandible using photographs impossible. There were no remarkable differences between the excluded patient group and our study group, so we therefore do not believe that exclusion influenced any of the results. Clinical inferior border defects were assessed using pre- and postoperative clinical standardized photographs. Although clinical assessment is preferred, we believe this offered a reliable detection method without causing discomfort to patients. All photographs were performed under standardized conditions by a professional medical photographer. Nevertheless, this study simply offers an estimation of the incidence of clinically visible soft tissue contour changes after BSSO. Further research is required to confirm our findings, ideally in a prospective study design including physical examination.
The percentage of a visible contour change of the inferior border of the mandible after BSSO in the present study was found to be 2% per patient and 1% per surgical side. There was a significant association between a visible contour change of the mandible and an osseous inferior border defect (p less than 0.001), however in most cases the osseous defect did not lead to a visible contour change. These findings could help surgeons to estimate the risk developing a visible contour change of the mandible after BSSO.
The authors declare that there are no conflicts of interest in this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
