
Case Report | DOI: https://doi.org/10.31579/2690-1897/117
* Department of General, Oncologic and Vascular Surgery Hospital Riuniti Marche Nord Pesaro, Piazzale Cinelli n.4, 61121 PU Italy.
*Corresponding Author: Irene Fiume, Department of General, Oncologic and Vascular Surgery Hospital Riuniti Marche Nord Pesaro, Piazzale Cinelli n.4, 61121 PU Italy. E-mail: irene.fiume@virgilio.it
Citation: Irene Fiume. (2022) Vermiform Appendix Incarcerated in Spigelian Aponevrosis Defect (VAISAD hernia) J. Surgical Case Reports and Images 5(4); DOI: 10.31579/2690-1897/117
Copyright: © 2021, Irene Fiume, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 May 2022 | Accepted: 30 June 2022 | Published: 07 July 2022
Keywords: spigelian hernia; vermiform appendix; chronic appendicitis; appendectomy; laparoscopic intraperitoneal onlay mesh repair
Spigelian hernia (SH) is infrequent accounting less than 2% of all abdominal hernias. The presence of vermiform appendix within the hernial sac is of further peculiarity. While the authors who first described inguinal hernia containing the appendix (Amiand’s hernia) and femoral hernia containing the appendix (De Garengeot’s hernia) are well known and their name was given to the disease, SH containing the vermiform appendix has no specific name.
This study provides a literature search on this topic and a review of the available case reports is conducted. A description of a clinical case of an incarcerated SH in which the vermiform appendix was located within the hernial sac is presented with attached the video of its mini-invasive surgical treatment.
Based on literature findings, an attempt is made to give a specific name to this condition (Vermiform Appendix Incarcerated in Spigelian Aponevrosis Defect) using the acronym VAISAD hernia, in such a way so that it can be specifically and easily searched. Moreover, a classification of its severity and related complications, similarly to what was done for Amiand’s hernia, is carried out in order to establish the optimal approach in the surgical treatment case by case.
Spigelian hernia (SH) is the protrusion of the abdominal content or peritoneum through a congenital or acquired defect of the anterior abdominal wall fascia in correspondence of the Spigelian aponeurosis, along the semilunar line. Mostly, these hernias lie in the SH belt [1] in which, the weakest area is at the intersection between the semilunar and semicircular line, as the posterior rectus sheath is no longer present. The “weak triangular area” is delimited laterally by the semilunar line, superiorly by the semicircular line and, inferiorly, by the deep inferior epigastric vessels [1], above the Hesselbach’s triangle. A representation of the SH site is shown in the figure 1.
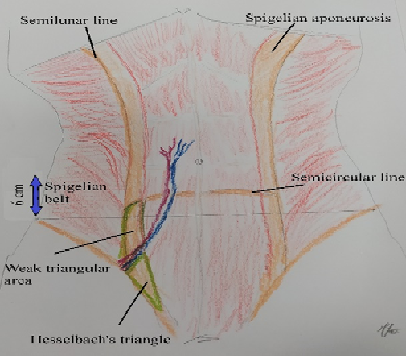
Anatomical definitions
Spigelian aponeurosis: part of the aponeurosis of the transverse abdominal muscle between the linea semilunaris laterally and the lateral edge of the rectus muscle medially.
Linea semilunaris: a vertical, curved structure that runs along the lateral edges of the rectus abdominis muscle in the anterior abdominal wall. It is the site of the union where the tendons of the lateral abdominal muscles (the external oblique, the internal oblique and the transversus abdominis muscles) meet the sheath surrounding the rectus abdominis muscle, also known as the rectus sheath. Linea semilunaris runs between the cartilage of the ninth rib and the pubic tubercle bilaterally. The ninth ribs are farther apart from each other when compared to the pubic tubercles, which are closer together, giving the linea semilunaris its curved shape [2].
Spigelian belt:a transverse zone of 6 cm located above the interspinal plane.
Semi circular line: also known as arcuate line or line of Douglas, marks the caudal end of the posterior lamina of the aponeurotic rectus sheath. This line is found in the infraumbilical area and represent the anatomical transition, inferior to which, all the aponeurotic layers of the abdominal muscles, except the transversalis fascia, pass simultaneously anterior to the rectus abdominis muscle. At the caudal side of the semicircular line, the posterior side of the rectus abdominis muscle is covered only by the transversalis fascia and the peritoneum.
Rectus sheath: fibrous compartment that contains both the rectus abdominis muscles and the pyramidalis muscle that extends from the inferior costal margin and the costal cartilages of fifth to ninth ribs to the pubic crest. The fascial coverings of the external oblique, internal oblique, and transversus abdominis muscles comprise the rectus sheath [3].
Hesselbach’s triangle: limited by the inferior epigastric vessels, the rectus abdominis muscle and the inguinal ligament.
Epidemiology
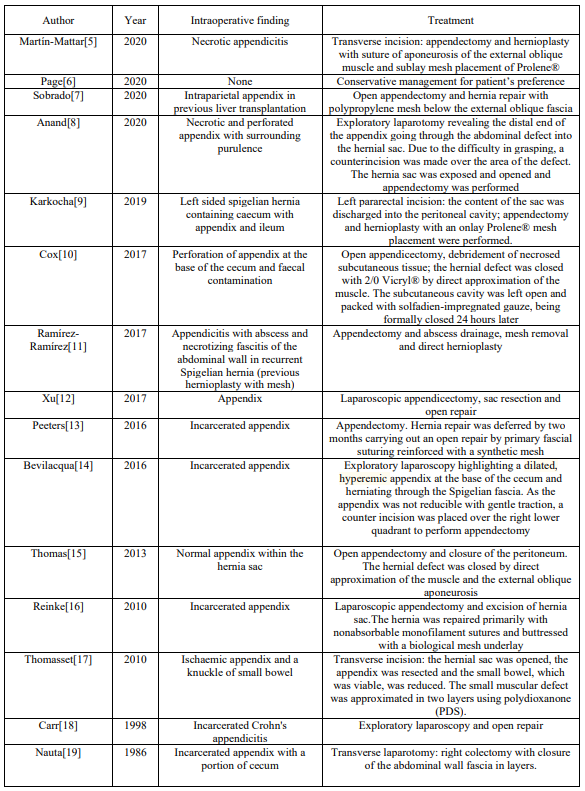
SH is rare and account for only 0.1%-2% of occurrence. However the risk of incarceration and strangulation is high due to the small size of the fascial defect [1, 4]. The hernia sac consists of extraperitoneal fat and peritoneum. Occasionally, the extraperitoneal fat is preceded by remnant bands from the transversalis fascia. Usually, SH contains small bowel or omentum. However, multiple intra-abdominal organs have been reported to have been found in the SH as large bowel, stomach, gallbladder, Meckel diverticulum, ovary, testis, leiomyoma of the uterus, and even bladder [1]. The involvement of appendix has also been described in various case reports [5-19] (table 1).
75 year old man, BMI 24.9 kg/m2
Comorbidity: diabetes mellitus, benign prostatic hyperplasia
Previous surgery: open right inguinal herna repair, open repair of strangulated left side SH with the hernia sac containing sigmoid loop with infarcted appendices epiploicae, subsequently laparoscopic left side SH repair with intraperitoneal mesh placement (IPOM) for recurrence
The patient presented to general surgery facility complaining right abdominal pain and discomfort. Physical examination demonstrated mild tenderness and a bulging of the right side. Abdominal ultrasound revealed an incarcerated SH containing vermiform appendix. Abdominal CT scan confirmed the ultrasound diagnosis and ruled out other abdominal disease.
Surgical technique
The patients underwent laparoscopy with placement of three trocars (a 5 mm sovraumbilical trocar for the telescope, a 10 mm trocar in left flank for the introduction of the stapler and the mesh, and a 5 mm trocar in ipogastrium) avoiding the area of the previous repair of the left SH. The hernia defect containing the incarcerated appendix was visualized. After being reduced into the abdominal cavity, the appendix appeared congested and covered by the thickened hernial sac but there were no sign of ischaemia and purulent peritonitis. Appendectomy and resection of the sac were then performed and the defect was addressed clearing off the peritoneum and the preperitoneal adipous tissue up to 5-6 cm from the edges. The defect was measured by the introduction of a sterile ruler (the size of the defect was less than 2 cm). No closure of the defect was carried out. An expanded polytetrafluoroethylene mesh (Gore® Dualmesh®, W.L. Gore & Assoc., Flagstaff, AZ, USA) was shaped of adequate size in order to obtain an overlap of about 5 cm per side and introduced into the abdominal cavity. The pneumoperitoneum was reduced to 8-9 mmHg and the fixation of the mesh was obtained using laparoscopic tackers and cyanoacrylat glue. A careful inspection of the deep ring and the identification of the angle of doom and the triangle of pain was done before fixation of the tacks to avoid injury to the testicular vessels, duct deferens, inferior epigastric vessels, iliac vessels, (the structures of the inverted Y) and the lateral cutaneous nerve of the thigh, the femoral branch of the genitofemoral nerve and the femoral nerve (crossing the triangle of pain). The cyanoacrylat glue was used to fix the part of the mesh closest to the internal inguinal ring. No intraoperative or postoperative complications occurred and the discharge was on day 2. Pathological examination revealed a chronic appendicitis.
1) SHs often have a narrow fascial defect and may be intra-parietal hernias, meaning that the hernial content may not lie below the subcutaneous fat but penetrate between the muscles of the abdominal wall [20]. Therefore, these hernias may be misdiagnosed at clinical examination and have an increased risk of incarceration and strangulation. Laparoscopic exploration, when feasible, is fundamental to evaluate the inflammation degree and the possibility of carrying out a mini-invasive treatment.
2) SHs may be primitive o secondary to previous trocar insertion [21, 22]. In the present case, four years earlier, the patient had undergone laparoscopic IPOM repair for recurrent left side SH. It is difficult to say if the right side SH was primitive or secondary to previous trocar insertion as the skin scar was barely visible.
3) In emergency setting, the risk of wound infection must be carefully considered before mesh positioning. In this case, we used the IPOM repair with an expanded polytetrafluoroethylene mesh given the absence of any abdominal effusion and phlegmonous appendicitis.
4) The IPOM method is the most popular type of repair among the laparoscopic methods of SH repair, including trans-abdominal preperitoneal mesh (TAPP) and totally extra-peritoneal mesh (TEP) placement. IPOM technique is usually a quick procedure and less demanding. However, tack fixation may result in disastrous drawbacks [23, 24]. In particular, it is necessary to consider the risk of damage of anatomical vascular and nervous structures surrounding the internal inguinal ring given its proximity to the Spigelian belt. Therefore, before positioning of the tacks, a careful inspection of the inguinal region and the identification of the anatomical landmarks, Hasselbach triangle, triangle of pain and triangle of doom, is mandatory. As was shown in a previous report of the Literature, the technique to partially fix the mesh with cyanoacrylat glue was adopted, in order to reduce the number of tacks near the inguinal ring and the epigastric vessels [25].
5) The approximation of the hernia defect was not carried out for two reason: the small size of the defect and consequently the low risk of post-operative seroma, and to avoid tension and alteration of the muscle-tendon dynamics of the abdominal wall at this level in close proximity to the internal inguinal ring. Furthermore, because of the anatomic nature of SH, the abdominal wall is stable and provides reasonable support after the incorporation of a mesh [26, 27].
6) The presence of vermiform appendix within the hernial sac is peculiar. The presence of vermiform appendix within the inguinal hernia is namend Amyand’s hernia after, in 1735, Amyand described the first case of incarcerated inguinal hernia, containing a perforated appendix, in an 11-year-old boy [28]. Femoral hernia containing the appendix was named De Garengeot hernia after Rene Jacques Croissant De Garengeot first described in 1731 a case of femoral hernia, containing a non-inflamed appendix [29]. Although rare entity, a classification of Amiand’s hernia have been described in order to improve management [30]. This last point of discussion is precisely aimed at underlining the importance of giving a name to the SH containing appendix. The search for scientific literature on the subject would become rapid and immediate allowing to obtain all the necessary information on the optimal management of this uncommon pathology.
This pathological condition could be indicated with the acronym VAISAD (vermiform appendix in Spigelian aponevrosis defect).
The table 2 presents a classification proposal on the basis of the severity of inflammation of the vermiform appendix incarcerated in the SH and on its reducibility into the abdominal cavity by laparoscopic traction.
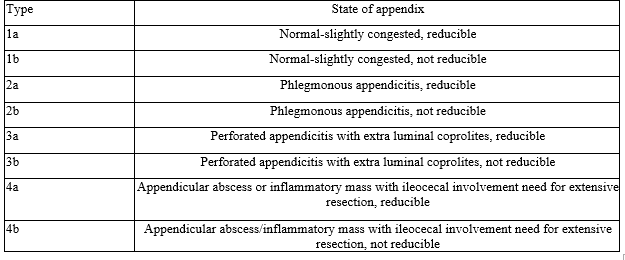
The type a is amenable of mini-invasive treatment if feasible, while the type b requires open treatment or conversion to laparotomy. Mesh repair is safe only in type 1 (in absence of contamination). In the setting of contamination a tailored approach is indicated balancing the risks and benefits of the use and the type of the mesh.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
