
Review Article | DOI: https://doi.org/10.31579/2641-0419/020
1* Department of Cardiology, Military Hospital “Dr. Carlos Arvelo” Caracas, Venezuela.
*Corresponding Author: Tania T. Muñoz H, Department of Cardiology, Military Hospital “Dr. Carlos Arvelo” Caracas, Venezuela.
Citation: Tania T. Muñoz H. (2019) Vasoreactivity Test to evaluate the Pulmonary Vascular Resistance and Mean Pulmonary Arterial Pressure by Doppler Echocardiography. J.ClinicalCardiologyandCardiovascularInterventions, 2(3); Doi.Org:10.31579/2641-0419/020
Copyright: © 2019 Tania T. Muñoz H. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 October 2019 | Accepted: 04 November 2019 | Published: 11 November 2019
Keywords: vasoreactivity test; pulmonary vascular resistance; pulmonary arterial pressure; doppler echocardiography
The pulmonary vascular reactivity test (PVRT) is essential to define patients with pulmonary hypertension(PH) responders to calcium antagonist treatment, this is possible evaluating the changes registered in the 3 hemodynamic variables: pulmonary vascular resistance (PVR), mean pulmonary arterial pressure(MPAP) and cardiac output(CO).Cardiac catheterization is unquestionably the gold standard for performing the test, but its application implies high costs, technical boarding limitations, risks and complications minor to serious inherent to the procedure. On the other hand, Doppler echocardiography is harmless and economical, offering in the last 15 years a considerable advance in techniques and practical methods for estimating these variables, being the most analyzed and documented to date, the PVR.
In this study we will review the different echocardiographic equations proposed by different authors to calculate the PVR and MPAP, in all cases, comparing the results obtained with the measurements made by the right heart catheterization (RHC) .The results obtained in them will be briefly mentioned and will give an important reference to the reader of a study done in our research center, where we grant a new use to the non-invasive measurement of MPAP applied in the PVRT.
| ABBREVI A T I ONS | ||
| and ACRONYMS | ||
| PVRT = pulmonary vascular reactivity test | ||
| PH = pulmonary hypertension | ||
| PVR = pulmonary vascular resistance | ||
| MPAP = mean pulmonary arterial | ||
| presssure | ||
| CO = cardiac output | ||
| RHC : right heart catheterization | ||
| TR= tricuspid regurgitantion | ||
| TRV=peak tricuspid regurgitant velocity | ||
| TVIRVOT = right ventricular outflow tract | ||
| time-velocity integral | ||
| ∆PR = transvalvular pressure gradient of | ||
| pulmonary regurgitation | ||
| tSm = systolic velocity of tricuspid | ||
| annulus | ||
| ∆CAP= capillary arterial pressure | ||
| gradient | ||
| PAT= pulmonary acceleration time | ||
| PPE= pre-ejection period | ||
| TT= total ystolic time | ||
| ∆PRi²=gradient derived of initial peak | ||
| velocity of pulmonary regurgitation | ||
| ∆PmRT= mean pressure gradient of | ||
| tircuspid regurgitantion | ||
| RAP= right atrial pressure | ||
| PCP= pulmonary capillary pressure | ||
| PAH= Pulmonary arterial hypertension | ||
| HR= heart rate | ||
| SPAP=systolic pulmonary artery pressure | ||
| RVSP= Right ventricular systolic pressure | ||
| WU= Wood Units | ||
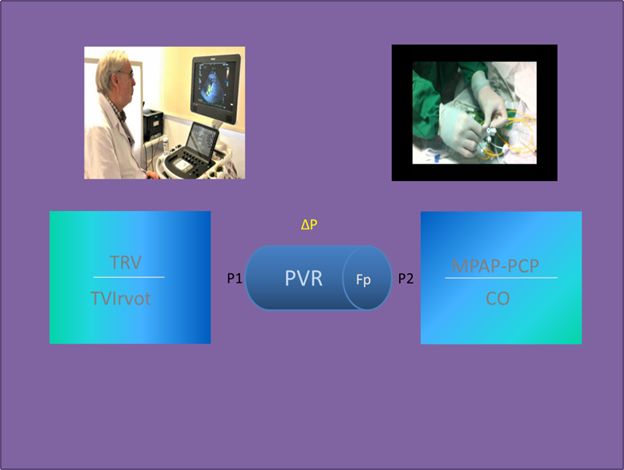
Several echocardiographic methods have been proposed to allow the calculation of the PVR, some incorporate the ratio of peak tricuspid regurgitant velocity (TRV) / right ventricular outflow tract time-velocity integral (TVIRVOT) [1-4](figure 1); other authors used different approaches and / or variables, such as the transvalvular pressure gradient of pulmonary regurgitation(∆PR),[5] systolic velocity of tricuspid annulus (tSm),[6] capillary arterial pressure gradient (∆CAP), [7] the E / E´septal ratio [8] and the ratio (pre-ejection period(PPE)/ pulmonary acceleration time (PAT)) / total systolic time (TT).[9]
MeanPulmonary arterial pressure (MPAP),is an indispensable hemodynamic variable for the diagnosis, classification and prognosis of Pulmonary Hypertension (PH). Its quantification is performed invasively and non-invasively by Doppler echocardiography. Masuyama [10] proposed its measurement by the transvalvular diastolic pulmonary gradient derived from the initial maximum velocity of pulmonary regurgitation (ΔPRi2) corresponding closely to the invasive measurement. Kitabatake et al[11], suggested estimating MPAP through the calculation of PAT, complemented with the study of pulmonary flow morphology. Chemla et al[12], proposed a method derived from the maximum velocity of TR and quantification of SPAP with the modified Bernoulli equation obtaining values close to those obtained invasively. Another equation derived from TR, is based on the estimation of the mean pressure gradient (∆PmTR) and the RAP, enunciated by Aduen et al. [13]
Until now, none of these equations has been recommended by the American and European Cardiology Society guidelines on diagnosis and treatment of Pulmonary Hypertension (PH), [14] leaving its measurement reliably reserved for RHC [14-16]. The same happens to the pulmonary vascular reactivity test where the measurements of these variables are essential to evaluate the diagnostic and therapeutic goal [17-20]. In this work we will review studies that propose echocardiographic measurements of the hemodynamic variables PVR and MPAP involved in the test.
PVR is an essential hemodynamic variable for the management of patients with cardiovascular and pulmonary pathologies. Its measurement can be performed invasively with the Swan Ganz catheter or Judkins catheter from the ratio of the pressure gradient and the transpulmonary flow (MPAP-

PCP/CO). [21-23] This variable is essential to assess the afterload imposed on the right ventricle, especially in patients affected by PH. Figure 2
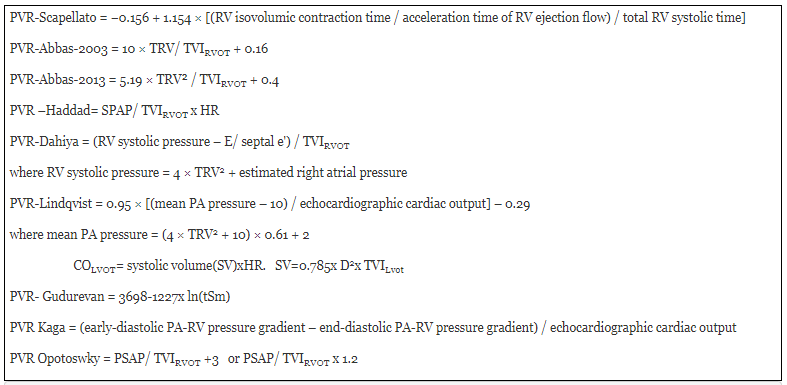
summarizes the different uses and applications of the PVR. Abbas et al [2], of the Department of Cardiology of the Mayo Clinic; Scottsdale, Arizona, California; in 2003, they proposed a simple Doppler echocardiographic equation PVR = TRV / TVIRVOT 10 + 0.16. According to this author, the TRV could correspond to the measurement of the pressure gradient and TVIRVOT with the cardiac flow, both obtained invasively. He reported in his study a high correlation when comparing both methods (R2 = 0.92). However, this work presented a great limitation by excluding patients with moderate and severe tricuspid regurgitation, representing the sector most in need and probably most benefited with this measurement. Subsequently, publications aimed at validating this work [24-29] discussing its content [4,5,8] or establish different approaches and hemodynamic variables. [6,9]
Prior to this publication, Scapellato et al [9] ,of the Rehabilitation Medical Center, Division of Cardiology, Veruno, Italy (2001); determined an index for the calculation of the PVR =PPE / PAT / TT; demonstrating that a value> 2.6 predicts an pulmonary vascular resistance obtained by catheterization (PVRcath> 2.5 Wood units (WU). Years later, this equation was questioned by Haddad et al [3], since it was not applicable in their work due to low correlation (R2 = 0.30).
Gudurevan et al, [6] of the Division of Cardiology at the University of California, in 2007, stated an inverse relationship between the estimation of systolic velocity of tricuspid annulus (tSm) by tissue doppler and the PVR; determining that a velocity <10> 12.5 WU. They obtained a high correlation with cardiac catheterization (R2 = 0.71). The proposed equation was: PVR = 3698-1227 x ln(tSm).
Vlahos et al [24] (2008), Stanford University and California; Loannina University, Greece; conducted a prospective study in 12 liver transplant candidates and obtained PVRcath. They analyzed the TRV / TVIRVOT and TVR / TVIRVOT index, corrected for the diameter of the RVOT, finding that both correlated well with PVRcath R2 = 0.711 and R2 = 0.731, respectively.
Haddad et al [3] of Stanford University, Division of Cardiovascular Medicine (2009), proposed the index to obtain PVR = systolic pulmonary artery pressure (SPAP) / heart rate (HR) x TVIRVOT in a group of patients with Pulmonary arterial hypertension (PAH). They concluded that a cut-off value of 0.076 provides 86% sensitivity and 82% specificity to determine a pulmonary vascular resistance index (PVRI)cath greater than 15 WU / m2.
Dahiya et al [8] of the School of Medicine, of the University of Queensland, Australia in 2010; They proposed the following echocardiographic equation: PVR = [Right ventricular systolic pressure (RVSP) - E / E' septal] / TVIRVOT reporting high correlation with the invasive method (R2 = 0.77). In this work, the authors found that when comparing the PVR measurements obtained by the Abbas method with the RHC these were underestimated, recommending their method by not presenting this limitation.
Lindqvist et al [7] of the Department of Cardiology of the University of Umea, Sweden (2011); described a more arithmetic calculation from the PVR = 0.95 × [(MPAP - 10) / cardiac output (CO)] - 0.29; the correlation reported with RHC was R2 = 0.87.
Opotoswky and at [4] of the Children's Hospital of the Department of Cardiology, Boston (2013), published a paper (217 patients) where they validated and then compared 2 equations with the one stated by Abbas et al (2003) (model 1). The derived models were: RVP = 1.2 × SPAP / TVIRVOT (model 2) and PVR = (SPAP / TVIRVOT) +3; if the systolic notch is present (model 3). They found that model 1 systematically underestimated the mesurement PVR by catheterization. Model 3 was better correlated with PVRcath(R2 = 0.80 vs; R2 = 0.73 and R2 = 0.77 for models 1 and 2, respectively). This approach generated discomfort in Abbas et al (Department of Cardiology of the System of Health Beaumont, Royal Oak, Michigan), because precisely in 2013, they published an article that seemed to solve the representative exclusion of patients with high PVR in their first job. To this end, they postulated a new equation: PVR = TRV² / TVIRVOT x 5–0.4, for patients with high PVR values, finding that a TRV / TVIRVOT index ≥ 0.275 defined the cut-off point for PVRcath> 6 UW. Currently his two works have wide recognition and acceptance in the medical community.
Yan et al [29], of the Department of Radiology, Nuclear Medicine and Echocardiography of the National Center for Cardiovascular Diseases, Cardiovascular Institute and Hospital of Fuwai Beijing, China (2015), estimated the PVR = MPAP-PCP / CO. They combined the Doppler echocardiogram to obtain MPAP and pulmonary capillary pressure (PCP) with cardiac magnetic resonance imaging (CMR) to quantify the CO.
Kaga et al [5] in the year 2017 of the Faculty of Medical Sciences of the University of Kita, Sapporo, Japan; They stated an equation based on the difference in the initial diastolic and final diastolic pressure gradient obtained through pulmonary regurgitation (PR) and cardiac output of the left ventricular outflow tract (COLVOT), . They analyzed the linear correlation between the Abbas equations (2003 and 2013) and the Scapellato equation with catheterization, obtaining correlation coefficients of 0.54. 0.66 and 0.54 respectively. They reported that the best correlation with catheterization was obtained by their equation (R2= 0.81).
II) Mean pulmonary arterial pressure: Mean Pulmonary artery pressure (MPAP) is an indispensable hemodynamic variable for the diagnosis, classification and prognosis of Pulmonary Hypertension (PH). Its quantification is performed invasively by right heart cathererization (RHC) and non-invasively by Doppler echocardiography thanks to different authors have channeled efforts to offer different equations. Kitabatake et al [11] of the First Department of Internal Medicine, Osaka University Medical School, Osaka, Japan in 1983, demonstrated possible its estimation starting of the PAT obtained with pulsed Doppler in the RVOT, with the relationship PAT/ right ventricular ejection time (RVET) and they described different patrons of flow with the midsystolic notching, in cases severs of PH. Dabestani et al [30], from the Division of Cardiology, Department of Medicine, University of California, Irvine Medical Center, Orange, California, USA in 1987, validated the flow velocity patterns and found that in patients with an acceleration time of 120 ms or less, there was a negative linear correlation with MPAP, expressed by the equation: MPAP = 90 - (0.62 X PAT) and a PAT≤100 ms corresponded to high pulmonary arterial pressure(sensitivity 78%, specificity 100%). Chemla et al [12], proposed a method derived from the maximum velocity of tricuspid regurgitation (TR) and quantification of systolic pulmonary artery pressure (PSAP) with the modified Bernoulli: PMAP= 0.61xPSAP+1.95 Another equation derived from TR is based on the estimation of the mean pressure gradient (∆PmTR) and the right atrial pressure(RAP), stated by Aduen et al. [13] from Division of Pulmonary Medicine, Mayo Clinic, Jacksonville, Florida, USA in 2009;. reporter in theirs work superiority in theirs method by finding an average difference of MPAP values with respect to the RHC of -1.6, less than the SPAP traditionally obtained with TR (-3.6) and comparing it with the PR method (-13.9) In a recent retrospective work [31] where they compared the 3 methods analyzed in this study, among others, with invasively obtained measurements, they found superiority with the Aduen equation. Also when this author compared his method, the Chemla equation and the Syyed equation with the measurements obtained invasively, he found a discrete superiority in his method [32]. Table 2 summarizes the echocardiographic equations to calculate the MPAP.

Right catheterization and PVRT:
At present, right catheterization is still considered as the gold standard for the definitive diagnosis of pulmonary arterial hypertension (PAH) and the method of choice to perform PVRT. [14] According to the guidelines of the European Society of Cardiology, this study is indicated for the diagnosis and treatment of patients with group 1: idiopathic PAH, hereditary PAH and associated with drug use [14] Through this procedure it is possible to evaluate the behavior of pulmonary vascular circulation before the stimulation of drugs that they produce acute dilation, making possible the diagnosis of patients who will respond to calcium antagonist treatment [14]. Until some time ago, there were multiple definitions of positivity in the vascular reactivity test which included a decrease of more than 20% of the PVR, without changes in cardiac output or a decrease in both MPAP and PVR greater than 20%. [17-19] An acute positive response defined as a reduction in MPAP> 10 mm Hg was then standardized, reaching an absolute value of MPAP <40>
At the last PH World Symposium held in December 2018, [15] it was agreed to incorporate within the new clinical classification of PH into group 1 of PAH: 1.5 Prolonged response to calcium channel blockers. Backed by the argument that although remodeling of small pulmonary arteries is the main pathological finding in PAH, vasoconstriction also plays an important role in the pathophysiology of PAH, particularly in vasoreactive patients. In a series of 64 patients published in 1992, RICH et al. [33] reported that patients with an acute vasodilator response to calcium channel blockers (CCB) had dramatically improved survival when treated with long-term beta blockers.
The long-term response to CCB was defined by clinical improvement (functional class I or II of the New York Heart Association) and sustained hemodynamics improvement after at least 1 year only in CCB (equal to or better than that obtained in the test Acute and generally to obtain MPAP <30>
The pathophysiology of PAH with vasoreactivity is largely unknown. Recently, Hemnes et al, have shown that PAH with vasoreactivity, was characterized by a specific blood form (lymphocyte microarray) and different genetic variants (complete exome sequencing) compared to PAHI. [35,36]These results suggest a specific entity with a different clinical course, characterized by a significant improvement in prognosis, unique management and different pathophysiology.
Classically, the drugs chosen to evaluate lung reactivity have a relatively selective effect on the pulmonary vasculature, such as inhaled nitric oxide, epoprostenol and adenosine infusion [17,37] although in another context, such as in patients with heart failure, they have been used vasodilators nitroprusside and nitroglycerin type,m [38,39] and even inodilators. [40] These drugs have a systemic effect and therefore greater adverse events, which poses difficulties in carrying out the test; In addition, they should be used in continuous infusion with dose titration, which prolongs the procedure and some of them are expensive. More recently, other options have been evaluated: iloprost, a prostaglandin analogue with a short half-life (20-30 minutes) that is recommended for intravenous or inhaled use. The inhaled route allows its effect to be selective pulmonary, specifically on the adventitial side of the pulmonary arterial wall, and in theory with fewer side effects. [41] It produces a decrease in PVR, MPAP, CO and saturation of mixed arterial and venous oxygen. [42] Studies have been conducted evaluating its usefulness in the PVRT with encouraging results, [43-48] so It has been suggested as an option in some PAH consensuses. [48] When the inhalation route is chosen, iloprost is used in ampoules of 1 ml of aqueous solution with 10 mcg for complete administration over a period of 30 minutes of fogging. Until de present, there are no reports of studies comparing simultaneous measurements of PVR and MPAP with the invasive method and echocardiographic doppler in PVRT. [49]
.We conducted in our University Military Hospital in Caracas Venezuela in 2019,[50] a research work where invasive and non-invasive measurements of MPAP were compared during the vasoreactivity test in all its stages; finding very high correlation in all, shown in the study the times t0, t30 and tR; (R2 = 0.87,0.99 and 0.98, respectively).Based on the encouraging results of this work, we recommend developing studies with a larger population of patients who estimate MPAP and other variables involved through echocardiography and RHC.
Discussion: MPAP and PVR are hemodynamic variables that have common applications, the most relevant are: distinguish the hemodynamic class of PH[15], quantify arterial elastance (Ea) from Ventricle Arterial Coupling[51] and define the response acute vasodilation in the PVRT[14,17]. Both variables, have been analyzed echocardiographically by different authors from different locations in the world, in a variety of patients with different clinical conditions and degrees of severity of PH, always comparing the measurements with those obtained by RHC to be able to validate their methods. In the case of the PVR, some of the studies analyzed in this review included an interesting comparison of their equations with those of other authors, showing in all cases, the superiority of the method of each research group, given by the highest correlation with the RHC[3-5] (see figure 3).This was also the goal established among the echocardiographic methods to obtain the MPAP through TR, representing the most recent proposals and shown as the most effective. [13, 31, 32] (Figure 4). However, despite all this extensive work carried out over three long decades, these echocardiographic assessments remain lagging behind and forgotten like a “Cinderella”. It isn’t the object of this review to question the use of RHC as the gold standard to perform these measurements, if instead, try to open a humble door to consider echocardiography as an excellent evaluation alternative in those patients who cannot perform the RHC due to high costs, the complications inherent in the procedure or the refusal of the patient or his relatives to perform it. It´s also important to keep echocardiography in mind as a valuable follow-up resource for patients who deserve repeated assessments of PVR and MPAP.
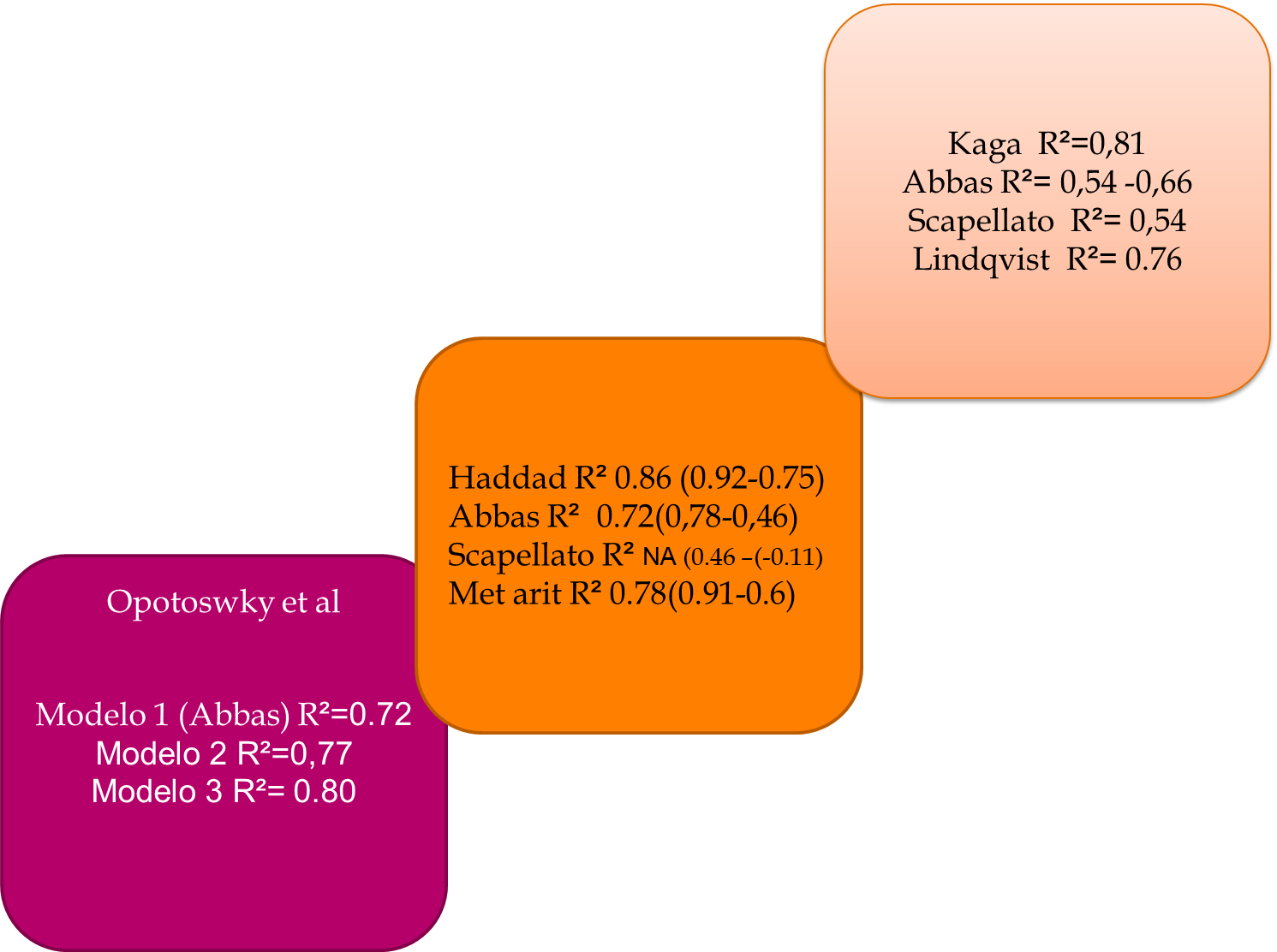
Figure legend 3:
Opotoswky et al reported the best correlation with PVRcath when applying model 3 corresponding to the presence of mesosistolic notch in the pulmonary flow. Haddad et al: For all methods, the highest correlation was observed for the lowest RVP values (values in brackets); the highest correlation with RHC was with his method and reported that the Scapellato method didn´t apply for study. Kaga et al compared their method with the two Abbas equations that make up their algorithm. They found a better correlation with the enunciated in 2013. The highest correlation reported was obtained with their method followed by the PVR Lindqvist.
In the case of PVRT, an excellent opportunity was found to analyze the applicability of Doppler echocardiography by measuring these two hemodynamic variables by simply recording the TRV and the TVIRVOT. In this sense, a research work was carried out in our center comparing the invasive and non-invasive measurements of the MPAP finding very high correlation between the methods. In the case of the PVR estimates, high correlation was also obtained by applying the Abbas algorithm in the 6 stages of the test.
It’s necessary to point out that the invasive and non-invasive methods are dependent operators, in both cases the observer must carefully analyze the set of data obtained for each patient, integrate them as a hemodynamic whole and never automatically take it as a single isolated value. This will allow us in all cases to narrow the margin of errors and possibly facilitate opening a window for the era of non-invasive measurements.

Figure legend 4:
Aduen et al 2009, reported in their work superiority to find an average difference of MPAP values with respect to the RHC of -1.6, less than the SPAP traditionally obtained with RT (-3.6) and comparing it with the PR method. Aduen et al 2011: The mean ± SD of the differences between invasive MPAP and the three echocardiographic methods were −1.6 ± 7.7 mm Hg for the mean gradient method, −3.7 ± 7.4 mm Hg for the Chemla formula, and −3.2 ± 7.6 mm Hg for the Syyed formula. Median absolute differences were 5.5 mm Hg (mean gradient), 5.7 mm Hg (Chemla; P = .45 vs mean gradient), and 6.0 mm Hg (Syyed; P = .23 vs mean gradient). Accuracy (calculated MPAP within 10 mm Hg of RHC-measured MPAP) was 81% (mean gradient), 77% (Chemla), and 76% (Syyed).* In a work published recently in 2017 (Hellenkamp K et al [36]), the authors recorded the highest correlation with the Aduen equation and the lowest with the Dabestani equation (PAT), when compared with PVRcath.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
