
Case Report | DOI: https://doi.org/10.31579/2690-4861/776
Gynecologic Oncology, Kaiser Permanente Cancer Center at LAMC, 4950 Sunset Boulevard, Suite 582, Los Angeles, CA 90027.
*Corresponding Author: Scott E Lentz, Gynecologic Oncology, Kaiser Permanente Cancer Center at LAMC, 4950 Sunset Boulevard, Suite 582, Los Angeles, CA 90027.
Citation: Hillary Kroll, Yingao Zhang, Scott E. Lentz, (2025), Vascular Injury During Gynecologic Surgery as a Result of Self-Retaining Retractor in a Low-Resource Setting, International Journal of Clinical Case Reports and Reviews, 27(1); DOI:10.31579/2690-4861/776
Copyright: © 2025, Scott E Lentz. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 May 2025 | Accepted: 09 June 2025 | Published: 23 June 2025
Keywords: textiloma; gossypiboma; foreign body; surgical procedure
Background: Self-retaining retractors are surgical tools to facilitate hands-free visualization and exposure while operating. The most common complication of self-retaining retractor use in gynecological surgery is nerve injury. This case presents a rare incidence of vascular injury as a result of the use of a self-retaining retractor in abdominal hysterectomy.
Case: A patient underwent abdominal hysterectomy for abnormal bleeding and dysmenorrhea in which a Balfour self-retaining retractor was used. The patient subsequently decompensated and required emergent laparotomy secondary to repair a laceration of the deep circumflex iliac artery.
Conclusion: The self-retaining retractor used in this low-resource setting was suboptimal, requiring frequent replacement throughout the case, leading to a previously unreported complication of vascular injury.
Self-retaining retractors are helpful surgical tools that facilitate hands-free visualization and exposure while operating. [1–3] While overall safe, when used in abdominal surgery, self-retaining retractors have been implicated in complications such as nerve injury and bowel injury. [1,4–6] This case presents a rare incidence of vascular injury as a result of the use of a self-retaining retractor in abdominal hysterectomy in a low-resource setting.
A 40-year-old nulliparous patient with history of dysmenorrhea and abnormal uterine bleeding requiring multiple transfusions presented for evaluation with our surgical mission team at a municipal hospital in the Philippines. An abdominal ultrasound demonstrated uterine fibroids as well as radiographic evidence suggestive of deep infiltrating endometriosis. She was counseled on the risks and benefits of definitive surgery, and agreed to total abdominal hysterectomy and bilateral salpingo-oophorectomy.
The patient underwent an uncomplicated total abdominal hysterectomy with bilateral salpingo-oophorectomy via a Pfannenstiel incision. A Balfour retractor was used, but required multiple repeated re-adjustments during the operation because it would not remain in position during surgery. Surgical findings were significant for a 6cm x 4cm uterine myoma and dense adhesions between the posterior uterus and sigmoid colon. Bilateral adnexa were normal appearing. Lysis of adhesions did not require retroperitoneal exploration. All surgical pedicles were examined prior to closure and found to be hemostatic, and estimated blood loss was 100ml. The patient was awakened from anesthesia without issue and moved to the recovery room.
In the recovery area, the patient developed severe hypotension within 30 minutes of transfer. Intubation was performed and aggressive fluid resuscitation was administered. The patient continued to decompensate, showing abdominal distension. The endotracheal tube was repositioned to exclude improper intubation as a cause for distension. Ultrasound was not available to assess the abdomen and the incision was opened at the bedside confirming hemoperitoneum. Cardiac arrest occurred during resuscitation efforts and CPR helped restore sufficient circulatory response to allow for emergent exploratory laparotomy.
Upon re-entry into the abdomen, there was approximately 3L of hemoperitoneum. Active arterial bleeding was noted from a laceration in the deep pelvis on the right side. This vessel was quickly clamped and suture ligated with good hemostatic control. There was no other source of active bleeding on a comprehensive abdominopelvic survey. The ligated vessel was then identified as the right deep circumflex iliac artery, immediately cephalad to its origin from the right external iliac artery. The right retroperitoneum was noted to be opened, near where the right blade of the Balfour retractor was previously placed, suggesting an iatrogenic vascular injury due to the frequent manipulations of the retractor. Her vital signs improved with continued vasopressor support and a total of four units of packed red blood cells. She was able to be extubated following the second procedure and had an uneventful postoperative recovery until hospital discharge on post-op day [5].
Self-retaining abdominal retractors are commonly utilized in open abdominal surgery around the world, and come in fixed (Balfour, Bookwalter, Kirschner, or Holzbach) or flexible (AlexisTM, MobiusTM) systems. [2,7] This case illustrates a rare vascular injury from a self-retaining retractor during abdominal surgery, something which has not been described previously. Developed in 1912, the Balfour retractor is a commonly used three-bladed instrument that allows for retraction and spreading at the incision site (Figure 1). [3,8] Nerve injury is the most common complication associated with self-retaining retractors, with reported rates ranging from 8 to 11% in open gynecologic surgeries. [1,6] Nerve injury is thought to result from excessive compression against the pelvic sidewall, particularly when the retractor blades are improperly placed or are used for prolonged periods of time. [5,6]
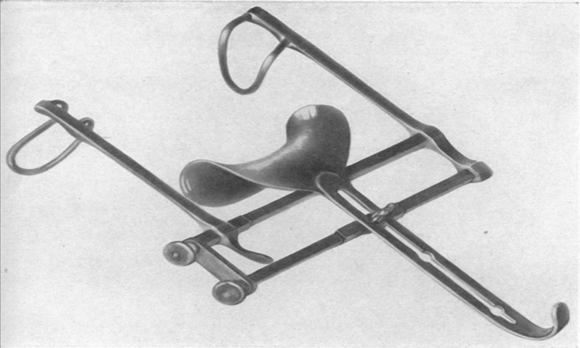
Figure 1: Balfour Retractor
In this case, the Balfour retractor was used as it was the only available instrument in the provincial hospital during the surgical mission. However, during the case, numerous re-adjustments of the Balfour had to be performed to maintain a static position, requiring frequent replacement of the retractor blades and repeated opening of the retractor throughout
the case. While it is unclear exactly how the retractor contributed to the vascular injury, we postulate that frequent opening of the Balfour retractor resulted in a retroperitoneal laceration causing deep circumflex iliac artery injury due to vascular shearing. A diagram of the anatomy of the area is shown in Figure 2.
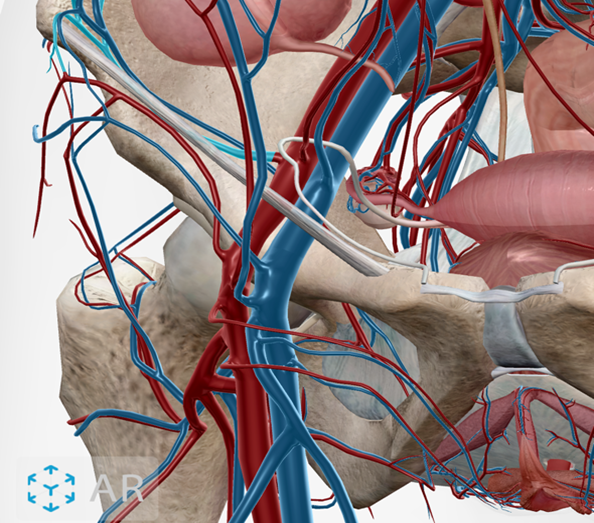
Source: Visible Body Suite, Human Anatomy Atlas (Version 2025.00.012) [mobile device software]. (2023).
Figure 2: Deep Circumflex Iliac Artery
Lateral to the external iliac artery as it exits the pelvis beneath the inguinal ligament, the deep circumflex iliac artery passes laterally and cephalad to supply the external oblique musculature. The artery is highlighted in light blue in the image above.
As we acknowledge that the standard instrument available in this low-resource setting contributed to further surgical complication, our team considered other possible retraction options to improve our care. Flexible retractors such as the Alexis O-Ring retractor or the Mobius Elastic retractor are self-retaining retractors composed of two plastic rings joined together by a plastic sheath (Figure 3). [9,10] They are commonly used in obstetric, gastrointestinal, urological and hepatobiliary surgery. [9] Studies have shown that these retractors can decrease risk of surgical site infections and have been shown to cause less trauma to surrounding tissues. [9,11] During our literature search, we did not find any data on the association of these flexible self-retaining retractors and nerve or vascular injury. However, one study did find a decreased need for opiate pain medication after abdominal surgery with an Alexis retractor as compared to a Balfour retractor, leading us to conclude there was less tissue injury.[7] In addition to these noted benefits, flexible self-retaining retractors are disposable and therefore do not require maintenance. [10,12] Although a desirable option, the current cost of flexible retractor systems is prohibitive to their routine use in low-resource settings. [10,13]

Figure 3: Alexis O-Ring Retractor
Alexis® O™ C-Section Retractor (Applied Medical Resources Corporation, Rancho Santa Margarita, CA). Photo courtesy of Applied Medical Resources Corporation.
This case demonstrates a rare complication of vascular injury secondary to a suboptimal self-retaining retractor. This vascular injury is a previously unreported complication that should now be considered when using metal self-retaining retractors during open abdominal or pelvic surgery. Additionally, this case highlights a unique challenge of operating in a low-resource setting, where upkeep and maintenance of surgical instruments may not be optimal.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
