
Research Article | DOI: https://doi.org/10.31579/2766-2314/053
*Corresponding Author: Azab Elsayed Azab, Department of Physiology, Faculty of Medicine, Sabratha, University, Libya.
Citation: Azab Elsayed Azab, J.M. Jbireal1, S. Alzahani and Rabia A. M. Yahya. (2021) Variation of COVID-19 Specific Immunoglobulin's and Some Inflammatory Factors in COVID-19 Patients in the Sabratha Isolation Center, Western Libya. J, Biotech. and Bioprocessing 2(7); DOI: 10.31579/2766-2314/053
Copyright: © 2021, Azab Elsayed Azab, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 August 2021 | Accepted: 24 August 2021 | Published: 03 September 2021
Keywords: SARS-CoV-2, COVID-19, coronavirus, IgG, IgM, CRP, ferritin, D-dimer, sabratha isolation center, western libya
Background: Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic causing significant mortality and morbidity and implementation of strict isolation measures. Serological testing can diagnose illness by detecting antibodies (IgM and IgG). Testing antibodies against SARS-CoV-2 is rapid and sensitive for the auxiliary diagnosis of COVID-19. The serum levels of CRP, D-dimers, and ferritin, which may be used in risk stratification to predict severe and fatal COVID-19 in hospitalized patients.
Objectives The present study aimed to investigate the variations in COVID-19 Specific Immunoglobulin's and Some Inflammatory factors in COVID-19 Patients in Sabratha isolation center, Western Libya.
Subjects and Methods: Sixty Confirmed COVID-19 patients hospitalized in the Isolation Centre located in Sabratha city, Libya from the 2nd October 2020 to the 2nd June 2021, were enrolled in this prospective study. Covid-19 patients were defined as positive cases after the detection of SARS-CoV-2 RNA in oro-nasopharyngeal swab samples. Data collected included demographic, clinical, and biological factors. Also, 30 healthy individuals without any chronic disease or respiratory symptoms were recruited for the control group. Blood samples were collected by vein puncture 5 ml of venous blood was withdrawn from each participant in the study by using disposable syringes under the aseptic technique; they were then transferred to a sterile tube for estimating biochemical parameters. Biochemical parameters were determined using automated COBAS E411 and INTEGRA 400 machines in the Sabratha Isolation Centre laboratory. The statistical significance of differences between groups was evaluated with the Kruskal-Wallis H test.
Results: The results showed that patients with COVID-19 had a significant (P<0.0001) increase in IgM levels at 0 day, 14 days, and 21 days, respectively compared with the healthy individuals. Also, IgG levels were showed a gradual significantly (P<0.0001) increase during COVID-19 Virus Infection among COVID-19 patients at 0 day, 14 days, and 21 days compared with the controls. In addition, coronavirus infection caused a significant (P<0.0001) increase in D-dimer, CRP, and Ferritin levels compared with the healthy control individuals.
Conclusion: It can be concluded that coronavirus infection caused a significant increase in IgM, IgG, D-dimer, CRP, and Ferritin levels at different periods compared to the controls. Further studies are needed to confirm these results. COVID-19 Specific Immunoglobulin's and Some Inflammatory factors in COVID-19 Patients These changes in IgM, IgG, D-dimer, CRP, and Ferritin levels during COVID-19 Virus Infection among COVID-19 patients may help the clinicians to better understand the COVID-19 and provide more clinical treatment options.
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a worldwide pandemic since it emerged in December 2019 [1]. In only a few months after initial discovery in Wuhan, China, SARS-CoV-2 and the associated coronavirus disease 2019 have become a global pandemic causing significant mortality and morbidity and implementation of strict isolation measures [2]. Adverse outcomes of COVID-19 were associated with comorbidities, including cardiovascular disease, lung disease, and hypertension. These conditions are more prevalent in men and linked to smoking and drinking alcohol [3, 4]. Epidemiological studies showed that elder patients were more susceptible to severe diseases [4, 5], while children tend to have milder symptoms [4, 6, 7].
COVID-19 is from the same group of ribonucleic acid (RNA) viruses that caused severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) [8-11]. Corona viruses are enveloped, non segmented, single stranded, positive-sense RNA viruses named after their corona- or crown like surface projections observed on electron microscopy that correspond to large surface spike proteins. Corona viruses are classified in the Nidovirales order [11-13].
Presently the tested against COVID-19, not exclusively to the analyzed infection however to anticipate the movement towards serious and deadly structures, these indicators will empower hazard delineation, guide interventional studies to target patients at the upgraded hazard of creating extreme sickness and improve the portion of restricted human and specialized assets in the continuous pandemic. Additionally, ID of lab boundaries equipped for segregating among serious and non-extreme cases, or those at high or generally safe of mortality, will consider advanced clinical situational mindfulness [14].
The fast and precise determination of COVID-19 adds to infection and flare-up administration by empowering speedy and exact general wellbeing observation, avoidance and control measures. Real-time reverse transcriptase polymerase chain reaction (RT-PCR) has been the primary means for diagnosing SARS-CoV-2 [15, 16]. However, molecular detection carries the risk of false-negatives because of low viral loads in specimens [16, 17]. Serological testing, another common laboratory diagnostic, can diagnose illness by detecting antibodies [16]. Knowing the pervasiveness of antibodies to the infection in the populace is significant as far as understanding its spread, and carrying out measures to control it. Seroprevalence surveys are necessary to inform and assist global policymakers in planning measures that could alleviate the economic burden of the disease, and prevent the collapse of the healthcare system [18].
Antibodies protect the host by binding to specific antigens (proteins) on the virus to neutralize its fusion and entry into the host cell and facilitate recognition and killing by phagocytic immune cells [2, 19]. In the SARS epidemic, the detection of IgM and IgG allowed for serological diagnosis [20, 21].
Antibodies secure the host by restricting to explicit antigens (proteins) on the infection to kill its combination and section into the host cell and work with acknowledgment and killing by phagocytic invulnerable cells [2, 19]. In the SARS plague, the recognition of IgM and IgG took into consideration serological determination [20, 21].Testing antibodies against SARS-CoV-2 is rapid and sensitive for the auxiliary diagnosis of COVID-19 [21, 22]. In humans, three kinds of antibodies or immunoglobulins have been the objective of COVID-19 serological tests: IgM, IgG, and IgA. Albeit the elements of the insusceptible reaction in COVID-19 are not completely seen, normally IgM antibodies are delivered by having invulnerable cells during the beginning phases of a viral disease. IgG is often the most abundant antibody in the blood and plays a more prominent role in the later stages of infection and in establishing long-term immune memory [2, 23]. While IgM and IgG antibodies have been the main applicants in COVID-19 serological test improvement, ongoing investigations show that IgA, predominately present in the mucosal tissue, may likewise play a critical role in the immune response and disease progression [2, 24]. Seroprevalence of Immunoglobulin Gamma antibodies against severe acute respiratory syndrome coronavirus 2 is important as a tool to estimate the extent of infection in a population [25]. Previous studies showed that the detectable antibodies concentrations persisted for more than two years in Middle East respiratory syndrome and severe acute respiratory syndrome coronavirus ‐infected patients [1, 26, 27].
Inflammatory biomarkers including C‑reactive protein (CRP), and IL-6 are significantly elevated in the early stages of the disease. In this regard, inflammation-associated biomarkers and coagulation test screening, including the assessment of IL-6, C‑reactive protein, and D-dimer [28]. C‑reactive protein is a plasma protein induced by various inflammatory mediators such as IL-6 and produced by the liver [28, 29]. In this process, the increased level of CRP is associated with disease severity [28, 30]. Biomarkers, such as high serum ferritin have also emerged as poor prognostic factors [31]. Recent clinical data have indicated CRP [32, 33] and other factors may be related to the severity of COVID-19 [5, 33]. Tan et al. [34] found that C‑reactive protein is a good accurate diagnostic tool in early predicting severe Coronavirus disease 2019. Overall, literature evidence suggests that in the early stage of COVID-19, CRP levels could reflect disease severity [34].
D-dimer and other Fibrin degradation products (FDPs) are the products of fibrin degradation that appear after blood clot destruction due to fibrinolysis in the blood. Blood d-dimer concentrations can help the diagnosis of thrombosis [28, 35]. There were numerous differences in laboratory findings between patients admitted to the ICU and those not, including, higher levels of D-dimer in ICU patients [36, 37].
Ferritin is an acute phase protein that can be released from damaged hepatocytes [33, 38]. It is known that ferritin levels may increase during inflammatory, infectious and malignant diseases among others [39]. Also, hyperferritinemia has been previously recognized in abnormal liver function conditions or metabolic syndrome [33, 40-42]. The role of ferritin seems to be ignored even though clinical observation has discovered abnormal ferritin levels in severe COVID-19 patients [5, 33]. Ferritin variations were also consistent with CT manifestation, presenting the ability to act as a sensitive and accurate indicator. Then, the diagnostic value of ferritin for the incidence of severe illness was compared to that of age, sex, CRP, and LYM%, which had been recognized as the risk factors of COVID-19 [33, 34, 43, 44].
Clinicians should consider the serum levels of CRP, D-dimers, and ferritin, which may be used in risk stratification to predict severe and fatal COVID-19 in hospitalized patients [45].
The present study aimed to investigate the variations in COVID-19 specific immunoglobulin's and some inflammatory factors in COVID-19 Patients in Sabratha isolation center, Western Libya.
Sixty Confirmed COVID-19 patients hospitalized in the Isolation Centre located in Sabratha city, Libya from the 2nd October 2020 to the 2nd June 2021, were enrolled in this prospective study. Covid-19 patients were defined as positive cases after the detection of SARS-CoV-2 RNA in oro-nasopharyngeal swab samples. This study was approved by the Research and Ethical Committee of the Faculty of Medicine, Sabratha University. Demographic data were extracted from electronic medical records and patient files. Data collected included demographic, clinical, and biological factors, as well as complications at admission and during the hospital stay. Any missing or uncertain data were collected and clarified through direct communication with the relevant health care providers and family members of patients. Also, 30 healthy individuals without any chronic disease or respiratory symptoms were recruited for the control group. Blood samples were collected by vein puncture 5 ml of venous blood was withdrawn from each participant in the study by using disposable syringes under the aseptic technique. Biochemical parameters were determined using automatic immunoassay analyzer- Snibe Maglumi 2000 Plus, COBAS E411, and INTEGRA 400 machines in the Sabratha Isolation Centre laboratory.
Statistical analysis
Continuous variables were presented as medians (interquartile range [IQR]). The data were analyzed using Graph Pad Prism software version 7. The Kolmogorov-Smirnov test was used to assess the normality of the distribution of continuous variables. The statistical significance of differences between groups was evaluated with the Kruskal-Wallis H test. A P-value of <0>was used to establish statistical significance.
The mean age of the patients was 62.7 years (20–90 years); sixty patients, 39 males (39%) and 21 females (35%) were included in the current study (Figure. 1).
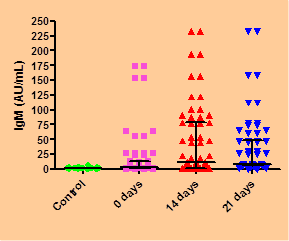
Effect of Coronavirus infection on IgM, and IgG levels in COVID-19 Patients
The results in table.1 and figure. 2 show that patients with COVID-19 had a significant (P<0>) increase in IgM levels [median (IQR), AU/mL], 2.50 (1.23-12.85), 12.10 (1.70-78.30), and 8.30 (5.90-48.00) at 0 day, 14 days, and 21 days, respectively compared with the healthy individuals [1.40 (0.98-2.03)]. Also, IgG levels [median (IQR), AU/mL], were showed a gradual significantly (P<0>) increase in during COVID-19 Virus Infection among COVID-19 patients at 0 day, 14 days, and 21 days [8.80 (1.700-121.3), 154.0 (75.30-416.3), and 291.8 (243-510) compared with the controls 1.50 (1.00-2.40) (Table. 1& Figure. 3).


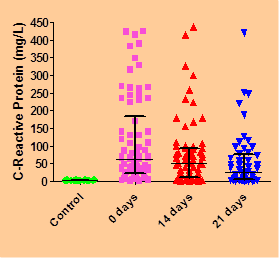
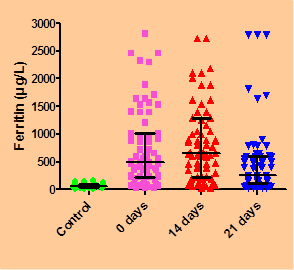
Effect of Coronavirus infection on serum D-dimer, CRP, and Ferritin levels in COVID-19 Patients
Coronavirus infection caused a significant (P<0>) increase in D-dimer levels (µg/ml) [median (IQR)], 0.61 (0.40-1.40), 0.65 (0.37-2.28), and 0.67 (0.42-3.12), in CRP levels (mg/L) 495.4 (228-1010), 664 (232.5-1285), and 261 (119.2-605.0), and in Ferritin levels (µg/L) 62.75 (23.08-183.7), 51 (9.7-93), and 26.55 (4.73-67.25) compared with the healthy control individuals 0.28 (0.20-0.32), 68.15 (45.10-99.28), and 2.35 (1.38-3.18), respectively (Table. 2& Figures. 4-6).


Serum immunoglobulin's against severe acute respiratory syndrome coronavirus‐2 were detectable within the first weeks after the onset of symptoms [1, 46-49]. They were detectable as early as 4 days and reached a peak in the second week after onset [1, 5, 46-48, 50]. Almost all the infected cases had seropositive antibodies in the first 3 weeks post‐illness onset [1, 46]. So, positive detection of IgM and IgG antibodies specific to SARS-CoV-2 has also been recognized as deterministic evidence for confirmed SARS-CoV-2 infection [51-53]. Serological tests may be important tool to estimate the prevalence of virus infection, virus lethality, and provide information about risk factors and immunity such as the patient’s location, and age [18, 54]. Previous studies have suggested that the upsurge of IgG antibody to SARSCoV correlates with the clinical worsening of pneumonia [55-58]. Studies on severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS) showed that virus-specific antibodies were detectable in 80–100% of patients at 2 weeks after symptom onset [46, 57, 60-63].
The current study showed that corona virus infection caused a significant (P<0>) increase in serum IgM and IgG levels at 0 day, 14 days, and 21 days, compared with the healthy individuals. Similar results were recorded by previous studies [1, 16, 21, 46, 58, 64]. During viral infection with SARS-CoV-2, the production of specific antibodies against the virus is consistent in most patients, except for immunodeficient patients. IgM can be detected as early as 3 days after infection and provides the first line of humoural immunity defense, after which high-affinity IgG responses are initiated and play a key role in long-term immune memory [21, 64]. It seems to be conclusive that IgM titer increases rapidly within the first 2 weeks, persists in the following 1 to 2 weeks as the virus is being cleared, and declines by the 4th week after illness onset as the virus nucleic acid turns negative [1, 65]. Therefore, the decline of IgM may be an indicator of virus clearance, which may help determine the true nucleic acid conversion negative in conjunction with RT‐PCR testing. It could serve as a criterion for discharge and in ending quarantine, especially for mildly symptomatic or asymptomatic cases [1]. The IgM level showed heterogeneity within the group of deceased cases, and some patients had very high IgM levels which might be in the active status of the disease or very low IgM levels due to the long disease course. The increased IgM level in the deceased case group might be related to the higher disease severity in these patients and indicate a poor prognosis. Alternately, cytokine storm, severe immune dysfunction, and other comorbidities might be the important risk factors in these cases [21, 65-68].
Hsueh et al., [57] reported that seroconversion for IgG (mean 10 days) occurred simultaneously, or 1 day earlier, than that for IgM and IgA (mean 11 days for both). IgG could be detected as early as 4 days after the onset of illness. The earliest time at which these three antibodies reached peak levels were similar (mean 15 days). A high IgG level (1:800) could persist for > 3 months.
Long et al., [46] reported that Seroconversion for IgG and IgM occurred simultaneously or sequentially. After seroconversion, IgM and IgG titers were plateaued within 6 days. After 17-19 days of the onset of COVID-19 symptoms, a positive virus-specific IgG was reached 100%, while after 20-22 days of the onset of COVID-19 symptoms, a positive virus-specific IgM reached a peak of 94.1%. Three weeks after the onset of the sympatoms of COVID-19, the virus-specific IgM and IgG antibody titers were increased in patients [46].
Jin et al., [16] reported that the sensitivities of serum IgM and IgG antibodies to diagnose COVID-19 were 48.1% and 88.9%, and the specificities were 100% and 90.9%, respectively. In the COVID-19 group, the IgM-positive rate increased slightly at first and then decreased over time; in contrast, the IgG-positive rate increased to 100% and was higher than IgM at all times. However, the median IgG titer after conversion to virus-negative was double that before, and the difference was significant. The authors concluded that viral serological testing is an effective means of diagnosis for SARS-CsoV-2 infection.
Hou et al., [21] reported that IgM levels increased during the first week after SARS-CoV-2 infection, peaked for 2 weeks and then reduced to near-background levels in most patients. The immunoglobulin M antibody levels were slightly higher in deceased patients than recovered patients, but, in these groups, the immunoglobulin G antibody levels did not significantly differ. The authors concluded that quantitative detection of IgM and IgG antibodies against SARS-CoV-2 quantitatively has potential significance for evaluating the severity and prognosis of COVID-19.
Zhang et al., [52] found that the IgM and IgG positive rates were 50% and 81% on day 0 (the day of first sampling) and increased to 81% and 100%, respectively, on day 5. The IgG-positive rate was consistently higher than the IgM-positive rate, and this phenomenon was also observed in the study by Jin et al., [16] and Zhang et al., [52].
Liu et al., [53] observed that the IgM antibody response to SARS-CoV-2 occurred earlier and peaked earlier than the IgG antibody response; the IgM antibody response began to decline at week 3 of the illness, while the IgG antibody response persisted and was maintained in patients with COVID-19; and severe cases of COVID-19 tended to have a more vigorous response in both IgG and IgM antibodies to COVID-19 illness. Importantly, the timing of IgM and IgG antibody occurrence in patients varies greatly, and this variation in timing may be associated with age as well as comorbidity [53, 69]. More care needs to be taken when using levels of anti-SARS-CoV-2 antibodies to make a clinical diagnosis of COVID-19 or determine discharge criteria [53].
Circulating ferritin, CRP, and D-dimers were reported to be expressed to a similar extent or more robustly expressed in COVID-19 compared with other acute states [70]. The results current study showed that patients with COVID-19 had a significant increase in serum CRP during COVID-19 Virus Infection among COVID-19 patients at 0 day, 14 days, and 21 days compared with the controls. These results run parallel to the results of the previous studies [28, 53, 65, 71, 72]. The CRP was elevated in 65% of COVID-19 patients on admission and elevated in 93.9% of severe COVID-19 patients [28, 53]. CRP levels are strong biological indicators to represent the severity of the COVID-19 infection. CRP seems to be one of the first biomarkers to show physiological complications in COVID-19 patients. In a study, CRP was elevated in 60.7% of patients [71]. A cut-off of >10 mg/L for CRP is a predictor of poor outcome [44]. A retrospective study showed that a CRP level of 26 mg/L could serve as a cut-off to predict progression to severe disease [65]. Twenty-six studies in the second analysis showed significantly higher CRP in severe COVID-19 compared to non-severe COVID-19 [44, 73, 74]. C-reactive protein (CRP) levels are increased in COVID-19 patients and it has been shown that survivors had median CRP values of approximately 40 mg/L, while non-survivors had median values of 125 mg/L, indicating a strong correlation with disease severity and prognosis [45, 75]. CRP levels in COVID-19 patients who died were much higher than in patients who survived [28, 66]. The increase in CRP is strongly associated with COVID-19 severity and critical condition [28, 72].
Elevated D-dimer levels are very frequently seen in patients with COVID-19. Several meta-analyses have shown that D-dimer levels have prognostic value and correlate with disease severity and in-hospital mortality [73]. D-dimer can be an early marker to guide the management of Covid-19 patients [74]. Correlations of abnormal coagulation parameters with poor prognosis have been observed. Non-survivors have shown significantly higher levels of plasma D-dimers compared to survivors [45, 76]. Coagulopathy and overt disseminated intravascular coagulation appear to be associated with high mortality rates. Among the coagulation parameters, D-dimer elevation > 1 ug/L was the strongest independent predictor of mortality [5, 45].
The present study showed that coronavirus infection caused a significant (P<0>) increase in the serum D-dimer levels compared with the healthy control individuals. This result is similar to the study of Guan et al., [71] who reported that the d-dimer level was significantly elevated among non-survivors compared to survivors. Also, Huang et al. [44] reported that COVID-19 patients with 0.5 μg/mL or higher levels of d-dimer on admission need critical care support. Previous studies showed that d-dimer levels were higher in non-survive COVID-19 patients compared to survive ones [28, 76]. D-dimer on admission upper than 2.0 μg/mL can predict mortality in hospitals among COVID-19 patients. The d-dimer level can be a basic and helpful biomarker to identify the patients with poor prognosis in the early stages and help to the management of COVID- 19 patients [28, 77].
Viral clearance is the golden standard for defining the recovery of COVID-19 infections and predicting hospital length is extremely vital in the COVID-19 pandemic due to the lack of medical resources. Thus, authors suppose ferritin could act as both an effective discriminator for severity of illness and a predictor for prognosis [33, 66]. Ferritin is an intracellular protein that contains iron and is the major form of iron stored in the cells. Although this protein is found in most tissue and organs, small amounts are secreted into the blood and are the carrier of iron. Ferritin is used as an indirect marker of the total amount of iron stored in the body [28, 78]. Ferritin concentration increases significantly during infection or cancerous conditions. Also, ferritin is an acute phase reactant that rises in the course of the disease [28, 79].
The current study showed that coronavirus infection caused a significant (P<0>) increase in the serum Ferritin levels compared with the healthy control individuals. This result is similar to the result of the study of Dahan et al., [80] who reported that a significant increase in ferritin levels was demonstrated in patients with moderate and severe disease, compared to patients with mild disease (P = 0.006 and 0.005, respectively). Severe patients had significantly higher levels of ferritin (2817.6 ng/ml) than non-severe patients (708.6 ng/ml) P = 0.02. Caoet al., [33] reported that patients with elevated ferritin levels (>200 ng/mL) had a higher incidence of severe illness when compared with those with normal ferritin levels (≤ 200 ng/mL) (50.0% vs 2.9%). In addition, the severity of illness manifested a significantly higher level of ferritin as compared with non-severe ones (median 921.3 vs 130.7 ng/mL, p < 0>
Also, Zhou et al., [5] found that ferritin levels were elevated in cases of COVID-19 with fatal outcomes compared with survivors. Li et al., [81] found that significantly elevated ferritin levels in patients with severe COVID-19. A decrease in ferritin levels was not seen along with patient improvement. Therefore, it was suggested that it is a sensitive marker of severe COVID-19, but it cannot be used for disease assessment. Al-Samkari et al., [82] recorded that elevated ferritin, and CRP were higher in patients with thrombotic complications. This knowledge thus suggests that elevated ferritin level is a marker of severe COVID-19 and is associated with thrombotic complications [39]. In addition, Lin et al., [83] reported that Chinese patients with severe Sars-CoV2 disease showed higher levels of serum ferritin than patients with a not severe one, confirming data from other authors on Chinese [84, 85] and Caucasian populations [86, 87]. Studies on ferritin levels in COVID-19 patients have yielded equivocal results. It is not clear whether it is a bystander or a true characteristic of the disease [88]. Two retrospective studies have reported the minimal role of ferritin in predicting ICU admission and the need for ventilation and failure in predicting mortality [83, 89]. But another study and a meta-analysis showed findings to the contrary; ferritin levels could predict severe disease and mortality ([44, 83]. Elevation of ferritin levels may be due to secondary haemophagocytic lympho-histiocytosis (sHLH) and cytokine storm syndrome that has been reported in severe COVID-19 patients. Based on body temperature, organomegaly, blood cell cytopenia, and ferritin levels, a predictive H-score has been proposed to estimate the risk of developing secondary haemophagocytic lymphohistiocytosis [45, 90]. Serum levels of ferritin progressively increased with the severity of the disease and correlate with poor prognosis in COVID-19 patients. Increased ferritin levels could be indicative of a strong inflammatory reaction in COVID-19 and recent studies suggest that increased levels of circulating ferritin levels play a critical role by contributing to the development of a cytokine storm [91, 92], resembling macrophage activating syndrome [93]. Ferritin is a key mediator of immune dysregulation, especially under extreme hyperferritinemia, via direct immune-suppressive and pro-inflammatory effects, contributing to the cytokine storm [94, 95]. Laboratory findings in patients with severe COVID-19 showed data consistent with cytokine storm involving elevated inflammatory markers, including ferritin, which has been associated with critical and life-threatening illness [90].
It can be concluded that coronavirus infection caused a significant increase in IgM, IgG, D-dimer, CRP, and Ferritin levels at different periods compared to the controls. Further studies are needed to confirm these results. COVID-19 Specific Immunoglobulin's and Some Inflammatory factors in COVID-19 Patients These changes in IgM, IgG, D-dimer, CRP, and Ferritin levels during COVID-19 Virus Infection among COVID-19 patients may help the clinicians to better understand the COVID-19 and provide more clinical treatment options.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
