
Case Report | DOI: https://doi.org/10.31579/2768-2757/083
1 Emergency Department, UKRIDA Hospital, Jakarta, Indonesia, 11510.
2 Department of Internal Medicine, UKRIDA Hospital, Jakarta, Indonesia, 11510.
3 Department of Surgery, UKRIDA Hospital, Jakarta, Indonesia, 11510.
*Corresponding Author: Michael Chandra Sarsono, Emergency Department, UKRIDA Hospital, Jakarta, Indonesia, 11510.
Citation: Michael C. Sarsono, Roy A. Pandapotan, Erwin S. Wahab, (2023), Valentino’s Syndrome in Acute Pancreatitis Female Patient: A Case Report with Literature Review. Journal of Clinical Surgery and Research, 4(4); DOI:10.31579/2768-2757/083
Copyright: © 2023, Michael Chandra Sarsono. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 June 2023 | Accepted: 09 June 2023 | Published: 19 June 2023
Keywords: acute pancreatitis, appendicitis, sepsis, case report
Introduction:
Valentino’s syndrome is an unusual right iliac fossa pain due to perforation of a duodenal peptic ulcer through the paracolic sulcus leading to local irritation. The aim of this study is to report a case of Valentino’s syndrome from acute pancreatitis with a brief literature report.
Case Presentation:
A 50-year-old lady presented with diffuse irradiated abdominal pain and swelling of about 6 h duration, associated with nausea, vomiting, and inability to flatus. There was positive upper abdominal and right iliac fossa tenderness. The abdominal computed tomography (CT) scan showed acute pancreatitis appearance with fat stranding and fluid collection from the peripancreatic to the right lower quadrant. Serum amylase and lipase were elevated. Therefore, the initial diagnoses were acute pancreatitis and appendicitis. Conservative management was done because of poor hemodynamics, laboratory work-up, and the lack of medical speciality to perform surgery. The patient was then transferred to another hospital with adequate facilities.
Conclusion
Valentino’s syndrome from acute pancreatitis is an extremely rare case, presented with vague symptoms, diagnosed by abdominal CT scan. Clinical diagnosis could be challenging for clinicians.
Acute pancreatitis is an acute inflammation of the pancreas parenchyma, contributing as the leading gastrointestinal cause of hospitalization in the United States [1]. Several etiologies are related to acute pancreatitis, with the most common causes including gallstones, alcohol use, endoscopic retrograde cholangiopancreatography (ERCP), metabolic conditions, infection, and hypertriglyceridemia [2]. The underlying mechanism of acute pancreatitis is due to the premature activation of trypsinogen to trypsin within the acinar, leading to extensive tissue damage and the initiation of the inflammatory cascade. Patients with acute pancreatitis commonly have moderate to severe abdominal pain in the epigastrium accompanied by nausea, vomiting, and anorexia [3]. Although the involvement of the appendix in acute pancreatitis is quite rare, its existence appears to be challenging for clinicians to determine the best treatment choice for the patient. A similar case was known as Valentino’s appendix or Valentino’s syndrome, where acute appendicitis was found to be related to a perforated gastric or duodenal ulcer with its content leaking through the paracolic gutters into the right iliac fossa causing local peritoneal irritation. In accordance with CARE guidelines, we reported a rare case accompanied by a brief literature review of Valentino’s syndrome as a complication of acute pancreatitis in a middle-aged woman [4].
1.1. Patient information
A 50-year-old married housewife presented with 6 h of diffuse abdominal pain and swelling. Dull irradiated persistent abdominal pain was reported with a visual analog scale (VAS) of 10. The patient also reported nausea and three episodes of vomiting. The patient was unable to flatus. This patient had visited the local community health center 2 hours prior to admission. She was given sucralfate and lansoprazole without an improvement in VAS. History of hypertension was recorded, with captopril 25 mg once daily. The patient was non-alcoholic. Other family, drug, past medical and surgical history were denied by the patient.
1.2. Clinical findings
The patient was conscious and able to respond. Hypertension (157/97 mmHg) and tachypnea (22 x/minute) were recorded, with other normal vital signs. Abdominal examination found ascites with abdominal circumferences of 110 centimeters. Upper abdominal tenderness was positive, without muscle guarding or rigidity. Right iliac fossa rebound tenderness was positive. The bowel sound remained present. Urinary production was decreased.
1.3. Diagnostic assessment
A whole abdomen computed tomography (CT) scan was performed, with the results: hepatomegaly with fatty liver appearance, acute pancreatitis appearance with fat stranding and fluid collection from peripancreatic to the right lower quadrant, a small stone and complex kidney cyst in the right kidney, appendicitis with minimal fat stranding, minimal ascites in peripancreatic space to the right lower quadrant and paravesical space. Marked white blood cells elevation (20,040 /uL), thrombocytes (440,000 /uL), serum amylase (2,133 U/L with normal range 28–100 U/L), serum lipase (1,658 U/L with normal range 13–60 U/L), creatinine (1.05 mg/dL), and non-fasting glucose (250 mg/dL) were reported. Prolonged prothrombin time (PT) (> 70.0) and prolonged activated partial thromboplastin time (aPTT) (> 120) were reported. An anteroposterior chest X-ray found cardiomegaly. Hence, the patient was admitted with acute pancreatitis, appendicitis, hypertensive heart disease, hyperglycemia, complex kidney cyst with a small stone, and mild ascites.
1.4. Therapeutic intervention
The patient went nothing by mouth (NPO) with total parenteral nutrition; additionally, a nasogastric tube (NGT) and a urinary catheter were inserted. Conservative management with antibiotics, insulin, and symptomatic treatments was commenced. Initially, a combination of 750mg levofloxacin and 2-gram ceftriaxone were used once daily. After acute pancreatitis was confirmed, the antibiotics used were changed into 1-gram meropenem tid. Multimodal pain management using 1 gram paracetamol, 10 mg hyoscine-N-butyl bromide, 30 mg ketorolac, and 50 mg tramadol were used at the beginning. However, these medications were ineffective; thus, 30 mcg/h fentanyl drips were used. 1 U/h rapid-acting insulin drip with a correction dose was used to control the hyperglycemia (target glucose of 100 to 180 mg/dL).
1.5. Follow-up and outcomes
No surgical procedure was attempted due to the absence of the digestive surgeon, prolonged PT and aPTT, and unstable hemodynamics. This patient was planned to be transferred to a higher healthcare center with an available digestive surgeon. After 12 h of observation in the general ward, the patient's vital signs worsened; thus, the patient was moved to the high-care unit (HCU). After 24 h in HCU, vital signs were stable, the abdominal circumference was reduced to 106 cm, abdominal pain was reduced to VAS 8–9, and the patient was transferred to another hospital for further surgical and non-surgical treatments. There were no adverse or unanticipated events discovered during treatment.
Valentino’s syndrome was named after the silent idol, Rudolph Valentino, who underwent appendectomy surgery at New York Polyclinic Hospital in 1926 [5, 6]. His autopsy report revealed a perforated ulcer, later developed peritonitis and multi-organ failure leading to death [6]. The incidence of Valentino’s syndrome remains unknown. Valentino’s syndrome occurred due to a perforated peptic ulcer, with gastric or duodenal content leaking through the right paracolic gutter to the right iliac fossa, leading to local peritonitis and a mildly inflamed appendix [7]. The most common presenting signs and symptoms are right iliac fossa tenderness and lower abdominal pain [8]. This finding should keep clinicians more vigilant regarding the possibility of Valentino’s syndrome. Although this eponym was related to peptic ulcer perforation, this case report shows a similar case of Valentino’s syndrome secondary to acute pancreatitis. Only one study reported Valentino’s syndrome secondary to acute pancreatitis [9]. In acute pancreatitis, localized destruction is due to premature activation of the trypsinogen to trypsin, causing extensive tissue damage and Damage Associated Molecular Patterns (DAMPs) release. Following the injuries, peripancreatic fluid collection can be found [3]. This fluid collection can potentially track along the mesenteries and paracolic gutters into the right iliac fossa causing local irritation [9]. Acute pancreatitis is the inflammation of the pancreas parenchyma with a high mortality rate (up to 20%) [3]. The annual incidence of acute pancreatitis in the United States ranges from 600 to 700 per 100,000 population, and it is believed to be rising over time [3, 10]. The most common causes of acute pancreatitis include gallstones, alcohol use, and hypertriglyceridemia [3]. Patients with acute pancreatitis commonly experience moderate to severe upper abdominal pain associated with nausea and anorexia. According to the Revised Atlanta Classification, the diagnosis of acute pancreatitis requires at least 2 of 3 criteria: (1) Serum lipase or amylase is three times the normal upper limit; (2) Abdominal pain is consistent with pancreatitis; (3) Abdominal imaging is consistent with acute pancreatitis [11]. Managing acute pancreatitis requires keeping nothing by mouth until abdominal pain, vomiting, nausea, loss of appetite, and ileus improve; early aggressive fluid resuscitation; pain management according to the World Health Organization (WHO) analgesic ladder; and antibiotics if needed [3]. There was a consideration in the past that Opioids could trigger the spasm of the sphincter of Oddi. However, a recent Cochrane review shows no difference between opioids and other analgesics regarding the risk of complications and adverse events [12]. Further management is directed at the etiology of acute pancreatitis, such as early cholecystectomy, early ERCP, and hypertriglyceridemia control. Acute peripancreatic fluid collection usually resolves spontaneously, with less than 10% results in pancreatic pseudocyst. Endoscopic or percutaneous drainage of the pancreatic pseudocyst is only recommended in the case of infection or rapid enlargement of the pseudocyst. Antibiotics are required if there is a high suspicion of infection, and the recommended antibiotic regimen includes carbapenem alone or a combination of quinolone, cefepime, or ceftazidime with metronidazole. A surgical necrosectomy is performed if the patient continues deteriorating [3]. In conclusion, Valentino’s syndrome secondary to acute pancreatitis is a rare presentation, with vague symptoms, diagnosed by abdominal CT scan and laboratory findings. Similar to Gapp et al. management, this case was initially managed by keeping patients NPO, step-ladder pain management, and carbapenem antibiotic [3]. Unfortunately, the surgical approach could not be performed due to the lack of a digestive surgeon and the facility in our hospital. Therefore, initial management and stabilization are essential before transferring the patient to another hospital.

Figure 1: Abdominal CT scan showed acute pancreatitis with appendicitis.
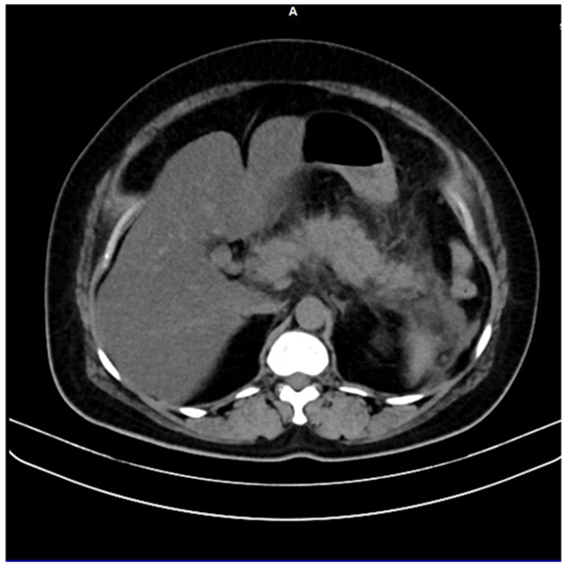
Figure 2: Abdominal CT scan showed an enlarged irregular pancreas with peri pancreatic fluid collection and fat stranding.
2.1. Patient perspective
The patient was desperately in pain before the intervention. The patient was anxious regarding the surgery plan, yet she agreed. Although the reduction of the VAS score was insufficient, she was happy and satisfied with the progress.
Conflict of interest
The authors declare there is no conflict of interest.
This case report did not receive any funding or grants.
Informed consent was obtained from the patient to use relevant information for publication in the journal.
MCS: conceptualized the case report, involved in case management, wrote the manuscript, reviewed the literature, participated in the discussion, and followed up.
RAP: involved in case management, wrote the manuscript, reviewed the literature, participated in the discussion, followed up, and gave final approval of the manuscript.
ESW: involved in case management, wrote the manuscript, reviewed the literature, participated in the discussion, followed up, and gave approval of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
