
Research Article | DOI: https://doi.org/10.31579/2578-8965/236
1Pelvic Rehabilitation Medicine Clinical Research Foundation, West Palm Beach, FL, USA.
2The Feinstein Institute for Medical Research, Northwell Health, Manhasset, NY, USA.
*Corresponding Author: Katherine Wolfrum, Pelvic Rehabilitation Medicine Clinical Research Foundation, West Palm Beach, FL, USA.
Citation: Allyson Shrikhande, Lolasri Rampally, Katherine Wolfrum, Rachael Haverland, Kimberlee Leishear., et al. (2024), Vaginismus: Results from Treatment with the PRM Protocol™, J. Obstetrics Gynecology and Reproductive Sciences, 8(7) DOI:10.31579/2578-8965/236
Copyright: © 2024, Katherine Wolfrum. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 August 2024 | Accepted: 04 September 2024 | Published: 10 September 2024
Keywords: pelvic medicine; vaginismus; pelvic floor therapy; patient reported outcomes; pain management interventions
Background/Aim: Vaginismus, a condition characterized by involuntary pelvic floor muscle spasms, presents considerable challenges in diagnosis and treatment, impacting sexual health and quality of life. This study evaluates the efficacy of a novel pelvic peripheral nerve block and trigger point injection protocol (the PRM Protocol™) in addressing vaginismus.
Materials/Methods: A retrospective chart review of 961 patients diagnosed with vaginismus, aged 18-76, was conducted. Participants underwent a 6-week treatment protocol involving neuromuscular treatment and physical therapy.
Results: Outcome measures included the Visual Analog Scale (VAS) pain scale, the Functional Pelvic Pain Scale (FPPS), and the modified Sexual Function Profile (SFP). Post-treatment, there were notable decreases in VAS by 46%, FPPS by 51% and a 25% improvement in SFP. Additionally, opioid use decreased by 22%, ER visits decreased by 18%, and absenteeism and presenteeism decreased by 56% and 68%, respectively. No adverse events were reported.
Conclusion: The study highlights the comprehensive efficacy of the PRM Protocol™ in alleviating vaginismus symptoms and improving patient outcomes. Implementation of this protocol offers a transformative opportunity to enhance patient care and optimize resource allocation in managing vaginismus, warranting further research and clinical application.
Vaginismus is a sexual health condition characterized by involuntary muscle spasms or contractions of the pelvic floor muscles surrounding the vagina1. These spasms can make any form of vaginal penetration, including sexual intercourse, gynecological examinations, or tampon insertion, painful or even impossible [1]. It is important to note that vaginismus is not a conscious choice or a result of psychological resistance; instead, it is an involuntary physiological response. Although a long-standing condition, first defined in 1862, research on the topic continues to be very limited[2]. Currently, vaginismus continues to affect somewhere between 5-17% of women, with reports on the prevalence varying[2].
The severity of vaginismus can vary, ranging from mild discomfort to extreme pain. The condition can have a significant impact on sexual relationships, causing emotional distress and anxiety for individuals experiencing it and their partners[1]. Vaginismus can be classified into primary or secondary categories. Primary vaginismus occurs when the condition has been present from the beginning of a person's attempts at vaginal penetration, while secondary vaginismus develops after a period of normal sexual function[2]. The causes of vaginismus are complex and may include psychological factors, past traumatic experiences, relationship issues, or medical conditions. Treatment approaches often involve a combination of physical therapy, counseling, and, in some cases, medical interventions2. Successful treatment typically requires a comprehensive and individualized approach addressing both the physical and psychological aspects of the condition[3]. If someone is experiencing symptoms of vaginismus, seeking the guidance of multiple healthcare professionals, such as gynecologists or sex therapists, is crucial for accurate diagnosis and tailored treatment plans[2].
The traditional indicator of vaginismus has been involuntary muscle spasms leading to sexual dysfunction[4]. However, both the American College of Obstetrics and Gynecology (ACOG) and the Diagnostic and Statistical Manual of Mental Disorders (DSM) V-Text Revision (TR) have defined vaginismus as a part of genito–pelvic pain/penetration disorder. ACOG defines genito-pelvic pain/penetration disorder as a combination of dyspareunia and vaginismus5. In the most recent DSM-V-TR, vaginismus is listed as a symptom within the category of “genito-pelvic pain/penetration disorder, “which is difficulty in one of the following: (a) vaginal intercourse/penetration, (b) genito-pelvic pain, (c) fear of vaginal intercourse/penetration/pain, or (d) heightened pelvic floor muscle tension during attempted penetration5. This is an update from the prior definitions of vaginismus used by DSM, which was defined as an involuntary contraction of muscles, making penetration painful or impossible [5,6]. The International Classification of Diseases (ICD)-11 classifies vaginismus as a sexual pain-penetration disorder [7].
Due to the lack of a clear definition for vaginismus, despite its long history, the etiology and treatment for vaginismus are varied. Currently, several treatment modalities are employed to address vaginismus, reflecting the complex nature of the disorder. Pelvic floor physical therapy is a common approach, focusing on the relaxation and strengthening of the pelvic floor muscles through targeted exercises and interventions [2]. General psychotherapy aims to address any underlying psychological issues or trauma that may contribute to vaginismus, fostering a holistic approach to treatment [2]. Additionally, pharmacological therapies, such as muscle relaxants or anesthetics, may be considered in some instances to alleviate symptoms[2]. Sex/cognitive behavioral therapy (CBT) plays a pivotal role in modifying negative thought patterns and behaviors associated with vaginal penetration, providing a structured and goal-oriented therapeutic approach2.
The available treatment options for vaginismus are diverse. However, the research literature frequently encounters methodological difficulties, such as small sample sizes and the necessity for long-term follow-up data. This study sought to address these concerns by conducting a comprehensive investigation into the efficacy of an outpatient neuromuscular treatment protocol. Notably, the research utilized a large-scale approach to enhance the study's statistical power, providing more reliable insights into the effectiveness of the novel treatment protocol. The focus of the study was explicitly directed toward treating myofascial pain and dysfunction commonly observed in vaginismus patients, offering a nuanced and targeted intervention for this intricate condition. The substantial sample size contributes to the validity and generalizability of the study's findings, shedding light on potential advancements in the treatment landscape for vaginismus.
The study included 961 participants aged 18 to 76 years old diagnosed with vaginismus who sought treatment at an outpatient pelvic rehabilitation practice between April 2021 and December 2022. The demographic and clinical characteristics of the patients are depicted in Figure 1 and Figure 2. The inclusion criteria for the retrospective chart review included the completion of the PRM Protocol™, which consists of a series of pelvic peripheral nerve blocks and trigger point injections; an internal examination with necessary workup; and specific findings such as trigger points, pelvic floor hypertonia, tenderness upon palpation of the levator ani sling during an internal examination; and tenderness along the pudendal nerve and posterior femoral cutaneous nerve at Alcock's canal and obturator canal bilaterally internally.
Exclusion criteria for the retrospective chart review included active infection, malignancy, pregnancy, pudendal nerve entrapment syndrome, and incomplete patient-reported outcome measures.
The Institutional Review Board (IRB) approved the six-week neuromuscular office-based treatment called the PRM Protocol™ (IRB# 17‐0761) designed for patients diagnosed with vaginismus. The treatment involved pre-medication with diclofenac 75 mg PO, pre-treatment with atopical anesthetic spray, and weekly external ultrasound-guided trigger point injections of Lidocaine 1% into the pelvic musculature. A global injection targeted specific muscles of the levator ani sling using a flexible, 6‐inch, 27‐gauge needle injected from the subgluteal posterior approach under ultrasound guidance.
Simultaneous ultrasound‐guided peripheral nerve blocks of the pudendal nerve at Alcock’s canal and the posterior femoral cutaneous nerve were administered. The initial treatment included dexamethasone with Lidocaine 1%, followed by subsequent appointments with normal saline and Lidocaine 1% for nerve blocks. Patients resumed normal activities immediately after treatment.
During the PRM Protocol™, patients did pelvic floor physical therapy either at a local clinic or at home virtually, with the goal of downtraining the pelvic floor musculature and the peripheral and central nervous systems. Patients also simultaneously participated in mindfulness, meditation, and deep breathing exercises at home alone or through PRM’s mindfulness meditation course, “Retrain Your Pelvic Pain.”
Six weeks after the final treatment, participant response to the PRM Protocol™ was measured. Primary outcome measures included Visual Analog Scale (VAS) scores for pelvic pain concentration and Functional Pelvic Pain Scale (FPPS) scores to assess pelvic functionality. Patients provided their average pain intensity ratings on a scale of 1 to 10 for the Visual Analog Scale (VAS) based on the preceding 24 hours. The overall Functional Performance Pain Scale (FPPS) score is derived by summing sub-scores across distinct categories, including working, intercourse, sleeping, walking, running, lifting, bladder, and bowel. Within each category, scores range from 0 to 4, where 0 signifies normal performance and 4 indicates substantial debilitation, yielding a cumulative FPPS score ranging from 0 to 32.
Secondary outcome measures encompass a modified version of the National Institutes of Health Sexual Function Profile (SFP), featuring three questions focused on sexual well-being that are totaled to derive an overall Modified SFP score. Additional perspectives on a patient's well-being are captured through Absenteeism and Presenteeism questionnaires, along with patient-reported data on the frequency of opioid use and Emergency Room (ER) visits. A retrospective review of medical records was conducted to analyze the outcome measures. The Wilcoxon signed-rank test, suitable for non-normally distributed paired samples, was employed to analyze VAS, FPPS, and SFP scores. Differences in Absenteeism and Presenteeism were assessed using a Chi-squared test, while changes in opioid use and ER visits were examined using a McNemar test for paired proportions.
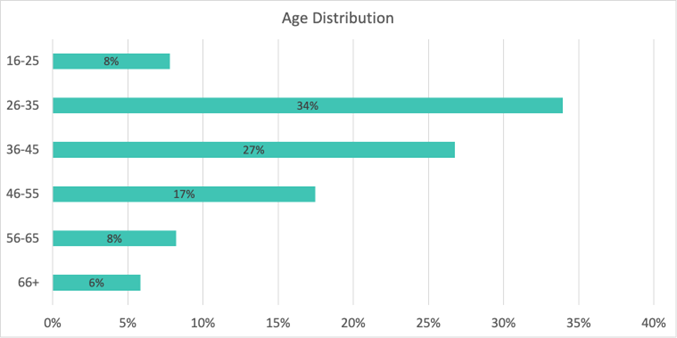
Figure 1: Age Distribution of Patients.
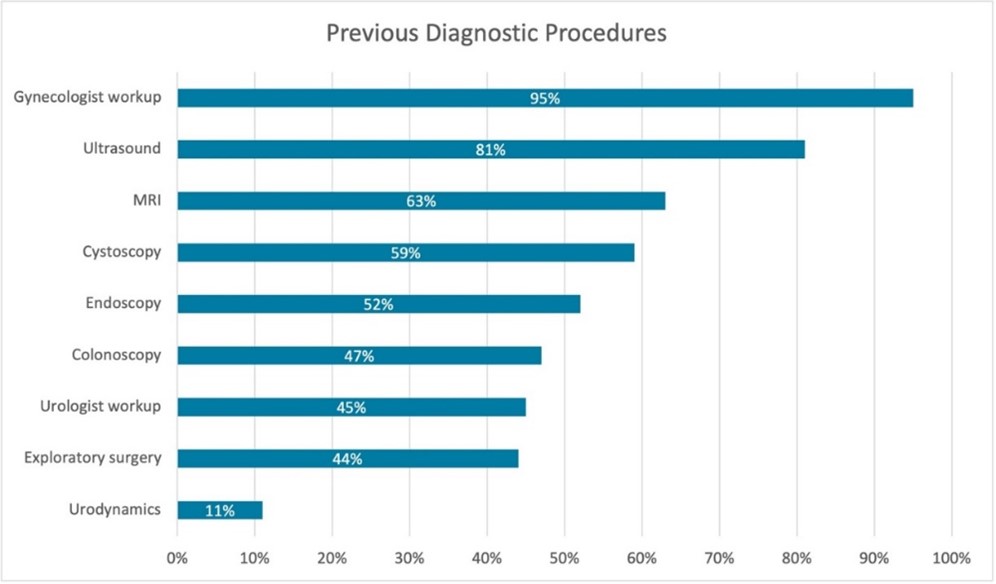
Figure 2: Previous Diagnostic Procedures.
Significant statistical findings were observed across various outcome variables. No adverse events were reported from the PRM Protocol™. The 1-10 Visual Analog Scale (VAS), Functional Pelvic Pain Scale (FPPS), a modified version of the Sexual Function Profile (SFP), as well as measures of opioid use, Emergency Room visits, Absenteeism, and Presenteeism (Figures 4-9). Measures were assessed during participants' New Patient (NP) and their six-week follow-up (6-WK FU) appointments after completing the initial protocol series. SPSS v.29 was used for analysis, with α = 0.05 as the cutoff for all analyses.
VAS pain levels decreased by 46% from 7.2 (SD 2.46, CI = 6.93 – 7.28) to 3.9 (SD 2.49, CI = 3.61 – 3.92) (p < .001). FPPS total scores decreased by 51% from an average of 9.6 (SD 5.23, CI = 9.52 – 9.68) to an average of 4.7 (SD 5.82; CI = 4.58 – 4.79) (p < .001). Improvements in all FPPS categories were statistically significant (p < .001), with the largest decreases in intercourse (47%), bowel function (45%), bladder function (44%), and sleep (42%).
Our modified SFP asked the following three questions: “In the past 30 days, how would you describe the comfort of your vagina during sexual activity?” “In the past 30 days, how often have you had difficulty with sexual activity because of discomfort/ pain in your vagina?” and “In the past 30 days, how often have you stopped sexual activity because of discomfort/ pain in your vagina?” Responses were scored 0-5 and summed for an average improvement of 25% (p = <0.01).
For those who underwent the PRM Protocol™, 38% of patients reported using opioids for their vaginismus-related pain at their first appointment. 29% of patients reported having gone to an Emergency Room for their vaginismus-related pain at their first appointment. These proportions reduced to 16% and 11%, respectively, at their six-week follow-up appointment after undergoing the PRM Protocol™. This is a 22% decrease in opioid use and 18% decrease in patients visiting the ERER (both p< 0.01) for the treatment group. Absenteeism, defined by at least one day of work missed in the past three months due to pelvic pain, decreased by 56%. Presenteeism, defined by at least 1 hour of work productivity being disturbed by pelvic pain in the past three months, decreased by 68%.
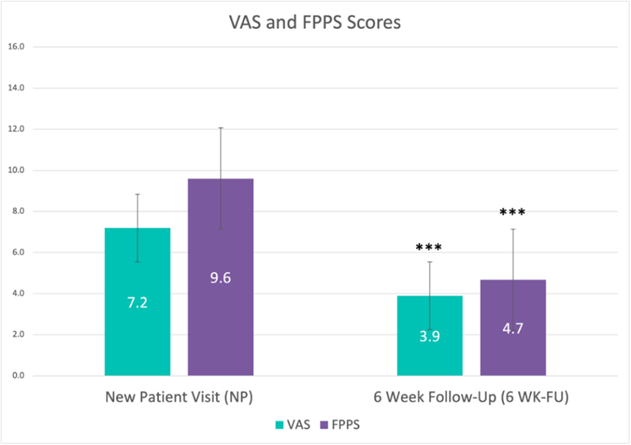
Figure 3: VAS and FPPS Scores Measured for Pelvic Pain Concentration in New patients (NP) and patients after 6 Week-follow (6WK-FU).
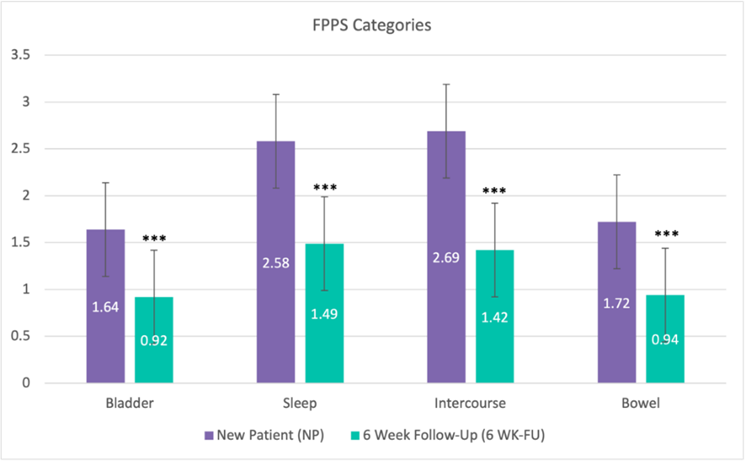
Figure 4: Significant improvements in FPPS Categories in New patients (NP) and patients after 6 Week-follow (6WK-FU).
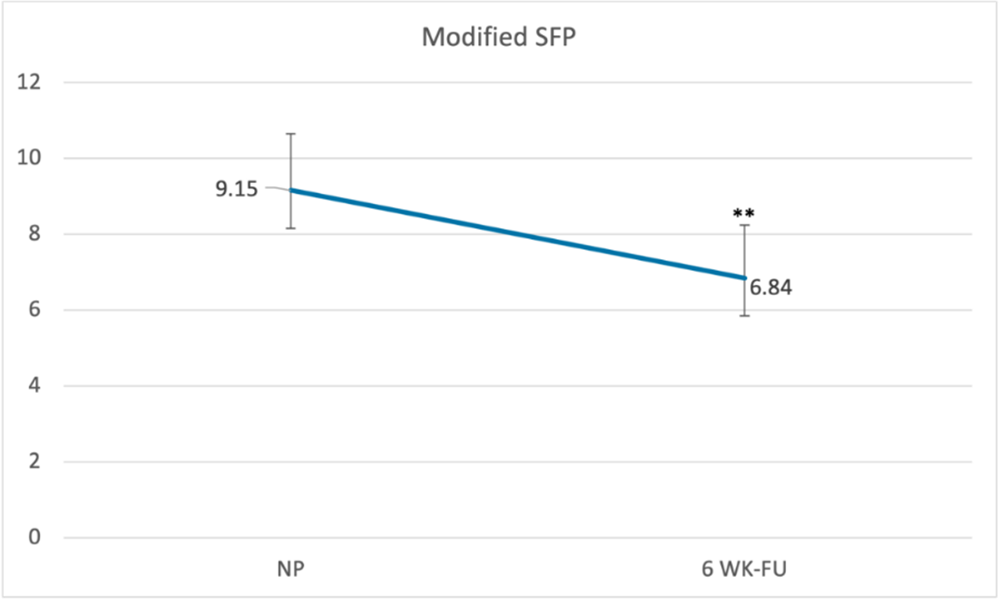
Figure 5: SFP measured for patients at NP and 6 WK-FU.
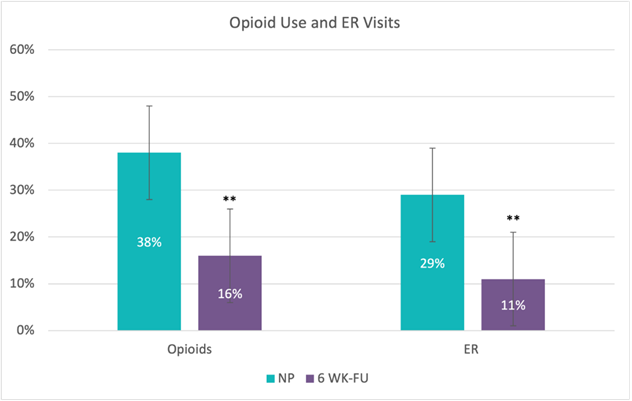
Figure 6: Opioid Use and ER Visits.
Vaginismus, a condition often characterized by complexity and misunderstanding, presents considerable challenges in both diagnosis and treatment. Determining the accurate prevalence of vaginismus is difficult due to underreporting and the private nature of sexual health concerns. Despite these obstacles, vaginismus is not uncommon, and its impact on individuals and their relationships can be profound, leading to emotional distress, strained relationships, and avoidance of sexual activities, thereby negatively affecting overall quality of life. The primary objective of this study was to evaluate the impact of the pelvic peripheral nerve block and trigger point injection protocol (the PRM Protocol™) on a wide range of outcome parameters, including pain, functionality, work productivity, quality of life, mental health, sexual health, and healthcare system utilization. It is noteworthy that the participants in this study reported an average pain duration of 9.5 years, underscoring the chronic and debilitating nature of vaginismus.
Significant improvements in Visual Analog Scale (VAS) pain levels were observed among patients, underscoring the efficacy of this approach in addressing the fundamental causes of nerve and muscle dysfunction. Myofascial dysfunction in the pelvic region is intricately linked to issues such as bowel, bladder, and sexual dysfunction, contributing to pelvic pain through the presence of myofascial trigger points[8]. The PRM Protocol™ employs ultrasound-guided trigger point injections in each muscle of the levator ani-sling to address the underlying myofascial pain and pelvic floor dysfunction. This intervention alleviates ongoing nociception, creating space for enhanced flow of pelvic peripheral nerves with reduced constriction and improved blood circulation[13].
Additionally, the PRM Protocol™ targets both peripheral and central sensitization, aiming to mitigate neurogenic inflammation, inhibit feedback loops from the peripheral to central nervous systems, and prevent cross-sensitization between the pudendal and posterior femoral cutaneous nerves9. Peripheral sensitization is managed through consecutive peripheral nerve blocks targeting the pudendal and posterior femoral cutaneous nerves9. The PRM Protocol™ employs two primary mechanisms for this purpose: 1) the reduction of neurogenic inflammation by locally administering dexamethasone to deplete substance P8 and utilizing repeated exposure to lidocaine 1%, which diminishes histamine release from mast cells, and 2) the desensitization of hyperactive peripheral nociceptors through repeated exposure to lidocaine 1%[10]. In addition to addressing peripheral sensitization, the PRM Protocol™ also focuses on central sensitization by treating associated pelvic neurogenic inflammation, effectively interrupting the feedback loop from the peripheral nervous system to the central nervous system [11]. It is crucial to note that the overlap in pain patterns and innervation between the pudendal and posterior femoral cutaneous nerves may lead to cross-sensitization, a phenomenon observed in the pelvic region where a sensitized structure can influence an adjacent, otherwise normal structure [12,13]. The PRM Protocol's™ multi-faceted approach, addressing myofascial dysfunction, pelvic floor dysfunction, and peripheral and central sensitization, demonstrates a comprehensive strategy for managing the intricate facets of vaginismus.
This study focused on assessing patients with vaginismus, aiming to establish a method for evaluating the severity of the condition and exploring effective treatment strategies for this specific group. A substantial cohort of patients with vaginismus actively participated in the study, providing a robust foundation for the research findings. The multimodal treatment approach, addressing both the physical and psychological dimensions of vaginismus, demonstrated a notable degree of success and safety, accompanied by a low recurrence rate. Significantly, the outcomes revealed that this comprehensive approach achieved pain-free intercourse successfully, even for patients with a history of long-term failures with alternative vaginismus treatments. The most notable enhancements were observed in symptoms related to intercourse, sleeping, and bladder function. The PRM Protocol™ specifically targets pelvic nerve inflammation and the pelvic muscles associated with both intercourse and vaginismus, leading to a reversal of pelvic neurogenic inflammation and a reduction in hypertonic pelvic floor conditions. This, in turn, results in decreased vulvar pain and improved functionality during intercourse.
A limitation of the study is its retrospective nature, preventing the use of randomized control groups and limiting the ability to evaluate the protocol's effectiveness compared to placebos. Consequently, individuals diagnosed with vaginismus often navigate a complex medical journey, seeking relief in the emergency room during severe pain episodes and undergoing unnecessary diagnostic procedures in addition to a series of unsuccessful surgical and non-surgical therapeutic interventions. It is crucial for the medical community to collaboratively establish a streamlined diagnostic and treatment protocol for vaginismus patients, benefiting both the individuals suffering from the condition and the healthcare system. Future research in a university context may address these limitations and contribute to a more comprehensive understanding of the studied phenomenon. Nevertheless, the findings from this study contribute valuable insights into the potential effectiveness and safety of the PRM Protocol™ in managing vaginismus, presenting a promising avenue for future research and clinical applications. As a complex and multifaceted condition, vaginismus necessitates a comprehensive and compassionate approach for successful diagnosis and treatment. Increased awareness among healthcare providers, coupled with open communication and support, can contribute to improved outcomes for individuals affected by vaginismus. Ongoing research and advocacy efforts are essential to destigmatize the condition, facilitate early intervention, and enhance the overall well-being of those living with vaginismus.
In conclusion, this research underscores the remarkable efficacy and safety of the PRM Protocol™ in alleviating distress among individuals aged 18-76 diagnosed with vaginismus. The substantial reductions observed in surgical interventions, medical treatments, diagnostic procedures, pain management interventions, opioid utilization, and emergency room visits bear significant clinical and economic implications. Integrating this protocol into healthcare practices presents a transformative prospect to enhance patient care, optimize resource allocation, and provide effective treatments for vaginismus. This study contributes valuable insights that advocate adopting the PRM protocol as a promising and impactful approach to addressing the challenges posed by vaginismus across diverse demographic groups.
The authors report no conflicts of interest in this work.
All authors contributed to the design and implementation of the research, to the analysis of the
Results, and to the writing of the manuscript.
Ethics approval and consent to participate
The protocol for this research project has been approved by an institution's suitably constituted Ethics Committee, and it conforms to the provisions of the Declaration of Helsinki. Committee of The Feinstein Institutes for Medical Research, Approval No. IRB# 17-0761. Our study does not have a clinical trial number, and consent forms were waived due to the study design.
The study was performed at Pelvic Rehabilitation Medicine, Atlanta, Chicago, Dallas, Houston, Miami, New York City, New Jersey, Michigan, and Washington DC. Patient data were gathered from these clinics.
This research received no external funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
