
Case Report | DOI: https://doi.org/10.31579/2642-9756/089
1*Department of gynecology and obstetrics Conjunto Hospitalar do Mandaqui, Brasil.
*Corresponding Author: Mauricio Sena-Martins, Department of gynecology and obstetrics Conjunto Hospitalar do Mandaqui, Brasil.
Citation: Mauricio de Sena Martins, Heloisa Fracalossi Frigini, Thaiane Silverio Batista, Roberto Lojelo, Fernando Zuccon e Silva s. (2021) Uterine Extra-Abdominal Exposure in the Management of Anterior Placenta Previa and Accreta to Proceed Hysterotomy. J. Women Health Care and Issues. 4(6); DOI:10.31579/2642-9756/089
Copyright: © 2021 Mauricio Sena-Martins, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 September 2021 | Accepted: 19 October 2021 | Published: 25 October 2021
Keywords: placenta previa; placenta accrete; hypovolemic shock; hysterectomy
The rates of placenta praevia and accreta are rising, probably as a result of increasing rates of cesarean delivery, as well as maternal age and assisted reproductive technologyIn this paper, we present a case report of a pregnancy complicated by anterior placenta praevia and accreta, in which the uterine extra-abdominal exposure technique was used to proceed the hysterotomy in the uterine fundus in order to avoid excessive bleeding and also to better evaluate the lower segment and consequent hysterectomy requirement. The main objective of this procedure is to describe a surgical technique which should guide the hysterotomy, in a position far enough away from the placenta site (fundus or posterior), in order to prevent bleeding complications in placental accreta disorders.
Placenta previa is a well-known obstetric complication in which the placenta is attached over the lower uterine segment. Placenta accreta is a condition first described in 1937 by Irving and Hertig as a placenta abnormally adhered to the uterine wall or part of it, in the total or partial absence of decidua, formerly known as morbidly adherent placenta, referring to the range of pathological adherence of the placenta, including placenta increta, placenta percreta, and placenta accreta [1]. The current terms for this condition refer to the Placenta accreta spectrum, abnormal placentation or just placenta accreta [2].
When both conditions are associated, the risk of obstetric hemorrhage and its complications, of use of endovascular procedures and of hysterectomy are increased, with 40% requiring more than 10 units of packed red blood cells and a maternal mortality rate as high as 7% [3].
Moreover, rates of placenta praevia and accreta are rising, probably because of increasing rates of cesarean delivery, as well as maternal age and assisted reproductive technology [4].
In this sense, previous knowledge of the site of adherent placenta through imaging exams may improve the cirurgic and endovascular management and possibly decrease its complications. [5]. The possibility of conservative management using fibrin sealant patch combined with uterine artery embolization, may be an alternative when there is a focal area of placenta praevia and accreta diagnosed intraoperatively [6]. The use of bakri balloon tamponade for this condition may preserve the uterus but fertility remain uncertain [7,8,9].
In this paper, we present a case report of a pregnancy complicated by anterior placenta praevia and accreta, in which the uterine extra-abdominal exposure technique was used to proceed the hysterotomy in the uterine fundus in order to avoid excessive bleeding and also to better evaluate the lower segment and consequent hysterectomy requirement.
The main objective of this procedure is to describe a surgical technique which should guide the hysterotomy, in a position far enough away from the placenta site (fundus or posterior). Another aim is to determine the hysterectomy type (supracervical or total) depending on the limits of the placenta previa spectrum in the anterior site. The use of visual inspection in a vertical position of the uterus can also help determine the need of other kinds of resources (urology, proctology or vascular) and may probably reduce intraoperative bleeding, with or without endovascular support in the Placenta accreta spectrum.
Patient’s consent was formally obtained.
A 43-year-old Brazilian woman, on her third pregnancy, with 2 previous cesarean sections, began pre-natal care around 20 weeks. At 32 weeks of pregnancy, an Ultrasound Doppler scan and MRI were performed and revealed a placenta accreta spectrum, characterized by loss of the normally continuous white line representing the bladder wall-uterine serosa interface, loss of the clear zone, myometrial thinning and abnormal vascularity, placental irregularity in vesicouterine space, suggesting placenta accreta [10] (Figure1). Immediately, an obstetric plan was made in order to obtain resources to prevent a possible hemorrhage and a complicated pelvic surgery, involving a multidisciplinary team (vascular, anesthetic and urology), and the delivery was scheduled. Two days before the scheduled cesarean section, at 36 weeks 6 days, the patient attended the obstetric emergency room with a history of one active antepartum bleeding episode and was immediately admitted.
We answered all the patient’s questions in the emergency room and the recommendation was to perform cesarean section, with arterial temporary blocking and hysterectomy as subsequent staged procedures to be done in the hybrid operation room. After her consent, the patient was forwarded to the operation room, two wide-bore cannula were inserted and blood was sent for a full blood count, and spinal anesthesia was performed. Frequent and ongoing dialogue between the vascular, obstetric, and anesthetic teams and the intraoperative nursing staff was established to provide all current information status, ongoing blood loss, and expectations about future blood loss. The vascular team bilaterally inserted balloon catheters through the common femoral arteries, into the internal iliac arteries to allow immediate cessation of blood flow to the pelvic arteries, if needed.

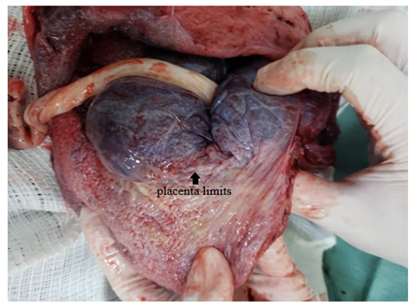
Obstetric team initiated the cesarean section through a Pnannenstiel skin incision. Abdominal findings revealed a placenta acretta spectrum, abnormal vascularity in the vesicouterine space, observed through the serosa, reaching the lower segment of the uterus. A maneuver to pull out the uterus was performed to attain uterine extra-abdominal exposure, and a fundus cesarean section was carried out (Figure 2). A breech delivery was done (Figure 3), leaving the placenta undisturbed in situ to perform the hysterectomy (Figure 4 and 5).



Before the beginning of the uterine artery ligature, the iliac balloons were inflated and kept inflated until the procedure was done, when they were deflated. The bladder flap was done by superficially incising and dissecting the peritoneal lining to separate the bladder from the lower uterine segment. The procedure was performed without complications and the patient evolved favorably, with normal hematimetric rates and without hemodynamic repercussions, being discharged 3 days after the delivery.
Placenta accreta spectrum is a life-threatening condition, especially when associated with placenta previa and prior cesarean delivery. It has been identified as a relevant contributor to maternal death from hemorrhage and seems to increase morbidity and mortality every year (11); (12). Antenatal diagnoses supported by ultrasound and MRI forwarded cases to early delivery planning, including the need of a multi-professional team, patients and family agreements, prompt surgical approach to delivery, site of hysterotomy and hysterectomy requirements (13).
Unless the placenta acretta is unexpectedly identified during a cesarean delivery, diagnosed cases must have their delivery planned. There is increasing evidence that the management of women with placenta accreta spectrum disorders by multidisciplinary teams in health centers of excellence decreases maternal morbidity and mortality when compared with standard obstetric care. Adequate multidisciplinary team management of PAS disorders can only be arranged when the diagnosis is made prenatally and the involvement of pelvic organs and tissues around the uterus has been accurately defined [14].
Planned cesarean hysterectomy performed before the labor to avoid emergency delivery has a potential to reduce maternal morbidity [11].
Preoperative urologic care with ureteric stent placement ‒ mainly when there is a parametrium involvement ‒, no attempts to remove the placenta before hysterectomy, endovascular balloons strategies, uterine artery embolization, and use of intraoperative ultrasound and cystoscopy must be discussed beforehand. As the placenta accretta spectrum has a wide variety of anatomical peculiarities, all the procedures listed above must be left in standby mode [5].
Evidence of worse outcomes in urgent delivery in placenta accreta spectrum reinforces the need of planned delivery using a multidisciplinary team due to increased rates of maternal coagulopathy and the need for more aggressive blood transfusion when the surgery is precipitated by vaginal bleeding as well as increased neonatal morbidity [15].
The relevance of this issue led medical teams to propose surgery steps in severe placenta acretta spectrum, called modified radical peripartum cesarean hysterectomy [16].
For stable (no bleeding or preterm labor) patients, we advise planned delivery between 34+0 and 35+6 weeks of gestation [1]. For women at high risk of emergency delivery before 34 weeks, planned delivery before 34 weeks may be reasonable, although outcomes are still favorable with emergency delivery in centers of excellence [15].
We performed the cesarean a little bit late at 36 weeks because the diagnosis was made at 32 weeks and we tried to make all the arrangements for the procedure in 4 weeks.
The choice of skin incision is left to the operator’s judgment, although many employs vertical incisions for better access and visualization. Reasonable alternatives are wide transverse incisions such as a Maylard or Cherney incisions [1].
We used a wide Pffannenstiel incision, and we did not have any problem to gently pull out the uterus. Obesity, previous abdominal incision, and surgeon expertise must be considered while performing the skin incision and change it if necessary.
A maneuver to pull out the uterus was performed to have uterine extra-abdominal exposure, and a fundus cesarean section was carried out. We used a transversal incision of the uterine fundus as described [17]. There was minimal bleeding observed from the surgical wound in the uterine fundus.
The hysterotomy in a position far enough away from the placenta site (fundus, posterior or anterior) is the main purpose of this report, and it may be performed with the help of imaging exams or visual intraoperative inspection.
The diagnoses of anterior placenta acretta spectrum was made by ultrasound and MRI imaging exams and was confirmed by visual intraoperative inspection. A fundus hysterotomy was carried out and a breech delivery was performed, and placenta was left in situ to proceed the hysterectomy. Endovascular team allocated temporary balloons in internal iliac arteries to facilitate the hysterectomy. After evaluating the blood loss and intraoperative bleeding which was not excessively high, uterine artery embolization was not considered and cesarean hysterectomy was performed. The conservative management in order to preserve the uterus with the immediate or late placental removal must be discussed beforehand, depending on reproductive desire, comorbities, and all threatening risks.
Placenta acretta spectrum disorders are increasing all over the world, mainly due to the increased incidence of cesarean section procedures. Many strategies have been reported to decrease pregnant morbidity and mortality in these cases.
Our report describes anterior placenta acretta spectrum and may contribute in the surgical management of placenta accreta disorders to increase the effectiveness of cesarean hysterectomy.
In this sense uterine extra abdominal exposure in the management of placenta previa and accreta to proceed hysterotomy and its most appropriate site may prevent hemorrhage complications in placenta acretta disorders and uterine fibroid pregnancies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
