
Research Article | DOI: https://doi.org/10.31579/2641-0419/064
1* Internal Medicine New York, NY Physician
2 Cardiology New Brunswick, NJ Physician
3 Cardiology New York, NY Cardiac Electrophysiology Physician
4 General Cardiology, Cardiac Electrophysiology, Interventional Cardiology
5 Clinical Cardiac Electrophysiology Mount Sinai Health System New York, NY
6 Cardiac Electrophysiology
*Corresponding Author: Mohaned Egred, Cardiac Department, Freeman Hospital, Newcastle-upon-Tyne, UK.
Citation: Jackson M., Egred M.,(2020) Usefulness of the Turnpike Gold Catheter in Balloon Uncrossable Coronary Lesions. J Clinical Cardiology and Cardiovascular Interventions, 3(5);DOI:10.31579/2641-0419/064
Copyright: © 2020 Mohaned Egred, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2020 | Accepted: 16 April 2020 | Published: 23 April 2020
Keywords: percutaneous coronary intervention; stent, microcatheter; urnpike; corsair; LASER PCI; coronary artery disease; resistant stenosis; calcified coronary arteries; debulking techniques; atherectomy.
Balloon-uncrossable lesions present a particularly challenging situation to the interventional cardiologist. They are increasingly encountered with the more complex cases performed and the aging population undergoing coronary intervention.
Method
All procedures where a Turnpike Gold micro-catheter was used to cross a balloon-uncrossable lesion (defined as any lesion uncrossable by a balloon < 1.5mm in diameter or an alternative micro-catheter with adequate guide catheter and guidewire support) between September 2016 and September 2018 were included.
Clinical demographics, procedural details and peri-procedural complications were recorded.
Results
Twenty one cases were included. The average age was 77 +/- 9.6 years (61 – 93) and 13 (62 %) were male. Fourteen (67%) lesions were mildly to moderately calcified, six (32%) were severely tortuous and all coronary arteries were involved, LAD (8 cases), CX or OM (8 cases), RCA (5 cases).
The Turnpike Gold successfully crossed 14 (67%) lesions that other devices failed to cross (low profile balloons (7 cases), Corsair micro-catheter (9 cases), Turnpike Spiral (3 cases), CrossBoss (1 case). In three cases, multiple devices had failed to cross the lesion and a Guideliner extension catheter was used in 4 cases.
Conclusion
The Turnpike Gold can be safely and effectively used to cross lesions that low-profile balloons and other micro-catheters have failed to cross, and would help in achieving a successful procedural outcome.
Balloon-uncrossable lesions present a particularly challenging situation to the interventional cardiologist. Percutaneous Coronary Intervention (PCI) is increasingly undertaken in an aging population with complex coronary disease and heavy calcification.[1-3]
The inability to dilate or cross calcified lesions with a balloon remain a major limitation of PCI. Measures to overcome this limitation and cross these lesions are of paramount importance in clinical practice and debulking techniques can help overcome this limitation,[4] PCI in older patients with more complex coronary disease, heavily calcified lesions and tortuous arteries (both associated with adverse events during PCI) is becoming increasingly common[5-7]. Similarly, chronic total occlusions (CTO) are found in up to 20% of patients with coronary artery disease and account for 10 – 15% of all percutaneous coronary interventions[8-10]. The difficulty in their treatment is reflected in the lower success rate compared to other non-CTO lesions (70% vs 98%)[10-17] and balloon uncrossable lesions account for up to 9% of all chronic total occlusion (CTO) interventions[18]. After successful guidewire passage, it is the second commonest cause of procedural failure during CTO attempts[18,19].
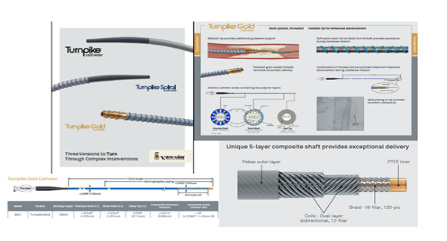
New techniques and instruments have been specifically developed to assist in complex PCI and this includes the Turnpike catheters of which there are 3 different ones (Vascular Solutions, Minneapolis, MN, USA) (Figure 1). The Turnpike is a family of micro-catheters that features a 5-layer composite shaft (Pebax ‘polymer’ outer layer, dual layer bidirectional coils for superior torque response and to permit tight bend radius without kinking, braid, PTFE Teflon inner liner) with a soft tapered
tip for enhanced flexibility and trackability and a hydrophilic coating over the distal 60cm for smooth advancement. The Spiral catheter adds a soft nylon outer coil over the distal 2cm of shaft to provide additional assistance during clockwise rotation allowing the device to track around tortuous anatomy. The Turnpike Gold adds a polished gold-coated threaded tip that increases the crossing profile of the catheter compared to the Spiral and LP but further enhances the ability to advance the catheter through balloon-uncrossable lesions[20].
We present our experience using the Turnpike Gold in balloon-uncrossable lesions to assess the feasibility and usefulness of this new device.
This is a retrospective analysis of prospectively collected data. The primary source of data was our local Coronary Artery Disease (CAD) database (Dendrite) which holds information on each PCI procedure performed at our hospital. Baseline demographics, clinical presentation, procedure details and procedural complications are prospectively collected at the end of every procedure by the performing cardiologist. Post procedural complications, clinical data and discharge medications are updated on discharge. Our hospital is a large tertiary centre in the North-East of England performing close to 3000 PCI in total and up to 200 CTO PCI per year.
Between September 2016 and September 2018, procedures where a Turnpike Gold micro-catheter was used were identified and included. All cases were performed by an experienced high-volume CHIP and CTO operator with more than 450 PCI/year.
A lesion was defined as ‘uncrossable’ if a low-profile balloon (less than 1.5mm in diameter) or an alternative micro-catheter other than a Turnpike
Gold (Corsair pro, Turnpike LP or Spiral etc) or device (e.g. over-the-wire balloon) would not cross it despite adequate passive guide support using a supportive guide catheter shape at least 6 French in calibre or a guide catheter extension.
Clinical demographics were recorded as defined in the British Cardiovascular Interventional Society (BCIS) standardised data set[21]. Calcification was defined according to the BCIS database. Mild (faint radiopacities noted during cardiac motion), moderate (dense radiopacities noted only during cardiac motion) or severe (dense radiopacities noted without cardiac motion before contrast injection generally compromising both sides of the arterial lumen). Severe vessel tortuosity was defined as one bend greater than 90 degrees or three bends 45 – 90 degrees proximal to the lesion.
The Turnpike Gold was deemed to have been used successfully if the lesion was crossed sufficiently to allow guidewire exchange and/or delivery of devices to facilitate a successful PCI (residual angiographic stenosis of < 30% and TIMI 3 flow). Any peri-procedural complications were recorded.
Once the lesion had been crossed using an 0.014” coronary guidewire and a balloon or other microcathetr failed to cross despite the use of a guidecatheter extension, the Turnpike Gold was used. It is advanced by using clockwise rotation to engage the lesion. Further procedural details (guide catheter and guidewire selection, arterial access etc) were done according to the operator normal practice and 60% of the cases were performed through the radial approach.
A total of 21 cases were identified, 5 of were CTO with TIMI 0 flow. The clinical demographics and procedural details of these cases can be seen in [tables 1 and 2] and sample cases are demonstrated in [figures 2 – 4].
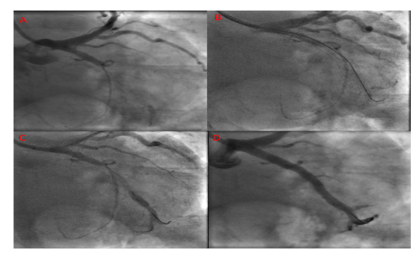
A 63y male with ongoing angina, ischaemia on stress imaging and a CTO of OM (A). The lesion was wired with a Confianza Pro 12 and Corsair (B) but the Corsair would not cross the lesion. A Turnpike Gold crossed restoring flow (C) and two drug-eluting stents were deployed (D).
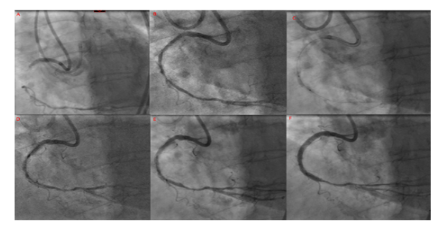
A 73y female with stable angina and CTO of RCA, shown here following both retrograde and antegrade contrast injections (A). The lesion was wired with a Confianza Pro 12 and Corsair (B) but Corsair would not cross the lesion. Turnpike Gold crossed successfully restoring flow (B). There was significant underexpansion of non-compliant balloons (C) and rotablation was performed with a 1.5mm and 1.75mm burr (D, E). Following extensive predilatation with non-compliant balloons, two drug-eluting stents were deployed successfully (F).
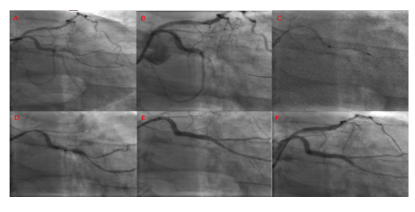
A 65y male with stable angina following previous primary PCI to RCA with severe 1,1,1 bifurcation lesion in CX (A). The lesion was crossed with a Sion blue wire (B) to OM1 losing flow. OM2 could not be wired despite multiple wires. A 1.2mm balloon and Corsair would not pass despite use of a Guideliner. A Turnpike Gold successfully crossed (C) restoring flow. Despite predilatation with a 2.5mm NC balloon (D), OM2 could not be wired and two drug-eluting stents with deployed (E). Final appearance following subsequent PCI to proximal LAD with a single drug-eluting stent (F)
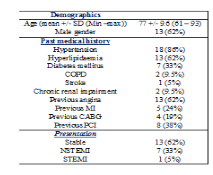

The average age was 77 +/- 9.6 years (61 – 93) and 13 (62%) were male. Thirteen (62%) lesions were at least moderately calcified, six (28.5%) were severely tortuous and all coronary arteries were involved (LAD (8 cases), CX or OM (8 cases), RCA (5 cases)). Thirteen (62%) cases were performed for stable coronary artery disease, seven (33%) patients were urgent cases following non-ST elevation myocardial infarctions and one (5%) case was a primary angioplasty procedure for ST-elevation myocardial infarction.
The Turnpike Gold successfully crossed 14 (67%) lesions that other devices failed to cross (low profile balloons (11 cases), Corsair micro-catheter (14 cases), Turnpike Spiral (3 cases), CrossBoss (1 case)). In 4 cases, multiple devices had failed to cross the lesion prior to using the Turnpike. In 4 cases, the Turnpike Gold crossed the lesion with additional support from a Guideliner catheter extension; in these cases, the Guideliner had been used to provide extra support for balloons (2 cases) and a Corsair micro-catheter (2 cases) which had failed to cross the lesion.
The Turnpike Gold failed to cross the lesion in 7 (33%) cases; in all of which other micro-catheters had also failed to cross the lesion prior to the Turnpike Gold (Corsair (7 cases), Turnpike LP and Spiral (2 cases)). Successful PCI was achieved in 5 of these cases, 2 using Excimer Laser Coronary Atherectomy (ELCA) and 1 using both ELCA and rotablation in the same setting. The remaining 4 failed cases returned at a later stage for repeat PCI using ELCA with successful outcome.
There were no immediate or direct complications from the use of the Turnpike Gold micro-catheter. However, two of the three cases that required ELCA to cross the lesions following failure to cross with the Turnpike Gold resulted in a complication. One patient who was a very high risk and elderly and was treated with ELCA and rotablation, died 3 days later after a cardiac arrest. Another patient had a minor coronary perforation after ELCA and ballooning and this was sealed with balloon tamponade only.
Resistant and complex lesions are encountered more frequently in the day to day practice. Crossing a resistant, occluded or fibro-calcific, lesion requires both the correct devices and the optimal support. This is more relevant in CTO PCI particularly with the increase undertaking of these complex cases. Despite advances in techniques and equipment, the success rate of CTO recanalization in the published literature ranges from 50 – 90% depending on the experience of the operator and lesion complexity[7-14]. The most common cause of failure is the inability to cross the occluded segment with a coronary guidewire (80-90%). However, failure to cross the lesion with a balloon or the inability to dilate the lesion account for 9% of failure [18].
Steps to overcome these resistant lesions are many. Upgrading the guide catheter to 7 or 8Fr, using a long arterial sheath and selecting a guide catheter shape to provide passive support through coaxial alignment with the coronary ostium and additional support from the opposite wall of the aorta (e.g. Extra Back Up (EBU) (Medtronic) / XB (Medtronic) for left coronary arteries, Amplatz Left (AL) (Medtronic) for right coronary arteries) are all simple strategies that can increase the chance of crossing a lesion[22]. In addition, the use of guide catheter extension is also an effective way in these cases. In our series and in nineteen cases (95%) a supportive guide catheter shape was used and in all but one case with ostial lesion. A 7F (11 cases) or larger calibre guide 8 Fr was used in 5 cases (24%). A Guideliner guide catheter extension (Vascular Solutions Inc., Minneapolis, MN, USA) to provide additional active support was used in 5 (24%) cases. Furthermore, the use a stiff tip CTO angioplasty wires, 13 (62%) cases, is an indication of the difficult and resistant nature of these lesions and cases.
A wide variety of micro-catheters is currently available, including the Tornus metal exchange penetration catheter (Asahi Intecc, Tokyo, Japan), Corsair and Caravel hybrid micro-catheter / septal dilators (Asahi Intecc) and FineCross micro-catheter (Terumo Medical Corporation, Somerset, NJ, USA). The Turnpike series of micro-catheters (Turnpike, Turnpike Spiral, Turnpike LP, Turnpike Gold), figure 4, all offer different solutions to the difficult-to-cross lesion (low crossing profile (LP), soft nylon coil on distal 2cm of shaft to aid advancement with clockwise rotation (Spiral), additional polished threaded gold tip to facilitate atraumatic delivery and enhance crossability (Gold).
In our series, the Turnpike Gold was successful in 67% of cases after low-profile balloons or other micro-catheters including other versions of the Turnpike device failed to cross the lesion. The Turnpike Gold has several advantages over other micro-catheters in this situation. The polished gold-coated threaded tip provides extra support and enhances the ability to advance the micro-catheter through the resistant segment and to engage in the lesion. The Turnpike series also have the largest proximal shaft diameter increasing the pushability over other micro-catheters.
One potential disadvantage is the larger crossing profile created by the threaded tip, however this is usually overcome with the threaded screw like tip that allow engagement and accessing the lesion. Lower profile micro-catheters such as the Corsair may be more successful at crossing some lesions and can also be utilised in the retrograde approach to ‘surf’ collaterals. However, it is possible that, even if the Turnpike Gold catheter does not completely cross the lesion, the ability to penetrate the proximal cap with the threaded tip may modify the lesion sufficiently to allow the balloon to cross or to engage enough to perform balloon-assisted microdissection to facilitate lesion modification and the successful completion of the procedure.
This is the first case series detailing experience with the Turnpike Gold and demonstrates that it is a useful tool in the management of the balloon-uncrossable lesion when other techniques have failed. Karacsonyi et al report the highest technical and procedural success rates were in patients managed with balloon-assisted microdissection and ELCA[18]. However, whilst the Turnpike Gold is more expensive than other micro-catheters, it remains cheaper than ELCA and may reduce the cost of the procedure by successfully crossing lesions that otherwise would have required ELCA not to mention the prolonged procedure time and use of multiple other equipment.
The large crossing profile may modify the proximal cap sufficiently to facilitate other adjunctive techniques such as balloon-assisted micro-dissection or ELCA or allow the exchange to a rotablation wire for debulking of the lesion. It is also common to offer a second attempt to revascularize CTO lesions when the first attempt has been unsuccessful; the use of the Turnpike Gold in difficult to cross lesions may help avoid repeat procedures, reducing contrast administration, radiation dosage and cost.
In cases where Turnpike Gold does not cross, ELCA, if available, can be used and requires no special action as it is compatible with and workhorse 0.014” PCI wires. On the contrary, rotablation to be used, requires a special thin 0.009” wire that is difficult to deliver unless an over the wire catheter is delivered distally which may prove difficult in such lesions we described.
Our experience suggests that using the Turnpike Gold is safe and effective with no immediate or direct complications resulting from its use. Rates of coronary perforation with ELCA have been reported up to 2%[22,23] and it is not widely available in all catheterisation laboratories, it may be that the Turnpike Gold provides a safer initial alternative although larger studies comparing the two would be needed to determine this.
This is the first published case series detailing experience with the Turnpike Gold micro-catheter in patients with balloon-uncrossable lesions. However, it is an observational retrospective descriptive study with all inherent limitations and it is a small series of patients in a single centre and single (albeit high volume) CHIP and CTO operator, and it may be difficult to generalise the results. It does however show that it is a useful tool in our armamentarium to help deliver a successful procedural outcome.
Limitations of the study:
This is a retrospective study with all well documented and inherent limitations. In addition, it is a single centre, single operator experience. However, the use and experience of Turnpike Gold is limited and no literature is available to guide its use and this study despite these limitations would highlight and present the experience with its use and its outcome. This comes from a high volume centre and a high volume operator of complex and CTO PCI, third highest in the UK, and it can be used to inform the community of this device that can help improve PCI procedural outcome in resistant uncrossable lesions.
The Turnpike Gold can be safely and effectively used to cross lesions that are resistant to even small and low-profile balloons and or other micro-catheters. It offers a reasonable success rate with no evident immediate complications. It can be used prior to or in combination with more advanced techniques such as ELCA.
Conflict of interest:
The authors have no conflict of interest to declare.
No funding was used for this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
