
Review Article | DOI: https://doi.org/10.31579/2641-0419/254
1 BSc, PhD, Specialized professional Public Health Research Division National Institute of Health Avenue Street 26 No 51-20 CAN Bogotá, D.C., Colombia.
*Corresponding Author: María Luz Gunturiz A, BSc, PhD, Specialized professional Public Health Research Division National Institute of Health Avenue Street 26 No 51-20 CAN Bogotá, D.C., Colombia.
Citation: María Luz Gunturiz A (2022). Use of Potential Markers in the Management of Myocardial Damage and COVID-19. J. Clinical Cardiology and Cardiovascular Interventions, 5(3); Doi:10.31579/2641-0419/254
Copyright: © 2022 María Luz Gunturiz A, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 February 2022 | Accepted: 17 March 2022 | Published: 28 March 2022
Keywords: coronavirus; myocardial injuy; cardiovascular disease; biomarkers; covid-19
Several biomarkers such as cardiac troponin (cTn), D-Dimer, C-reactive protein (CRP) or lactate dehydrogenase (LDH) have been related to the severity and progression of COVID-19. However, the determination of which of these biomarkers can provide greater prognostic value will depend on the clinical background of each patient, comorbidities, among others.
Understanding the pathophysiological processes associated with cardiovascular damage and the metabolic processes associated with the critical course of the infection allows us to infer the prognostic and predictive value of the different biomarkers used both for COVID-19 and at the cardiac level.
It is well described that most of them are not only predictive of the severity of the disease, but are also useful for the clinical management of these pathologies, allowing in turn the stratification of positive COVID-19 patients in risk categories.
The objective of this review is to understand the role of known biomarkers for COVID-19 infection, and those used to predict cardiovascular diseases in these times of pandemic.
Coronaviruses affect the cardiovascular system and the complication and mortality rates of COVID-19 have been shown to be higher in patients with pre-existing cardiovascular risk factors or cardiovascular disease [1-3].
Previous studies have shown that myocardial injury and cardiovascular risk factors are associated with a worse prognosis in patients with COVID-19 in 2 Chinese cohorts, therefore, it has been suggested that the virus can cause heart damage, but the data on this topic is scarce and the clinical and prognostic consequences are still not fully clarified [4,5].
The pathophysiology of myocardial injury caused by SARS-CoV-2 is still under study, although some hypotheses and mechanisms of action have been described. The first is related to direct myocardial injury, where viral RNA was found in heart muscle cells in 35% of SARS-infected subjects in 2005 [6-8]. During these pandemic months, it has been suggested that SARS-CoV-2 can enter myocardial cells by binding to type 2 angiotensin converting enzyme (ACE) receptors on their surface [9-12].
Among the pathogenic mechanisms triggered by COVID-19 are inflammatory cascades, cytokine storms and activation of signaling pathways involved in coagulation, which are common in systemic vasculitis and lead to serious and even fatal complications, such as sepsis, disseminated intravascular coagulation and acute cardiovascular events [13].
Patients affected by COVID-19 produce cytokines that enter the systemic circulation, stimulating macrophages within the plaque to increase local cytokine production and cause an increase in tissue factor expression that makes lesions more thrombogenic [14]. If COVID-19 patients also have severe underlying atherosclerotic diseases, extreme cases of acute myocardial infarction are likely to occur during the course of the disease. COVID-19 patients are likely to suffer from atherosclerosis, leading to insufficient coronary blood supply and causing damage to the myocardium [15,16].
Constant increase in cardiac markers is a predictor of disease worsening and in most cases patients should be transferred to an intensive care unit (ICU) ward for treatment. Although the evidence that patients with hypertension and cardiovascular diseases are more susceptible to SARS-CoV-2 infection is still insufficient, the truth is that patients with hypertension and cardiovascular diseases are more likely to develop severe cases, in addition to the fact that patients with SARS-CoV-2 are more prone to cardiovascular complications [17-19].
Some publications have shown that myocardial damage in patients with COVID-19 is more frequent among patients with more serious disease and who entered ICU. It is worth mentioning that the increase in markers of myocardial damage in these patients regardless of pre-existing diseases could be related to increase myocardial oxygen demand in COVID-19 positive patients with or without known coronary artery disease [20-23]. For another way, SARS-CoV-2 infection, could lead to a significant increase in coronary flow and oxygen demand, causing myocardial ischemia, especially in patients with coronary disease.
The increase in myocardial metabolic activity causes a great expenditure of oxygen in the arterial blood, requiring the generation of flow increases from regulation mechanisms, capable of guaranteeing a balance between supply and demand, involving nervous, humoral, mechanical phenomena and electrical. Tachycardia and severe hypertension contribute to breaking this balance, causing damage to myocardial cells [23].
Definition of myocardial injury
Damage caused to cardiac cells by SARS-CoV-2 infection is relatively common in severe forms of the disease, however, the mechanisms by which these cardiac cell alterations occur are still under study, although whether knows that an imbalance occurs between oxygen supply and demand, systemic inflammatory response, hypoxia, microvascular dysfunction and direct myocardial damage caused by the virus. What is clear is that there is a relationship between myocardial damage and the future evolution of the patient and short-term mortality. For example, in a study that included 416 positive patients for COVID-19, elevated troponin I values above the reference value were found in those patients with an average age of 64 years (19.7%) [24].
Myocardial injury or damage is defined as the detection of a cardiac troponin value (T or I) above the 99th percentile of the upper reference limit, which can respond to acute or chronic damage depending on the values of the enzyme curve. Markers such as creatine kinase MB fraction (CK-MB) could be used in the detection of cardiac cell damage, although their sensitivity and specificity is lower than that of troponins [25,26].
On the other hand, higher in-hospital mortality has been reported in patients with myocardial damage. Guo et al [27] described that in 187 admitted patients, positive for SARS-CoV-2, 27.8% presented elevated troponin T values and mortality 52%, compared to 8.9% of those with enzyme values within the normal range.
In patients with myocardial injury with elevated levels of cardiac enzymes, electrocardiographic alterations of the ST segment and the T wave, regional motility disorders of the left ventricular walls and cardiac function, identified during the echocardiogram, also generally occur [24].
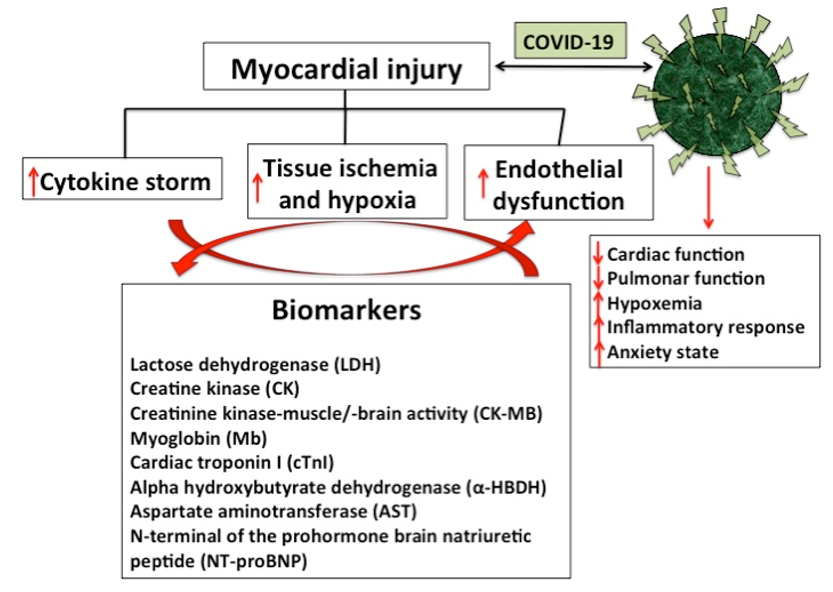
A study have shown that there is damage between 8% and 20% of cardiac cells associated with SARS-CoV-2 infection [28], especially when the disease occurs in its severe forms. Additionally, it has been described that in Chinese patients from the province of Wuhan, with an average age of 64 years positive for COVID-19, about 20% presented troponin I values above the reference value [24]. Although much progress has been made in the understanding of and the relationship between cardiovascular disease and COVID-19, the mechanisms by which alterations occur in the cardiac cell are not entirely clear. Among the factors involved in cardiac injury caused by COVID-19, the imbalance between oxygen supply and demand, systemic inflammatory response, hypoxia, microvascular dysfunction and direct myocardial damage caused by the virus, among others, could be considered [29]. (Figure 1).
However, many authors agree on the relationship between myocardial damage, patient evolution, and short-term mortality. It has been reported that patients with myocardial damage presented a quantitatively higher hospital mortality than those without this condition. Similarly, Guo et al [27], reported that mortality was greater than 50% in admitted patients, positive for SARS-CoV-2, with elevated troponin T values compared to patients who presented enzyme values within the normal range [23, 24].
It should be remembered that myocardial injury or damage is defined as the detection of a cardiac troponin value (T or I) above the 99th percentile of the upper reference limit, which can respond to acute or chronic damage depending on the values of the enzymatic curve. Biomarkers such as CK-MB could also be used in the detection of cardiac cell damage, although with lower sensitivity and specificity [25,26].
On the other hand, patients with myocardial injury, in addition to presenting high levels of cardiac enzymes, have electrocardiographic abnormalities of the ST segment and the T wave, as well as regional motility disorders of the left ventricular walls and cardiac function, identified by echocardiogram. Knowing how much enzyme elevation corresponds to primary damage to cardiac cells, and how much is secondary to critical states of the disease, is the challenge that clinical cardiologists are facing in these times of pandemic [23,24].
It is important to note that due to the difficulty in performing cardiac magnetic resonance imaging or endomyocardial biopsy, the diagnosis for cardiac affectation is based mainly on the elevation of troponin in association with echocardiographic data compatible with acute myocarditis (i.e., segmental wall motion abnormalities, left ventricular ejection fraction (ðLVEFÞ) < 50> 10mm and/or pericardial effusion) and ECG changes (ST elevation or ST/T segment changes) [13, 30,31].
Several authors have reported that high plasma levels of hyperhomocysteinemia (Hcy) significantly increase the incidence of vascular damage and that concentrations above the 90th percentile are associated with an increased risk of degenerative and atherosclerotic processes in the coronary, cerebral, and peripheral circulatory systems [32-34].
Hyperhomocysteinemia is defined as a medical condition characterized by an abnormally high level (>15 μmol/L) of Hcy in the blood [35,36]. The total Hcy concentration in plasma of healthy humans is low, between 5.0 and 15.0 μmol/L when assessed with the use of high performance liquid chromatography (HPLC), or 5.0–12.0 lmol/L when using immunoassay methods [37]. When the level is between 16 and 30 μmol/L it is classified as moderate, 31-100 μmol/L is considered intermediate, and a value >100 μmol/L is classified as severe hyperhomocysteinemia [38,39]. Recent publications have linked hyperhomocysteinemia with cardiovascular diseases, diabetes, CKD, and fatty liver disease [35,36,39]. Although Hcy is an effective biomarker of cardiovascular risk and it is known that cardiovascular complications are critical in hospitalized patients with COVID-19, this biomarker has not been used or studied in the clinical setting or in published prospective studies focused on useful laboratory markers for clinical evaluation of COVID-19 [13].
In line with the Fourth Universal Definition of Myocardial Infarction (2018), cardiac injury was diagnosed if serum levels of cardiac biomarkers (eg,hs-cTnT) were above the 99th percentile upper reference limit, (>14.0ng/L), as recommended by the manufacturer [26,40] and regardless of new abnormalities on electrocardiography and echocardiography. Among the cardiac markers, lactose dehydrogenase (LDH), creatine kinase (CK), creatinine kinase-muscle / brain activity (CK-MB), myoglobin (Mb), cardiac troponin I (cTnI), alpha hydroxybutyrate dehydrogenase (α- HBDH), aspartate aminotransferase (AST) and N-terminal prohormonal brain natriuretic peptide (NT-proBNP) increase their levels in different proportions in patients with COVID-19. Although LDH, CK, α-HBDH, and AST are cardiac enzymes, their increases cannot specifically represent myocardial injury, due in part to damage to the lungs, liver, kidneys, or other organs [30, 41-44].
On the other hand, it has been described that the anti-aging gene Sirtuin 1 has been linked to the risk for cardiovascular disease as well as various chronic diseases such as obesity, NAFLD, diabetes and neurodegenerative diseases. COVID-19 has been strongly linked to Sirtuin 1 inactivation and cardiovascular disease. According to this, within the selection of markers for the diagnosis and treatment of cardiovascular disease may need to involve the plasma measurement of Sirtuin 1 in COVID-19 individuals [45-47].
However, specific myocardial markers including CK-MB, cTnI, Mb, and NT-proBNP are increased to varying degrees in COVID-19 patients, especially in ICU and critically ill patients [48,49].
It is important to note that COVID-19 increases the risk of cardiovascular events, such as acute myocardial infarction, myocarditis and arrhythmias. Cardiac injuries as a result of COVID-19 are associated with higher mortality. It is not yet known whether there will be a long-term elevated cardiovascular risk as a result of COVID-19. In this context, the WHO [48] indicates that in patients with severe COVID-19, laboratory tests usually show a decrease in the number of leukocytes, in particular lymphocytopenia, as well as an increase in the number of neutrophils, inflammatory markers, D-dimer and elevated blood urea and creatinine concentrations. Chest computed tomography usually shows ground-glass opacities, with or without consolidative lesions. They are also more likely to be bilateral, have a peripheral distribution, and involve the lower lobes [48].
In studies with confirmed COVID-19 patients, biomarkers of cardiac injury have been reported to rise above normal during hospitalization and rise sharply immediately before death. It has also been reported that increased troponin, CK-MB, NTproBNP can and be considered indicators of possible cardiac damage during SARS-CoV-2 infection [30,50]. (Table 1)
For NT-proBNP, positivity was considered if serum levels were above the limit for ruling out heart failure in the acute setting, which is <300>
Acute respiratory distress syndrome was diagnosed according to the Berlin criteria as acute-onset hypoxemia (ratio of arterial oxygen partial pressure to fractional inspired oxygen expressed as a Fraction <300>
For the rapid propagation of the COVID-19, it is relevant to have biomarkers available to the progression of this pathology that allow patient risks stratification and identify those patients who will suffer a rapid progression of serious complications and death. The knowledge of new biomarkers for the detection, clinical management and prevention of serious complications should be based on the understanding of the molecular and cellular mechanisms involved in viral pathogenesis [13].
Several studies report that within the main laboratory findings in survivors and non-surviving patients with severe or fatal COVID-19, significant increase in total bilirubin and CK, together with serum ferritin, leukocyte count and IL -6 in non-survivors compared to survivors [20,55,56]. In addition to the strong association between thromboembolism, Covid 19 and myocardial injury, the diagnosis of D-dimer and cardiac markers is crucial in the follow-up of patients with COVID-19. On the other hand, the markers of muscular and cardiac injury were high in patients with both severe and deadly Covid-19 [43,52,57,58]. Additionally, in mortal chaos were found significantly higher cardiac troponin levels probably due to viral myocarditis and cardiac injury due to the progression of the disease to multiple organic insufficiency, also characterized by the significant elevation of liver enzymes (Alanine aminotransferase (ALT) and aminotransferase aspartate (AST)) and with critical changes in the parameters of renal function (blood ureic nitrogen, creatinine) and coagulation markers [13, 59].
Troponin has been used to determine the extent of cardiac injury, but determination of the level NT-proBNP on admission of COVID-19 patients could also help to better stratify the risk of in-hospital mortality or MV [52, 60].
C-reactive protein (CRP) is produced by the liver and its level rises when there is inflammation. LDL cholesterol not only coats the walls of the arteries, but also damages them by causing inflammation that the body tries to cure by sending out a "response team" of proteins called "acute phase reactants" within which CRP is found. Some studies report that testing for CRP levels is a better indicator of cardiovascular disease (CVD) than testing for LDL. However, it is important to mention that a CRP test is not a test for heart disease but rather a test for inflammation in the body. A high level could also be a sign of cancer, infection, inflammatory bowel disease, lupus, rheumatoid arthritis, tuberculosis, or another disease [44,61].
a-Hydroxybutyrate dehydrogenase (HBDH) is an isoenzyme of lactate dehydrogenase (LDH). Heart muscles contain high concentrations of HBDH. The serum concentration of HBDH is elevated in myocardial damage [62,63].
Cardiac markers |
Reference value | Value in patients with pre-existing cardiovascular diseases |
Observations |
Lactose dehydrogenase (LDH) | 120–250 U/L | In Covid patients values of ≥334U/L were reported
| This marker was initially used to aid in the diagnosis and monitoring of acute coronary syndromes. However, as it is a non-specific marker of tissue injury, only of the heart, it is currently hardly measured, and has been replaced by much more specific markers of diseases of cardiovascular origin, such as troponins. This marker rises 12-18 hours after the onset of symptoms and usually normalizes in the first week [44,61]. |
Creatine kinase (CK) |
50–310 U/L | In patients with Covid who did not survive the infection, it was observed that among other markers, CK and CK-MB were greatly increased compared to the values found in patients under the same health conditions but who managed to overcome the disease. | -Poor cardiospecificity and sensitivity -Not very useful for predicting cardiovascular risk -Recommended only if measurement of CK-MB or troponin concentration is not available. However, until the availability of other markers, total CK has been the most widely used biological marker for the diagnosis of myocardial and musculoskeletal disorders. Currently, it still has a relevant role in the follow-up of myocardial infarction in its sub-acute phase [13,16, 30, 48-50] |
Creatinine kinase-muscle/-brain activity (CK-MB) | 0–5 ng/mL | - It is the best alternative if there is no availability to analyze troponins - Detects reinfarction early - Not specific to heart tissue [30, 48-50] | |
Myoglobin (Mb) | 25 a 72 ng/mL (1.28 a 3.67 nmol/L | Myoglobin is considered one of the biomarkers of cardiac damage that, in patients with this pathology, is significantly associated with increased mortality from COVID-19, in more than half of the affected patients. | - Appears very early, less than two hours after the heart attack - It is useful when the patient goes to the doctor as soon as he notices the symptoms - It has a high sensitivity - It is not specific to cardiac tissue, but it is useful to rule out a heart attack [48,49]. |
Cardiac troponin I (cTnI)
| >14 ng/L 0.04 ng/mL | In patients with mycarditis, values of 0.12 ng/mL were reported In patients with Covid-19, the recorded cut-off points associated with a worse prognosis are >25,6 pg/mL(hs-TnI) and ≥21ng/L | - It is the most suitable for detecting acute myocardial infarction. - Detects minimal myocardial damage - Of high clinical value for the choice of treatment - Higher sensitivity and specificity than CK-MB - It is a marker of evolution [30, 48-50] |
C reactive protein (CRP) | hs-CRP level of lower than 1.0 mg/L -- low risk of CVD (heart disease)
hs-CRP level of 1.0 mg/L and 3.0 mg/L -- moderate risk of CVD
hs-CRP level of more than 3.0 mg/L -- high risk of CVD | In patients with Covid-19, the recorded cut-off points associated with a worse prognosis are ≥10mg/dL |
-It is a marker of evolution [44,61] |
D-Dimer | The reference value should be less than 100 ng/ml. Values greater than 500 ng/ml strongly suggest disseminated intravascular coagulation. (Quantitative methods). | The increase in D-dimer and lactate dehydrogenase (LDH) is considered a risk factor for the development of acute respiratory distress syndrome and its progression to death in patients with COVID-19. In China in a cohort of patients with cardiovascular diseases and Covid-19, values of D-dimer of ≥1112ng/mL were observed. | D-dimer is a fragment of fibrin that contains an intermolecular bond between the gamma chains of two fibrin monomers but not fibrinogen. It comes from the action of plasmin on stabilized insoluble fibrin. D-dimer has a negative predictive value of over 90%, meaning that a negative result excludes coagulation activation and consequently fibrinolysis [57] |
Hcy | Normal between 5.0 and 15.0 μmol/L when assessed with the use of high performance liquid chromatography (HPLC), or 5.0–12.0 lmol/L when using immunoassay methods | Above the 90th percentile are associated with an increased risk of degenerative and atherosclerotic processes in the coronary, cerebral, and peripheral circulatory systems. Abnormally high level (>15 μmol/L) of Hcy in the blood. Recent publications have linked hyperhomocysteinemia with cardiovascular diseases, diabetes, CKD, and fatty liver disease. | Although Hcy is an effective biomarker of cardiovascular risk and it is known that cardiovascular complications are critical in hospitalized patients with COVID-19, this biomarker has not been used or studied in the clinical setting or in published prospective studies focused on useful laboratory markers for clinical evaluation of COVID-19 [32-34, 38,39]. |
Aspartate aminotransferase (AST) | Ranges depend on multiple factors and vary slightly between different laboratories. The test report must include the reference ranges used in the laboratory that performed the analysis.
Men: 14 – 20 units perliter (U/L) Women: 10 – 36 U/L
| The amount of AST in the blood is directly proportional to the amount of tissue injured. AST elevation begins 6–10 hours after injury and remains elevated for about 4 days.
In patients with Covid-19 who also presented liver complications, the values observed in many cases doubled the reference values. | The activity of transaminases in the blood has traditionally been used as an indicator of liver injury, and since the heart and muscles produce a fairly high AST, it has also been used in the diagnosis and monitoring of myocardial infarction, although its role has been relegated to the background due to its low specificity and the existence of better markers. Because AST can be elevated for different reasons, in the event of altered values, it is usually necessary to carry out additional tests to correctly interpret the results [41-44] |
N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) | 300 pg/mL | Individuals with severe SARS-CoV-2 infection frequently have elevated levels of BNP and NT-proBNP27. In some patients with severe COVID-19 pneumonia, the prognostic value of NT-proBNP levels was greater than 88.6 pg/ml and was associated with a higher risk of in-hospital death; after adjusting for sex and age. Additionally, patients with elevated COVID-19 and NT-proBNP had high blood pressure and coronary heart disease more frequently. | - High diagnostic value - Helps to stratify risk - It is very useful to establish a treatment - It is a marker of evolution - Functionality of the left ventricle [13,16,50,52] |
Table 1: Cardiac marker and COVID-19
It is well described that inflammation plays an important role in the pathogenesis and prognosis of COVID-19, so many studies are focusing on studying the cytokine storm phenomenon and investigating effective, cost-effective and easily accessible inflammatory biomarkers [64, 65].
Patients with more severe presentations have been shown to trigger an acute systemic inflammatory response with fatal and fulminant hypercytokinemia; which is what has been called a “cytokine storm” [66,67].
Cytokine storm is a generalized inflammatory response characterized by an increase in circulating levels of pro-inflammatory cytokines: interferon gamma (γ), tumor necrosis factor alpha (TNFα), interleukins (IL-1β, IL-6, IL-12) and chemokines. In SARS, it is associated with pulmonary inflammation and extensive lung involvement very similar to that found in MESR-CoV38 infection. Additionally, they are also associated with myocardial damage and cardiac remodeling [68,69].
As already described, inflammation plays an important role in the pathogenesis of COVID-19, but it is also an important driver of pathological cardiac responses to stress, including after myocardial infarction and the transition to heart failure, where immune cells infiltrate the myocardium and release proinflammatory cytokines that regulate maladaptive cardiac remodeling [70,71].
TNFα is a cytokine secreted into cardiac tissue by macrophages, endothelial cells, and cardiomyocytes, and has an effect on reducing the contractile force of the myocardium, in addition to its role in calcium hemostasis, excitation-contraction junction, and oxide metabolism nitric and signaling through second messengers. It can also facilitate cell apoptosis, once chemical damage occurs, and contribute to cardiac dilation [72-78].
TNFα, IL-1β and IL-6 affect the myocardium, due to a decrease in blood pressure and peripheral resistance, while in the long term nitric oxide has a deleterious action on cardiac contractility. For their part, endotoxins and cytokines inhibit cytosolic calcium movement in isolated cardiac myocytes and open potassium-dependent ATP channels, shortening
action potentials and reducing intracellular calcium availability, which decreases calcium reserve and contraction [79-81].
In COVID-19, the inflammatory response caused by the infection has a depressant effect on contractile force, as well as a direct action on the vessels of the heart and arteriosclerotic disease. Increased inflammatory activity in the walls of coronary vessels and inside atherosclerotic plaques contributes to making unstable plaques more susceptible to rupture, increased blood procoagulant activity, contributing to the formation of Occlusive thrombi on a fractured coronary plaque [82-84].
In severe forms of COVID-19 infection, serum levels of inflammation mediators are increased, secondary to a dysfunctional and uncontrolled immune response, causing serious damage to cardiac function. Abnormalities in hematological, biochemical, inflammatory and immunological biomarkers have been observed in patients with COVID-19 and severe or mild systemic disease, which could be used to generate risk stratification models [13, 84].
Infection by COVID-19, in addition to the possible binding of the virus to an ACE2 receptor on myocardial cells, could favor the internalization and subsequent replication of the capsid proteins and the viral genome with a direct effect of the virus on the tissue myocardial. In this context, it is likely that the cytokine storm triggered by the COVID-19 infection is responsible for myocarditis, and in its most severe presentation with circulatory failure and high mortality [85,86].
Within hematologic biomarkers used to to classify COVID-19 patients include white blood cell, lymphocyte, and neutrophil counts, lymphocyte-to-neutrophil ratio (NLR), platelet count, eosinophil count, and hemoglobin. Lymphopenia, excessive activation of the inflammatory cascade, and cardiac involvement have been reported to be crucial features of COVID-19 disease and have high prognostic value, however, the understanding of the mechanisms involved is still under study. Based on results obtained from clinical practice, it has been proposed that coronaviruses can directly infect bone marrow precursors, generating abnormal hematopoiesis and triggering an autoimmune response against blood cells [13, 87-89].
In summary, SARS-CoV-2 damages myocardial cells and induces changes in cardiac laboratory markers to varying degrees through mechanisms that include, among others, direct infection of the myocardial lesion, specific binding to functional receptors on cardiomyocytes and immune-mediated myocardial injury. In this context, in patients with COVID-19, it is relevant to prevent myocardial injury to reduce the possibility of irreversible myocardial remodeling and the appearance of congestive heart failure [31].
During the pandemic, it has been shown that myocardial injury is a common finding in patients hospitalized for COVID-19. In this context, the selection and proper use of cardiovascular injury markers that allow risk stratification and anticipate the need for advanced treatments is relevant. In any case, it is worth mentioning that myocardial injury is also observed in critically ill patients in other circumstances and affected by inflammatory processes that ultimately lead to perfusion defects and myocardial injury. Therefore, the proper selection and incorporation of the different biomarkers can be useful in the diagnosis, early detection and prediction of cardiovascular diseases in times of COVID-19.
The author wishes to acknowledge the financial support provided by the National Institute of Health of Colombia.
Abbreviations
The following abbreviations are used in this manuscript
SARS | Severe Acute Respiratory Syndrome |
COVID-19 | New coronavirus of 2019 (Wuhan virus) |
ICU | Intensive care unit |
LDH | Lactose dehydrogenase |
CK | Creatine kinase |
CK-MB | Creatinine kinase-muscle/-brain activity |
Mb | Myoglobin |
cTnI | Cardiac troponin I |
CRP | C reactive-protein |
α-HBDH | Alpha hydroxybutyrate dehydrogenase |
AST | Aspartate aminotransferase |
NT-proBNP | N-terminal of the prohormone brain natriuretic peptide |
CVD | Cardiovascular disease |
IL | Interleukins |
WHO | World Health Organization |
ACE | Angiotensin converting enzyme |
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
