
Case report | DOI: https://doi.org/10.31579/2578-8868/342
1 Neurosurgeons. Institute of Neurology and Neurosurgery. Havana - Cuba.
2 Neurosurgery Resident. Institute of Neurology and Neurosurgery. Havana - Cuba.
*Corresponding Author: Duniel Abreu Casas, Neurosurgeons. Institute of Neurology and Neurosurgery. Havana - Cuba.
Citation: Duniel A. Casas, Jhohana L. Benavides, (2024), Use of Heber FERON as Part of the Treatment in Diffuse brain tumors: Report of Two Cases and Literature Review, J. Neuroscience and Neurological Surgery, 16(3); DOI:10.31579/2578-8868/342
Copyright: ©, 2024, Duniel Abreu Casas. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 08 October 2024 | Accepted: 23 October 2024 | Published: 29 October 2024
Keywords: glioblastoma, adult diffuse glioma, heberferon
Glioblastomas are the most common and malignant tumor among glial neoplasms (1). According to the Central Brain Tumor Registry of the United States (CBTRUS), the age-adjusted annual incidence rate of malignant primary brain tumors is 7.06/100,000 inhabitants and glioblastoma was 49.1% of them (2). It is characterized by being a fast-growing tumor, composed of a heterogeneous mixture of poorly differentiated astrocytic tumor cells, with pleomorphism, necrosis and vascular proliferation. According to the fifth classification of the World Health Organization, this type of tumor does not present a mutation in the IDH gene and usually presents a mutation in the EGFR gene, a mutation of the TERT promoter, trisomy of chromosome 7 and monosomy of chromosome 10 (3). It can manifest at any age, but it mainly affects adults, with a peak incidence between 45 and 70 years (3).The failure of current therapeutic approaches (focusing on surgical resection followed by radiotherapy and chemotherapy) is due to the dissemination that occurs in these tumors. Gliomas are highly infiltrating neoplasms, with solitary tumor cells or clusters of neoplastic cells that migrate extensively throughout the brain. In addition, malignant gliomas are an important stimulator of angiogenesis in a physiological manner, and angiogenesis in turn, may be a significant component in the progression of glial tumors. (5)This situation shows that the population of patients with malignant gliomas does not have therapeutic options to prolong their life, for this reason these two cases are presented to whom a therapeutic option with HeberFERON was offered to patients with diffuse brain tumors with a poor prognosis, also evaluating its antitumor effect (Imaging).
Glioblastomas are the most common and malignant tumor among glial neoplasms (1). According to the Central Brain Tumor Registry of the United States (CBTRUS), the age-adjusted annual incidence rate of malignant primary brain tumors is 7.06/100,000 inhabitants and glioblastoma was 49.1% of them (2). It is characterized by being a fast-growing tumor, composed of a heterogeneous mixture of poorly differentiated astrocytic tumor cells, with pleomorphism, necrosis and vascular proliferation. According to the fifth classification of the World Health Organization, this type of tumor does not present a mutation in the IDH gene and usually presents a mutation in the EGFR gene, a mutation of the TERT promoter, trisomy of chromosome 7 and monosomy of chromosome 10 (3). It can manifest at any age, but it mainly affects adults, with a peak incidence between 45 and 70 years (3).
In this type of neoplasia, different genes have been identified that are involved in the diagnosis, some of them in the prognosis and a few others with predictive power in the response. Among them, the Tyrosine Kinase receptors (RTQ) play a very important role, which are characterized by being central regulators of cell proliferation, differentiation and apoptosis pathways. The lack of regulation of the signaling mediated by these proteins is involved in the pathogenesis of multiple neoplasias such as glioblastomas (4).
A report of two cases and a review of the literature are presented, the objective of which is to present to the neurosurgical community the clinical characteristics and ominous prognosis despite the therapeutic measures that are currently owned.
Female patient, 24 years old, mixed race, dexterous, urban origin, with a history of migraine since adolescence treated with second-line analgesics, once hormonal causes were ruled out, MRI brain imaging studies were performed.
(October 2019) (Figure 1) where a neoplastic-looking mass is evident in the left parietal region, behaving as a well-defined, rounded, cortico-subcortical lesion, circumscribed to the primary sensory cortex in the postcentral g, yirus, which maintains homogeneous characteristics, with a hypointense character in T1, being hyperintense in T2 and FLAIR sequences, which does not capture contrast, which is bordered in its posterior and medial pole by a terminal branch of the M4 segment. middle cerebral artery, possibly the same post-central artery. The lesion has a diameter of 3.09 x 3.1 cm with very little perilesional edema, and no mass effect on adjacent structures is observed. The physical examination revealed that there were no signs that would suggest an injury in the affected area.
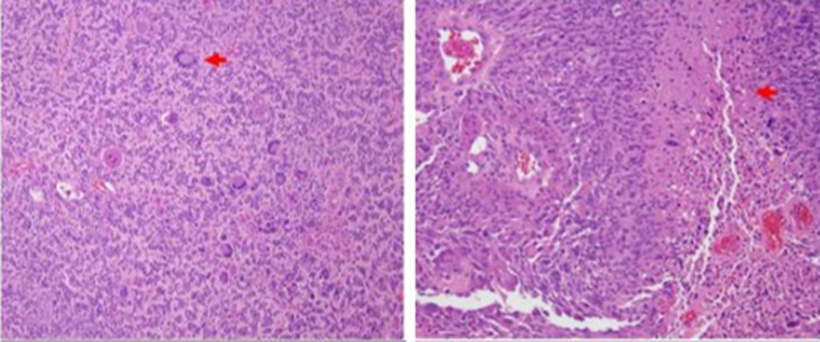
Figure 1:
On November 12, 2019, the Institute of Neurology and Neurosurgery for neurosurgical procedure (November 13, 2019) where it was performed
Left Temporo-Parietal Craniotomy, during the transoperative period a frozen biopsy was performed where slight nuclear pleomorphism in the brain white matter was observed, there was no mitoses or newly formed vessels, K167 with marked nuclei less than 1%, concluding a histopathological diagnosis of reactive gliosis secondary to a low-grade tumor.
A CT imaging study of the Post Cranial Nervous System is performed Operative (November 17, 2019) observing image of bone continuity solution in the left parietal region related to the craniotomy area performed during the surgery, noting little residual edema in the surgical bed, which is visualized as a hypodense image in the left parietal cortico-subcortical region. No hematomas are observed in the bed, and the presence of discrete bilateral frontal pneumocephalus is observed. Midline structures are intact, no displacement of the same, ventricular system and basal cisterns are present and functional.
The patient presented adequate clinical evolution, the wound showed no signs of local infection, and was discharged on November 13, 2019.
On November 17, 2019, the patient presented a seizure, with focal onset, which later became generalized, without loss of consciousness, which is why the anticonvulsant dose of Phenytoin was adjusted to 250 mg every 8 hours, anti- edema measures were started with 20% Mannitol IV for 5 days and Betamethasone (4 mg ampoule) every 8 hours, the patient responded to said treatment obtaining an adequate recovery.
During this hospital stay, a Simple Cranial CT scan was performed (November 22, 2019) were, due to the resolution of the post-surgical cerebral edema, a residual tumor lesion could be seen. However, it was decided to discharge the patient with clinical and imaging follow-up by the neurosurgery outpatient clinic, and the procedure was started to complete the treatment with Radiosurgery, which was arranged to be performed outside the country, but due to the epidemiological situation in the country and the world (Pandemic - COVID 19) this process was not possible to carry out.
In November 2021, the patient returned to our institution for consultation due to motor dysphasia, right hemiparesis, and recurrent headaches that did not respond to analgesic treatment.
A simple CT scan of the head was performed, which showed an increase in the size of the previously addressed tumor lesion accompanied by a cystic component, which compressed the ipsilateral ventricle and displaced midline structures. Given these imaging findings, it was decided to readmit on November 20, 2021, and the imaging study was expanded with contrast-enhanced brain MRI (November 23, 2021). Where a complex occupying lesion can be seen in the left frontoparietal region, its solid component occupies the periphery of the lesion, restricts diffusion, shows signs of angiogenesis and captures contrast.
The lesion measured 7.4 x 6.21 cm in axial section and is associated with a mass effect on neighboring structures. It is taken to the operating room with the objective of draining the cystic component of the lesion, which was carried out on November 26, 2021, where 60 ml of a yellow-greenish liquid with an oily consistency was extracted. With cytochemical: Color: Yellow, Appearance: Transparent, Pandi +++, Glycemia: 6.2 ml, Proteins: 2.08 ml.
A simple CT scan of the head was performed after the procedure (November 26, 2021), documenting the expected post-surgical changes in the recent left temporo-parietal region, signs of residual tumor lesion, and no hemorrhagic or acute ischemic signs.
After this procedure, the patient presented a favorable clinical evolution with evident improvement of dysphagia, adequate articulation of words, still maintained paresis of the right upper limb with a muscle strength of 3/5 distal and distal and was discharged from the hospital on November 29, 2021.
On December 17, 2021, the patient began with the same condition previously presented. A simple head CT scan was performed, which documented the presence of the cystic portion treated less than a month ago again. For this reason, she was admitted again.
Operated on December 20, 2021 Puncture of the cystic portion of the Right Parieto-Temporal lesion, evacuation and placement of intracystic Ommaya reservoir (45 ml of yellow pressurized fluid was drained).
The next day the patient is discharged.
On January 5, 2022, the patient was seen due to temperature increases of 38.5 °C. The reservoir was punctured, draining 28 ml and a medical discharge was decided. On January 8, 2022, the patient presented a focal onset seizure, which later became generalized. Convulsive management was adjusted. A simple head CT scan was performed (Figure 2) which documented an extensive, already known, occupying lesion with a drainage system in place, mass effect on the parenchyma and ventricular system.
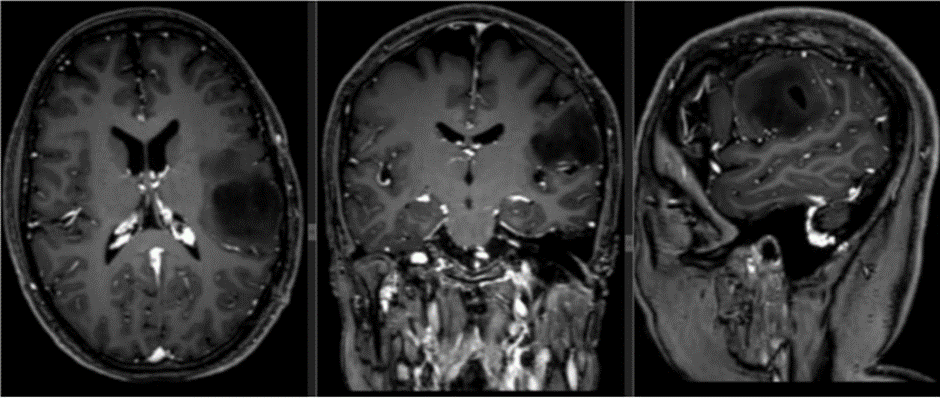
Figure 2
5 days later (January 10, 2022) he returned again, the reservoir was punctured but fluid extraction was not possible. Therefore, he was admitted for study.
A CEREBRAL MRI imaging study was performed (January 22, 2022) (Figure 3) surgical area occupied by a cystic portion of a dedifferentiated high- grade Astrocytoma tumor requiring puncture and evacuation of the cystic portion with a late control imaging study with tumor recurrence.
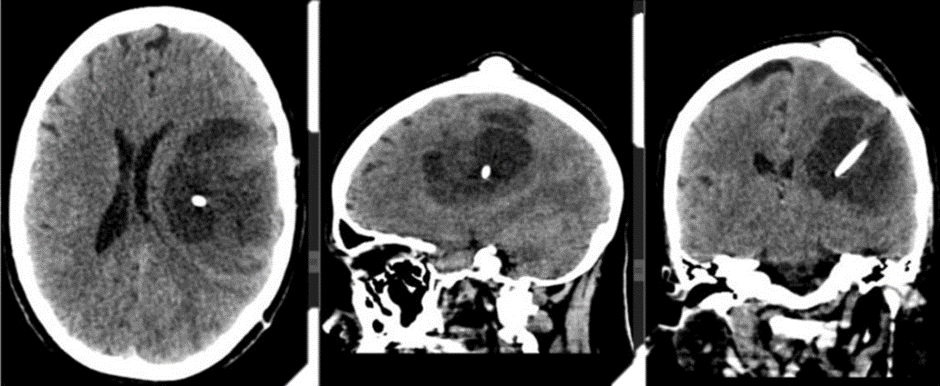
Figure 3
An electroencephalogram was performed (January 12, 2022) in which signs of intercritical focal cortical irritation of the left temporo-parietal regions of moderate intensity, signs of cortical dysfunction of the left cerebellar hemisphere of slight intensity were documented.
On January 18, 2022, the same previous surgery was performed at the left parieto-temporal level and the maximum safe macroscopic resection of the lesion was performed with a biopsy result (January 20, 2022): In the sample examined, hypercellularity and pleomorphism were observed.
cellular with the presence of tumor gemistocytic, small and other elongated cells. High number of atypical mitoses of endothelial hyperplasia with a glomeruloid appearance, microscopic areas of necrosis in palisade. Diagnosis: IDH MUTATED GLIOBLASTOMA. WHO GRADE IV.
The following day, January 20, 2022, a Simple Cranial CT scan (Figure 4) was performed for post-surgical control, observing recent post-surgical changes associated with a region of left cerebral hemispheric edema.
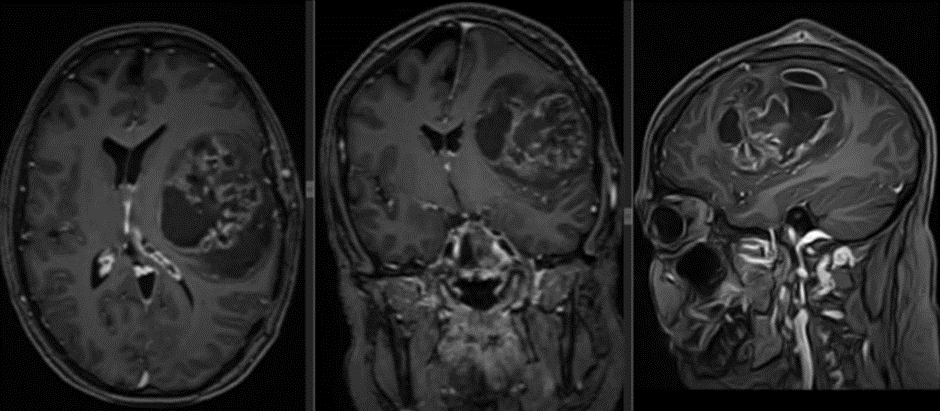
Figure 4
High-field imaging control was performed with Contrast-Enhanced Brain MRI (January 21, 2022) and a known heterogeneous left frontoparietal lesion was documented with significant mass effect on neighboring structures. After the administration of contrast, the lesion enhances in a non-homogeneous manner associated with enhancement of the ipsilateral ependyma as well as signs of diffusion restriction.
Patient with adequate clinical evolution, discharged on January 25, 2022 with referral by the Oncology service to start Radiation treatment completing 33 sessions of 1.8 GY which culminated on May 22, 2022 and Temozolamide concurrent with radiotherapy at a dose of 75 mg/m2 daily for 49 days and subsequently Adjuvant at a dose of 170 mg/m2 daily for 5 days every 28 days
On June 6, 2022, they consulted the institute of neurology and neurosurgery due to a clinical picture of one month of evolution, given by progressive decrease in muscle strength in the right side of the body, inability to express language, intermittent headache of mild to moderate intensity, occasional photophobia, reasons for which it was decided to admit them. A simple cranial CT study was performed (June 6, 2022) (Figure 5) observing post-surgical changes, an occupying lesion in the left fronto-parietal region measuring approximately 6.3 x 9.7 cm, heterogeneous with predominantly fluid (15 HU). This lesion exerts a mass effect on the ventricular system and neighboring parenchyma. IDX: Glioma.

Figure 5
Given these findings, it was decided to move the neurosurgical procedure to a new date (June 22, 2022), the injury from previous surgery was addressed, immediately documenting the leakage of cerebrospinal fluid upon opening the dura mater, and the remaining tumor was addressed in the BIOPSY result. (Figure 12)
Pleomorphic tumor cells, high mitotic index, areas of ischemic necrosis, and collagenized vessel walls are observed. Tumor cells are dispersed away from the tumor core. A diagnosis of IDH MUTATED GLIOBLASTOMA, RECURRENT, WHO GRADE 4 is concluded (IDH: Performed at the Hermanos Amejeiras Hospital)
Simple Cranial CT scan is taken (June 23, 2022) (Figure 6) Recent postoperative changes in the left frontotemporal region. No signs of hydrocephalus. No signs of ischemic injury or acute hemorrhage. The edema in the surgical bed is striking, with blood in its interior, which seems to extend to the inferior longitudinal sinus. The bone flap is dislocated.
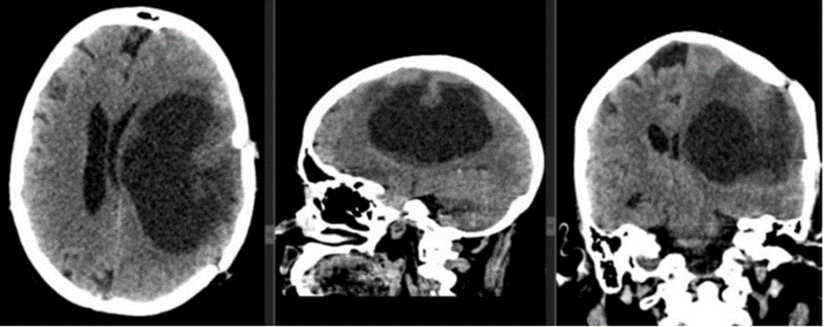
Figure 6
Simple Cranial CT (June 27, 2022) (Figure 7)

Figure 7
Postoperative changes in the left frontoparietal region are not recent, comparatively cerebral edema has increased in the left cerebral hemisphere and it is striking that the areas of bleeding in the surgical bed are larger. as well as herniation of the brain and an increase in the volume of the epicranial soft tissues. It is striking that the bone flap is more dislocated than in the previous study.
On July 14, 2022, the patient had a transcalvarian hernia confirmed by a Simple Cranial CT scan (Figure 8) accompanied by dehiscence of the surgical wound, for which she was taken to the operating room for repair, with respective imaging control (Figure 9). On August 22, 2022, an electroencephalogram was performed to adjust anticonvulsant treatment, a 19-channel EEG was performed, and the patient was in a functional state of wakefulness. Continuous baseline activity was observed, with preserved frequency and amplitude gradients. Globally, better modulated alpha activity of greater amplitude was recorded in the right hemisphere, alternating with diffuse global polymorphic theta activity, which was not blocked by eye opening.
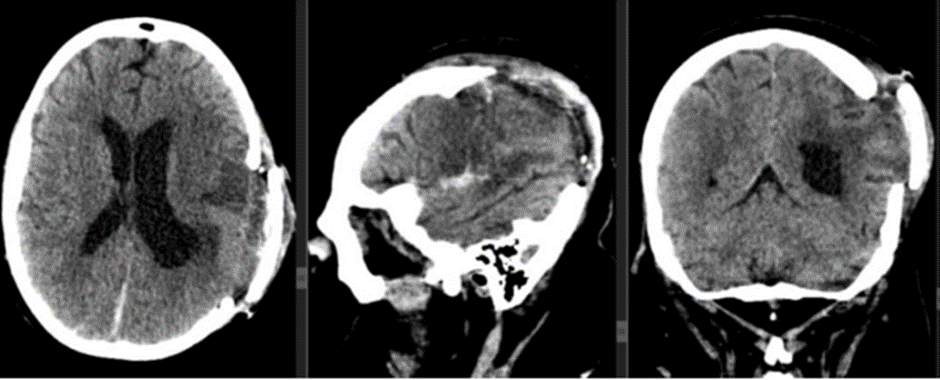
Figure 8

Figure 9
Focal interictal paroxysmal activity is recorded in the central-parietal region of the right hemisphere, of the type of slow angular waves that appear as very few isolated elements in the recording. Abnormal EEG. Signs of cortical irritation in the central-parietal region of the right hemisphere, of slight intensity
Patient is evolving satisfactorily with discharge hospitalized on September 20, 2022.
On October 4th, he starts with adjuvant treatment: RT + HeberFERON (currently 7.0 MUI: 2 bulbs - Tuesday and Friday) so far 2 years and 5 months have been completed (29 months). In February 2023, a Brain MRI is taken. (Figure 10) evolutionary where tumor control is observed.
The patient is currently at Miami Neuroscience Center at Larkin Community Hospital Inc. Dr. Aizik L. Wolf where imaging control was performed 19 months after starting Heberferon (Figure 11).
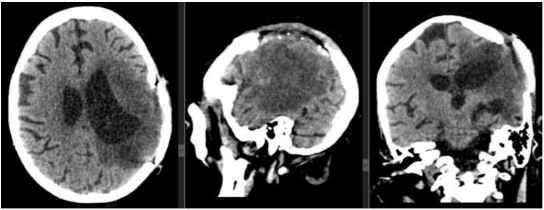
Figure 10
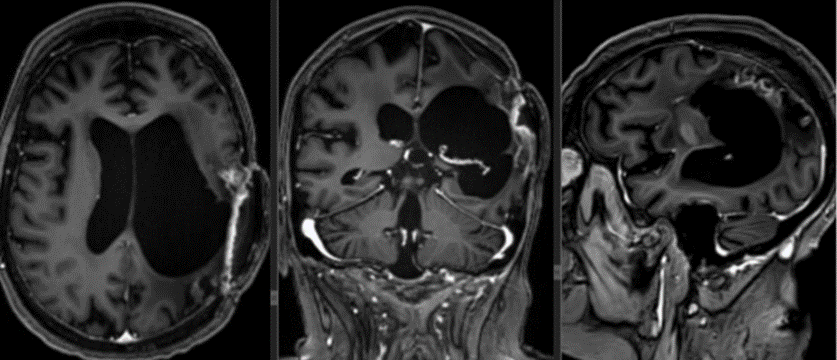
Figure 11
(Figure 12). Remarkable nuclear pleomorphism and giant cell characteristics along with pseudopalisade necrosis.
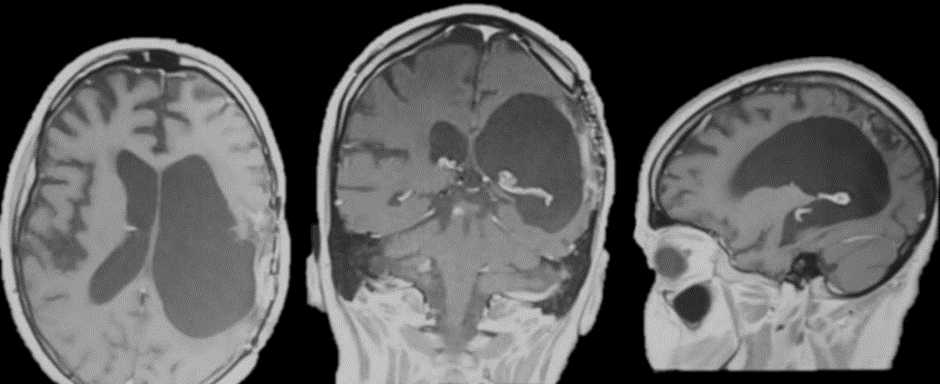
Figure 12
The second case is a 63-year-old male patient with a history of benign prostatic hyperplasia who underwent surgery in 2018. He debuted in January 2022 with associated gait instability, associated with intense, oppressive, holocranial headache, predominantly in the morning with little response to taking analgesics. No positive findings were found in the neurological physical examination.
In the emergency room, a simple head CT scan was performed, which showed mixed density images in the right fronto-parieto-temporal region, producing a mass effect on the ipsilateral lateral ventricle, as well as displacement of midline structures, surrounded by abundant perilesional edema.
An electroencephalogram was performed, which was reported as normal.
A brain MRI study shows a right sylvian occupying lesion surrounded by vasogenic edema with mass effect on neighboring structures with focal areas of diffusion restriction, signs of angiogenesis and calcification nuclei inside.
After administration of contrast, the walls enhance intensely, appearing irregular and thickened (Figure 13).
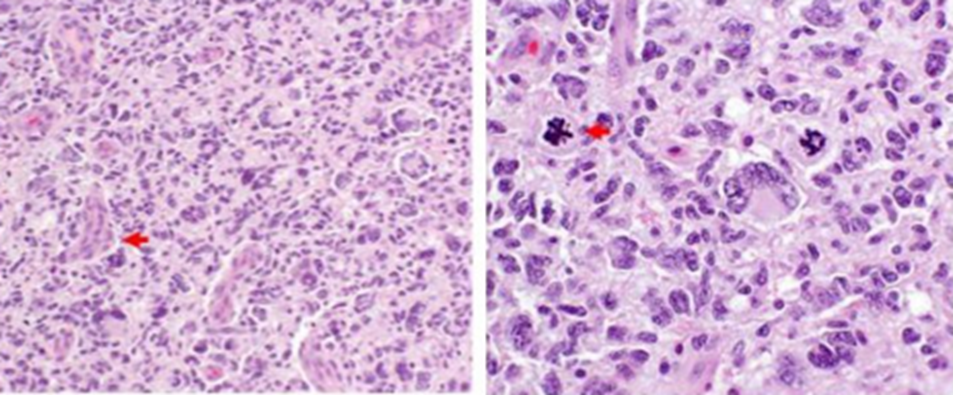
Figure 13
The spectroscopy sequence shows a high lipid peak. The lesion described measures 2.3 x 3 cm, which is related to Glioblastoma. Due to these findings, at the end of February 2022 he was taken to surgery where a right parieto-temporal craniotomy was performed with total fluoroguided tumor excision.
The biopsy study confirmed the diagnosis of Glioblastoma NOS Grade IV WHO, and the microscopic study of the sample showed fragments of cortex with the presence of red neurons and neuropil edema. Abundant areas of ischemic necrosis, vessels with thickened walls of glomeruloid appearance, newly formed vessels, a few small tumor cells with pyknocytic nuclei, and other large pleomorphic cells with atypical mitoses were observed. (Figure 14).
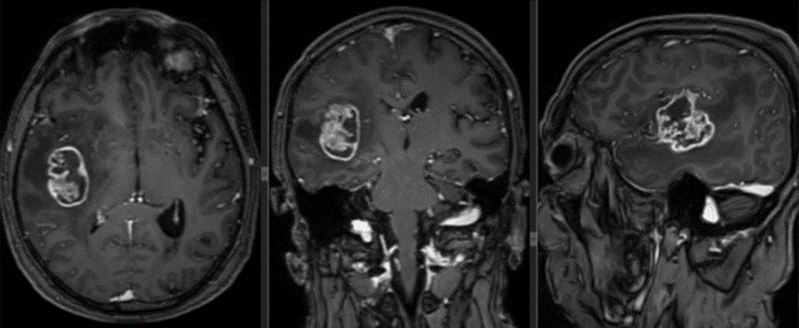
Figure 14
One week after surgery, he was discharged with adjuvant treatment: RT + Temozolamide alone as monotherapy (6 cycles) + HeberFERON. In February 2023, a progressive brain MRI was taken where tumor control was observed (Figure 15).

Figure 15
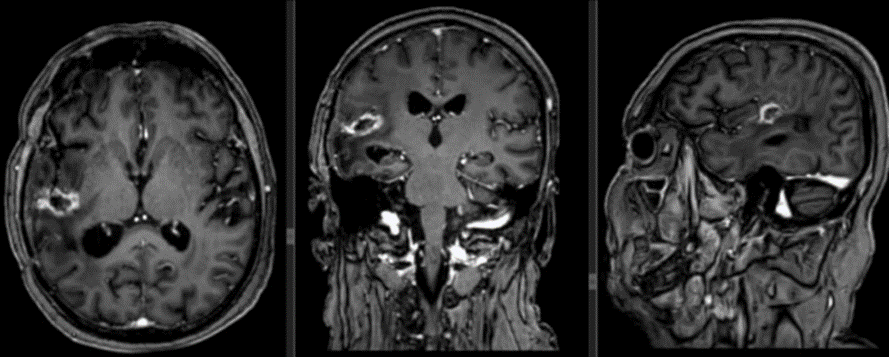
Figure 16
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
