
Case Report | DOI: https://doi.org/10.31579/2690-8794/092
*Corresponding Author: Sule Muhammad Baba, Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule M.B., Shamaki AMB, Umar A.U., Gele I.H., Dada M.A., Ribah M.M., Aliyu A.Z., (2021) Burkitt’s Lymphoma of the Right Jaw in a Child: The Radiographic Features and Case Report; J, Clinical Medical Reviews and Reports. 3(6); DOI: 10.31579/2690-8794/092
Copyright: © 2021, Sule Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 August 2021 | Accepted: 05 August 2021 | Published: 13 August 2021
Keywords: burkitt’s lymphoma, jaw swelling, dental anarchy, lamina dura
Burkitt’s lymphoma is a tumor that most often affects the jaws, most commonly seen in endemic areas of Africa, although the jaws are affected in about 15-18% in non-endemic regions, with prevalence in boys aged between 4-7 years.
This is a 12-year-old male child that presented with right jaw painful swelling for more than six-months duration of onset. He was referred for plain radiographs of the jaw from a peripheral healthcare center.
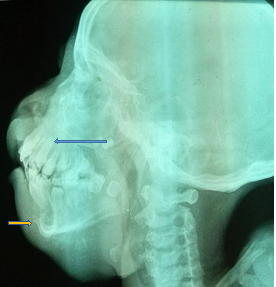
The jaw radiograph was done in anterior-posterior and oblique views of both sides respectively. The radiographs demonstrated a soft tissue density mass on the right, with associated destructive lytic lesion involving the right maxilla severelyand the right mandibleto a lesser extent. There is associated loss of lamina dura with severe dental anarchy involving the maxilla. The mandible showed lytic and expansile areas in its body with marked periosteal reaction; the sunray appearance. The contralateral maxilla and mandible have normal appearances. Complementary abdominal ultrasonography revealed normal appearances excluding abdominal involvement.
Histology revealed the classic diffuse starry-sky appearance with benign histiocytes containing abundant, clear cytoplasm dispersed among a background of homogeneous, basophilic tumor cells, in keeping with Burkitt’s lymphoma.
We report this case to describe the radiographic appearance of Burkitt’s lymphoma of the jaw bones.
Burkitt’s lymphoma (BL) is defined as a malignant lesion most predominantly affecting the jaw in about 50-70% of cases of children in Africa, and is of the B-lymphocyte origin, affecting the maxilla more commonly than the mandible [1, 2].
Burkitt’s lymphoma is a tumor that most often affects the jaws, most commonly seen in endemicareas of Africa,although the jaws are affected in about 15-18% in non-endemic regions [3].
BL is thought to be relatedpathogenetically to Epstein-Barr virus (EBV), more than 90% of tumor cells showed the EBV DNA in their nuclei most especially the African-BL, this was detected following insitu hybridization using EBV probes [1, 4, 5].
The World health Organization (WHO) classifies BL in three main variants, these are: endemic, sporadic and immunodeficiency-associated forms. The endemic form most often involves the jaw bones and the abdomen of equatorial African children, the sporadic form usually presents as an abdominal mass in adult patients from North America and Europe. The immunodeficiency-associated form has a similar presentation as that of sporadic form, with rare orofacial involvement [6, 7].
The main clinical featuresare those of facial swellingand pain, exophytic mass on alveolar ridge, discrete swelling with tooth mobility, alveolar bone destruction, loss of lamina dura, cutaneous ulceration and facial asymmetry [6].
Histological diagnosis of cases of BL revealed the classic diffuse starry- sky appearance, with associated diffuse proliferation of medium sized neoplastic lymphoid cells, with scant basophilic cytoplasm and few nucleoli [6].
Radiological examination of the jaw either by panoramic or plain radiographs of the jaw often reveals jaw swelling, radiolucent osteolytic lesion with destruction of the cortical bone, loss of lamina dura with dental anarchy [8].
Chemotherapy with combination of drugs; the R-CHOP, is the regimen of choice in the management of BL, these are Rituximab, Cyclophosphamide, Doxorubicin, Vincristine and Prednisolone, with satisfactory result especially in children [6, 9].
In BL, which is a malignant neoplasm, the combination chemotherapy proves effective in achieving a total cure with an overall survival rate of between 75-95%, although the tumor staging and onset of the chemotherapy also determines the achievable cure [1, 2].
This is a 12-year-old male child that presented with right jaw painful swelling for more than six-months duration of onset. He was referred for plain radiographs of the jaw from a peripheral healthcare center.
The patient is oriented, conscious and alert, has a jaw asymmetry with a hard mass in the region of the right upper and lower jaws with no ulcerations of the overlying skin.
The hemoglobin was normal, the white-cell countwas elevated and about 182x 109/L, there is also elevation of lactate dehydrogenase to about 7500 IU/L. The blood film revealed medium-large sized mononuclear cells with basophilic cytoplasm, vacuolation, and multiple nucleoli.
Histology revealed the classic diffuse starry-sky appearance with benign histiocytes containing abundant, clear cytoplasm dispersed among a background of homogeneous, basophilic tumor cells, in keeping with Burkitt’s lymphoma.
The jaw radiograph was done in anterior-posterior and oblique views of both sides respectively.
The radiographs demonstrated a soft tissuedensity mass on the right, with associated destructive lytic lesion involving the right maxillaseverely and the right mandible to a lesser extent (Figure1). There is associated loss of lamina dura with severe dental anarchy involving the maxilla (Figures1- 3). The mandible showed lytic and expansile areas in its body with marked periosteal reaction; the sunray or sunburst appearance (Figures 2 and 3). The contralateral left maxilla and mandible show normal appearances. Complementary abdominal ultrasonography revealed normal appearances excluding abdominal involvement.
A diagnosis of Burkitt’s lymphoma in a 12-year-old male child presenting with a right jaw mass was made. We report this case to describe the radiographic appearance of Burkitt’s lymphoma of the jaw bones.
The parents were counseled on the commencement of the combined chemotherapy; R-CHOP for about four-sixcauses, each courselasting for about 2 weeks. The patient is yet to commence the chemotherapy as at the time of this report.


Burkitt’s lymphoma, a malignant solid tumor of B lymphocytes grouped under the umbrella of non-Hodgkin's B-cell lymphoma. Burkitt's lymphoma is known to be endemic in Africa but can occur sporadically in other part of the world [10]. The index case is a confirmed case of Burkitt’s lymphoma and of the African ancestry residing in an African country, thereby conforming to this literature.
Burkitt's lymphoma is the most common childhood cancerin areas where malaria is holoendemic. The incidence is very high in immunosuppressed patients in non-endemic areas, especially when associated with HIV infection [11]. The index case happensto be a child aged 12-years, living in a malaria endemicarea, although not HIV positive,thereby conforming to this literature.
Burkitt’s lymphoma (BL) is also defined as a malignant lesion most predominantly affecting the jaw in about 50-70% of cases of children in Africa, and is of the B-lymphocyte origin, affecting the maxilla more commonly than the mandible [1, 2]. The case had affectation of both maxilla and mandible, with severe involvement of the maxilla, thereby agreeing to these literatures.
The World health Organization (WHO) classifies BL in three main variants, these are: endemic, sporadic and immunodeficiency-associated forms. The endemic form most often involves the jaw bones and the abdomen of equatorial African children, the sporadic form usually presents as an abdominal mass in adult patients from North America and Europe. The immunodeficiency-associated form has a similar presentation as that of sporadic form, with rare orofacial involvement [6, 7]. The case under review is most likely to be the endemic variant of BL; he has mainly the jaw lesion, no abdominal lesion and not a case of immunosuppression (HIV infection).
The main clinical featuresare those of facial swellingand pain, exophytic mass on alveolar ridge, discrete swelling with tooth mobility, alveolar bone destruction, loss of lamina dura, cutaneous ulceration and facial asymmetry [6]. The case under review also presented with most of these features, some of which are facial swelling and asymmetry, pain and dental anarchy to mention a few, thereby conforming to this literature.
Radiological examination of the jaw either by panoramic or plain radiographs of the jaw often reveals jaw swelling, radiolucent osteolytic lesion with destruction of the cortical bone, loss of lamina dura with dental anarchy [8]. The indexcase had plain radiographs of the jaw, these demonstrated destructive lesions of the maxilla with loss of lamina dura, dental anarchy with associated lyticlesions of the mandible and extensive sunburst or sunray pattern of periosteal reaction. These features are in conformity to those reported by this literature.
Histological diagnosis of cases of BL revealed the classic diffuse starry- sky appearance, with associated diffuse proliferation of medium sized neoplastic lymphoid cells, with scant basophilic cytoplasm and few
nucleoli [6]. The histologic findings of the case under review were also similar to the findings reported by this literature.
Chemotherapy with combination of drugs; the R-CHOP, is the regimen of choice in the management of BL, these are Rituximab, Cyclophosphamide, Doxorubicin, Vincristine and Prednisolone, with satisfactory result especially in children [6, 9]. The case under review was alsonot an exception, he was advised to commence the R-CHOP regimen; a course lasting for two weeks and expected to undergo four-six courses depending on the response clinically.
Jaw masses most especially in children living in endemic regions such as Africa, should be evaluated histologically, clinically and by radiologic means to rule out Burkitt’s lymphoma, this will enableprompt institution of management in-order to achieve a total cure, thereby reducing the associated morbidity and mortality associated with the condition.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
