
Research Article | DOI: https://doi.org/10.31579/2767-7370/070
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
2 Obstetrics Gynecological Nursing, Faculty of Nursing Benha University.
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Hanan E. Hassan, Samar S.A. Mohamed, Elham A. Ramadan, Amel A H. Omran (2023), Urinary Incontinence among Menopausal Northern Upper Egyptian Women Impact of Deep Kegel and Breathing Exercises. J New Medical Innovations and Research, 4(9); DOI:10.31579/2767-7370/070
Copyright: © 2023, Shahid Afridi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 November 2023 | Accepted: 27 November 2023 | Published: 06 December 2023
Keywords: deep breathing; menopausal women; kegel exercise; urinary incontinence
Background: According to age, the prevalence of stress incontinence ranges from 29% to 75%, with a mean of 48%.
Aim of the study: The study aimed to evaluate effect of deep breathing and kegel exercises on urinary incontinence among menopausal women.
Design: A quasi-experimental study design was utilized in this study (one group pre and post-test).
Sample: A purposive sample was selected and this study was performed on 100 Menopausal women diagnosed with stress urinary incontinence.
Setting: gynecological and urological outpatient clinics Beni-Suef university hospital.
Tools: Data was collected using 1) a structure interviewing questionnaire schedule, 2) The International Consultation on Incontinence Modular Questionnaire 3) Pelvic floor muscles exercises checklist.
Results: There were highly statistical significant differences in the frequency of urinary incontinence (p-value 0.000) and the amount of urine loss (p-value 0.004) among the studied women before and after practicing deep breathing and Kegel exercises, Also there were as highly statistical significant improvement in physical condition (p-value 0.000) and psychological condition of the studied women (p-value 0.000) after intervention than pre-intervention.
Conclusion: Deep breathing and kegel exercise had positive effect on physical and psychological conditions as well as “performing daily activities without stress, feeling of confidence and satisfied from sexual relation". Recommendations: Developing awareness program regarding importance and benefits of practicing deep breathing and kegel exercises to reduce stress urinary incontinence symptoms among elderly women.
Urge Urinary Incontinence is the involuntary leakage of urine accompanied by or immediately preceded by a strong sudden urge to urinate. Commonly referred to as “Overactive Bladder,” this incontinence is usually caused by involuntary contractions of the detrusor muscles of the bladder wall at inappropriate times. There is no gradual buildup of desire to urinate in this type of incontinence and a large amount of urine is lost during each incontinence episode [1].
According to age, the prevalence of stress incontinence ranges from 29% to 75%, with a mean of 48%. The prevalence of daily stress urinary incontinence is 10% in community dwelling middle-aged women; A third of women with stress urinary incontinence report leakage weekly. The overall prevalence of urgency urinary incontinence is estimated at 7-33%. 7 Women are more likely to experience urgency urinary incontinence (overactive bladder syndromewet) than men, with 9.3% of women experiencing this condition versus 2.6% of men. The prevalence of mixed urinary incontinence (both stress urinary incontinence and urgency urinary incontinence) ranges from 14% to 61% [2-4].
Continence aids and products: Counseling and guidance about the appropriate use of incontinence aids and pads are important for enhancing quality of life and reducing the stigma of incontinence. The range of products includes mobility aids, accessible commodes and containment products, such as absorbent pads or catheters. When choosing the optimal product, many things must be considered. Nurse continence advisers are best placed to counsel patients and provide access to these products [5].
The pelvic floor muscle training exercise (PFMT) (kegel exercise) is defined as any program of voluntary pelvic floor muscle contractions taught by a health care professional. Awareness of the pelvic floor muscles is important in order to perform and gain benefit from kegel exercise. The objectives of this exercise are to produce a strong, fast, well-timed contraction, which will clamp the urethra. Approximate the urethra to the back of the pubic bone. Prevent descent of the bladder neck and urethra with coughing, sneezing, etc. Enhance the pressure rise in the urethra, which, following a cough occurs approximately before that in the bladder. These aims can be achieved by regular voluntary contraction and relaxation of the pelvic floor muscles [6].
There are a number of reasons why breathing normally during Kegel exercises is important as Normal breathing during pelvic floor exercises promotes pelvic floor strength, endurance and coordination. Also, the pelvic floor muscles should contract appropriately during everyday activities and actions and these involve breathing at the same time.in addition Practicing coordinated breathing and Kegels helps the pelvic floor muscles to contract strongly when necessary for example coughing and sneezing. It is need to be able to contract the pelvic floor muscles against the force of a normal breath to progress to contracting with more forceful breathing activity [7].
The recommended posture to be adopted during the prescribed exercise regimen also varies and includes sitting, kneeling, standing, lying down and standing with legs astride. The recommended duration of the prescribed regimen varies widely, from one week to six months, with three months being most frequently recommended [8].
Aim of the study
To evaluate effect of deep breathing and kegel exercises on urinary incontinence among menopausal women through:
Study design:
The study followed a quasi-experimental one group (pre-post) test study design.
Study Setting:
The study was conducted at gynecological and urological outpatient clinics at Beni-Suef University Hospital.
Sampling;
Sample type:
A Purposive sample was used from the above-mentioned setting.
Sample Size;
Total sample was 100 women who attended to the previous mentioned setting for a period of 9 months from the beginning of July 2021 until the end of March 2022 with average of three days per week according to the following Criteria.
Tools of data collection:
Tool I: A structured interviewing questionnaire sheet was developed by the researcher in the Arabic language based on a review of recent literatures, under guidance of supervisors. It was consist of:
The first part: included personal characteristics data of the study women such as (age, height, weight, body mass index "BMI" education level, occupation, residence, marital status).
Second part: Obstetrics history such as (number of gravidity, parity, and abortion, mode of deliveries, any complications during pregnancy, labor and post-partum, mode of delivery, weight of baby at birth and duration between pregnancy).
Third part: urinary incontinence history included duration of illness, frequency, amount of leakage of urine, timing (day and night), and predisposing factors as coughing, sneezing, laughing, using sanitary towels for urine leakage, frequency of change the towels.
Supportive material: instructional brochure developed by the researcher based on review of literatures contained data regarding the following:
Validity & Reliability of the tools:
Tools of data collection were investigated for their content validity by three experts in the field of Obstetric and Gynecological Nursing from Faculty of Nursing,Benha University who were selectedto test the content validity of the instruments and to judge its clarity,comprehensiveness, relevance, simplicity, and accuracy. Reliability was done by using Cronbach’s alpha test. Reliability of knowledge equal 77.1, reliability for practice equal 87.2, this indicateshigh degree of reliability of thestudy tools.
Administrative Design:
An official written approval letter for data collection to conduct this study clarifying the purpose of the study was obtained from dean of faculty of nursing, Benha University to the director of Beni-Suef university hospital.
Operational design (field work)
Preparatory phase:
It was included reviewing of local and international related literatures and theoretical knowledge about various aspects of the study problem, and guided the researcher to prepare the required data collection tools. Also, the researcher prepared the instructional brochure which included data about urinary incontinence (definition, causes, symptoms, complications, and management), Kegel exercise (benefits, technique, duration, frequency). Deep breathing exercise (benefit, technique, duration, frequency).
Field work (procedure):
The data was collected through a period of nine months, from the beginning of July 2021 until the end of March 2022. The researcher attended at the previous mentioned setting till all the pre-mentioned sample size collected.
The data was collected through the following phases:
Assessment phase
Firstly, the researcher introduced herself to the studied women and explained the aim of the study and explained the benefits of performing Kegel and deep breathing exercises on stress urinary incontinence to encourage them in the participation in the study and maintain their cooperation. All women interviewed individually using the previously mentioned tools.
Then the researcher started to fill the interviewing questionnaire to assess women's personal characteristics, obstetric history, and urinary incontinence history. After that the researcher assessed the frequency, severity of urinary incontinence and its effect on physical and psychological women’s life by using the International Consultation on Incontinence Modular Questionnaire ICIQ-SF as a pretest assessment.
Implementation phase:
At the beginning of the first month; that started immediately after assessment and included two instructional sessions.
The first instructional session,this session included information about urinary incontinence causes and risk factors, possible ways of management, what are the pelvic floor muscles and their functions, definition of Kegel exercise and its benefits on improving the strength and elasticity of pelvic floor muscles and reducing symptoms of stress urinary incontinence. It took about 10 minutes.
The 2nd session included instructions about how to detect the right muscle group for applying Kegel exercises by instructing the studied women to try to stop the urine flow in the middle of urination, and must experience a feeling of squeezing and lifting in the same time. If she could do this, she was using the right muscles; it took 20 minutes. Also, the researcher provided the instructions to women such as take deep breathing during the exercises; don’t try to move legs, buttock, or abdominal muscles during the exercises, also the researcher instructed the studied women to relax for a period equal to the period of holding [9].
The researcher instructed the studied women to contract the muscle as she is trying to stop the urine follow and count for 3 (3 seconds) and relax for another 3 seconds, contract and relax 5 times (the first exercise group) and repeat this exercise group 5 times per day (25contractions per day) these contractions increased frequently [10].
Moreover, the researcher instructed the women that they can do these exercises at any position at any time also may be done during sexual intercourse. Also, each studied women received brochure about urinary incontinence, breathing exercise and Kegel exercises to remind them with the procedure at home. At the end of the first month: the researcher assessed the accuracy of practicing of deep breathing and Kegel exercises for the last four weeks by using check list tool. Then the researcher instructed the studied women to increase the number of contractions and the duration of holding to 6 seconds and increase the number of contractions and relaxations to 10 times (1st exercise group) and repeat this exercise group 5 times per day (50 contractions per day).
At the end of 2nd month, the researcher assessed the accuracy of practicing of deep breathing and Kegel exercises for the last week by using check list tool. After that the researcher instructed the studied women to increase the number of contractions and the duration of holding to 9 seconds and increase the number of contractions and relaxations to 15 times (1st exercise group) and repeat this exercise group 5 times per day (75 contractions per day).
At the end of the 3rd month the researcher assessed the accuracy of practicing of deep breathing and Kegel exercises for the last week by using check list tool. Then the researcher instructed the studied women to increase the number of contractions and the duration of holding to 12 seconds and increase the number of contractions and relaxations to 20 times (1st exercise group) and repeat this exercise group 5 times per day (100 contractions per day).
Evaluation phase:
The researcher evaluated effect of practicing deep breathing and Kegel exercises on stress urinary incontinence among elderly women as posttest by reassessing the frequency and severity of urinary incontinence and its effect on women’s physical and psychological conditions by using the same tool of pretest and evaluate whether the frequency and severity and the effect of urinary incontinence decreased or not. this tool took about 5-10 minutes.
Statistical Design:
The collected data was revised, coded, tabulated and introduced to a computer using statistical package for social sciences (IBM SPSS .25.0). Data was presented and suitable analysis was done according to the type of data obtained for each parameter.
I- Descriptive Statistics:
1. Mean and Standard deviation (X2±SD) and range for parametric numerical data.
2. Frequency and percentage of non-numerical data
II- Analytical Statistics:
Figure (1): Reveals that (49%) of the studied sample were in the menopausal stage and (51%) were in the late-menopausal stage and (71%) were from rural areas, also (51%) of them were educated and (87%) were married and (52 %) of them were working.
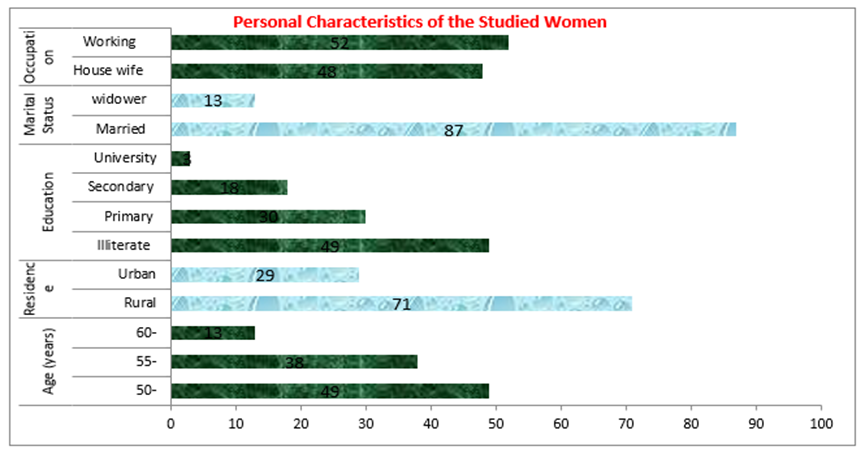
Figure (1): Distribution of studied sample according to personal characteristics (n=100).

Figure (2): Distribution of studied sample according to obstetrics history (n=100). *Results not mutually exclusive
Table (1): Illustrates that (70%) of the studied sample got pregnant and delivered more than three times while (56%) of them aborted from 1-3 times. Regarding type of delivery, about (66%) of them delivered spontaneous vaginally, while about (29%) delivered by cesarean section. Regarding complications during pregnancy (78%) of the studied sample complained from (untreated urinary tract, gestational diabetes, ante partum hemorrhage, anemia and pregnancy induced hypertension) (30%, 19%, 15%, 7%, 7%), respectively, during their previous pregnancies. While complications during labor revealed that about (46%) of the studied sample delivered without any complications while (34%) experienced prolonged labor. Also, complications during postpartum period showed (32%, 18%, and 14%) of them complained from chronic constipation and post-partum hemorrhage and Puerperal sepsis respectively

Person correlation coefficient test *significant at p≤ 0.05 **highly significant at p≤0.01
Table (1): Relationship between frequency of urinary incontinence and women's gravidity and parity (N=100)
Figure (3): Revealed that only 4% of the studied women have normal weight, two-thirds (72%) were obese while one quarter of them (24%) was overweight.
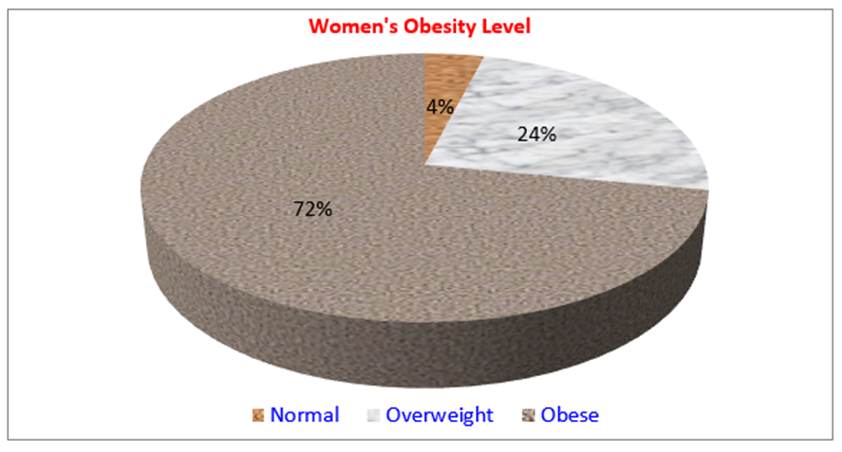
Figure (3): Distribution of studied sample according to their obesity level (n=100)
Figure (4): Presents the relation between women's number of gravida and para and frequency of urinary incontinence. It is clear that 33.3% of women who experienced 1-3 pregnancies reported that their frequency of urinary incontinence is once a week or less often compared to only 14.3% of women who had more than three pregnancies. However, 50% of women who experienced only one labor reported that their frequency of urinary incontinence is once a day compared to only 3.4% & 4.3% of women who had two and three labors, respectively. The figure table shows that there were highly statistical differences in the frequency of urinary incontinence in relation to number of parity and gravidity among the studied sample (p≤0.01).
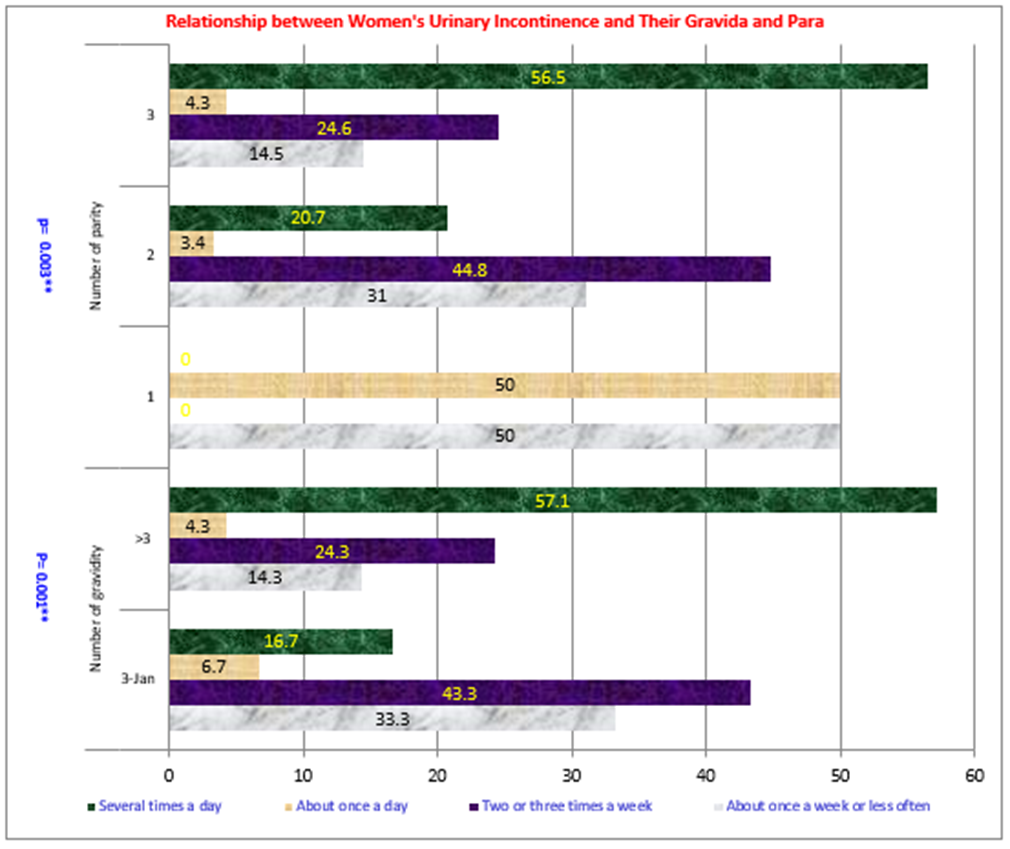
Chi test *significant at p≤ 0.05 **highly significant at p≤0.01
Figure (4): Relationship between women's urinary incontinence and their gravida and para (N=100)
Table (1): Demonstrates the relationship between frequency of urinary incontinence and women's gravidity and parity. A positive correlation between number of gravidity and parity and frequency of urinary incontinence with statistical significant association were found.

Figure (5): Distribution of studied sample according to practicing Kegel and breathing exercise through intervention phases (N=100)
Figure (6): Shows the relationship between body mass index and frequency of urinary incontinence (pre & post intervention): Regarding the frequency of urinary incontinence; at pre-program, 30% of the studied obese women reported two or three times a week. This percentage id decline to 22.2% post program Implementation. However, at pre-program, 51.4% of the studied obese women reported that their frequency of urinary incontinence was several times a day. This percentage declined to 22.6% post program Implementation. It demonstrates that there was statistical significant association between BMI and frequency of urinary incontinence among the studied sample.

Figure (6): Relation between body mass index and frequency of urinary incontinence pre and post intervention (n=100)
Table (2): Indicates that there was negative correlation between regularity of practicing deep breathing and Kegel exercise and frequency of urinary incontinence and highly statistical significant improvement in the frequency of urinary incontinence at the end of the 3rd month of intervention.

Person correlation coefficient test *significant at p≤ 0.05 **highly significant at p≤0.01
Table (2): Correlation between practicing Kegel and breathing exercise and frequency of urinary incontinence through the study (N=100)
Table (3): Reveals that there was negative correlation between deep breathing and kegel exercises adherence and severity of stress urinary incontinence.

Person correlation coefficient test *significant at p≤ 0.05 **highly significant at p≤0.01
Table (3): Correlation between deep breathing and kegel exercises adherence and personal characteristics through
the program phases (N=100)
Figure (7): Demonstrated thatthere was decrease in the severity of urinary incontinence from pre and post application of deep breathing and kegel exercise among the studied women.

Figure (7): Distribution of studied sample according to the severity of urinary incontinence (n=100)
Table (3): Portrays the correlation between deep breathing and kegel exercises adherence and personal characteristics through the program phases. It reveals that there was negative correlation between age of the studied sample and their adherence to practicing deep breathing and Kegel exercises throughout the study.

Person correlation coefficient test *significant at p≤ 0.05 **highly significant at p≤0.01
Table (3): Correlation between deep breathing and kegel exercises adherence and severity of incontinence through the intervention phases
Stress urinary incontinence (SUI) affected menopausal women by reducing social and mental well-being such as loss of self-esteem, impaired body image, decreases the ability to maintain an independent life-style, social isolation, and clothing may become wet with urine which leads to embarrassment, and in particular, fear of unpleasant odor and sometimes sexual difficulties [11].
Kgel exercise offers a possible reprieve from urinary incontinence. This conservative therapy appears to have no significant side effects and enables improvement in symptoms; it can therefore be considered as a first choice of treatment for urinary incontinence in women. The National Institute of Clinical Excellence guideline No. 40 on the management of urinary incontinence in women recommends pelvic floor muscle training for at least three months as the primary treatment for urinary stress incontinence. The guideline states that pelvic floor exercises were found to be effective in the treatment of incontinence in female patients in more than 50% of cases.
The present study aimed to evaluate effect of deep breathing and kegel exercises on urinary incontinence among elderly women through 1-Assess effect of urinary incontinence on the woman’s pattern of life (physical and psychological conditions of women). 2-Instruct elderly women about the technique of deep breathing and Kegel exercises.3-Evaluate effect of application of deep breathing and kegel exercises on elderly woman’s pattern of life (physical and psychological conditions of women).
Finding of the constant study showed that twelve weeks of Kegel and deep breathing exercise elucidate statistically significant improvement of stress urinary incontinence symptoms. This result supported with Chitra (2019) who assessed the role of postpartum Kegel exercises in the prevention and cure of stress incontinence and found that it takes near fifteen weeks of regular exercise for result to be noticeable. Other attributing factors may exist among present study women including; age, menopause, number of pregnancies which may delay the positive effect of Kegel [12]. From the researcher point of view "regularly" is the key word as performance of Kegel infrequently or improbably is not enough to reveal advances.
Also, Hartini et al., (2018) who assessed The Influence of Kegel Exercise on Urine Incontinension Reduction in Elderly and reported that kegel exercise should be applied every day at least twice for 4 weeks, with instructor guidance and facilitator monitoring twice a week. From the researcher point of view the ageing process is a natural process accompanied by a decline in physical, psychological, and social conditions, which allow senility or forget new things [13]. For that reason, Kegel exercise in the elderly needs to be done regularly in a relatively long time and inconsistent monitoring so that the elderly keep doing Kegel exercises regularly and correctly.
Dissimilar to Mohamed et al., (2018) assessed the Effect of pelvic floor muscle strengthening-kegel's exercise on severity of stress urinary incontinence and quality of life among women [14]. Fitz et al, (2019) who studied Impact of pelvic floor muscle training on the quality of life in women with urinary incontinence were congruent with such result; they mentioned that, women with stress urinary incontinence improved greatly in relation to pelvic floor muscle strength and stress urinary incontinence symptoms after the first eight-weeks of demonstrating Kegel [15].
The current study revealed that regular practicing of deep breathing and kegel exercise improved urinary incontinence symptoms. This was in line with at least five studies. First, Dumoulin et al., (2018) who conducted a review about ''Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women''; they concluded that PFMT can cure or improve symptoms of SUI and all other types of UI. It may reduce the number of leakage episodes, the quantity of leakage. They also suggested that PFMT could be included in first line conservative management programs for women with UI [16].
Results of the present study revealed that women’s compliance to perform deep breathing and Kegel exercise increased gradually throughout the study. This progress after the implementation of the program indicated that there is an enhancement in women’s practices. This improvement could be attributed to that all women of the sample were committed with the guidelines, and indicated the success of the program. Additionally, the attending of the guideline’s sessions and the lecture and positive reinforcement or the long-term retention of practices, as well as wide verities of used educational used methods [17-20].
The distributed Arabic booklets, also, played a crucial role in attaining and retain knowledge about kegal and breathing exercise. This is, in accordance, with Edgаr Dаle’s or the NTL’s Pyramid of Learning as cited by Mаsters as the pyramid illustrated that individuals can retain 10.0% of what he read and 20.0% of what he sees and hear (audiovisual). The same author added that ones can retain 50.0% of what he learned by a discussion [17-22].
Concerning relationship between Body Mass Index and the frequency of urinary incontinence, the current study demonstrated that there was statistical difference in the frequency of urinary incontinence in relation to Body Mass Index among the studied women after practicing deep breathing and kegel exercises. This was agreed with Jayachandran (2019) who assessed the Prevalence of Stress, Urge, and Mixed Urinary Incontinence in Women and mentioned that body mass index has been associated with urinary incontinence as the greatest number of women in the overweight and obese categories had stress urinary incontinence [23].
Weight reduction in women who are overweight or obese can substantially improve symptoms and associated bother. Clinicians and patients alike are aware of the challenge this poses for most individuals who are overweight. However, one study showed that, for those enrolled in a weight loss program and losing at least 3–5% of their baseline weight, a 47% reduction in stress incontinence episodes was achieved, with concomitant reduction in urge incontinence episodes. Similarly dramatic improvements have been demonstrated with bariatric surgery and other weight loss modalities [24].
Concerning the severity of urinary incontinence symptoms, the current study showed that there was negative correlation between deep breathing and kegel exercise adherence and severity and frequency of urinary incontinence , this result in consistent with Hung et al., (2019)who assessed the Exercise Adherence to Pelvic Floor Muscle Strengthening is not a Significant Predictor of Symptom Reduction for Women With Urinary Incontinence, Bo K (2020) who assessed Pelvic floor muscle strength and response to pelvic floor muscle training for stress urinary incontinence and Chen &Tzeng (2019) who studied Path analysis for adherence to pelvic floor muscle exercise among women with urinary incontinence, all of them reported that the more adherence to pelvic floor muscle training exercise , the more improvement in urinary incontinence symptoms and decrease in frequency of urinary incontinence [25, 27].
Regarding relationship between personal characteristics of the studied women and deep breathing and kegel exercises adherence the present study revealed that there was a negative significant correlation between age of the studied sample and their adherence to practicing deep breathing and Kegel exercises throughout the study. However, a significant positive correlation was found between deep breathing and kegel exercises adherence in related to women's education, occupation, and residences. This attributed to that age affect all physical and mental capabilities. Edibe, P et al., (2019) supported the idea that age and menopausal state are attribution factors interfering with Kegel's effect and added that age was statistically correlated to SUI [28]. Moreover, Wang & Ying (2019) and tonus & Altman et al., (2019) both of them stated that most of the studied women were illiterate women and there was a significant relation between the prevalence of stress urinary incontinence and illiterate women, this rational why women with (SUI) don’t think that they are need in medical advice [29, 30]. Additionally, Taha (2020) reported a significant relation between the prevalence of (SUI) and unemployed female among Menoufiya women [31]. This is attributed to that the employed had the highest empowerment when compared with the unemployed ones. Work ensures the independence and financial security and provides sources for seeking health care [32].
Remarkable improvement in urinary incontinence according to ICIQ-SF scale is observed after practice of deep breathing and Kegel exercise. Deep breathing and kegel exercises adherence is affected by personal characteristics and body mass index for the elderly women through the intervention phases. Hypotheses were accepted.
Recommendations:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
