
Review Article | DOI: https://doi.org/10.31579/2641-0419/025
1 Garrahan Children Hospital, Buenos Aires, Argentina
2 Buenos Aires Italian Hospital, Argentina
*Corresponding Author: Sebastián Maldonado, Garrahan Children Hospital, Buenos Aires, Argentina.
Citation: Sebastian M., Guadalupe A., Lafuente M Victoria., Monica B., Lopez J Darues. et al. (2019) Update on Pediatric non-Postoperative Junctional Ectopic Tachycardia. J Clinical Cardiology and Cardiovascular Interventions, 2(3); DOI:10.31579/2641-0419/025
Copyright: © 2019 Sebastián Maldonado. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 October 2019 | Accepted: 12 November 2019 | Published: 19 November 2019
Keywords: junctional ectopic tachycardia; ablation; cryoablation; Junctional tachycardia; congenital junctional tachycardia
Junctional ectopic tachycardia (JET) is a rare supraventricular tachycardia more frequently seen in pediatric patients which is associated with high morbidity and mortality without an adequate treatment. Its treatment often requires multiple drugs for arrhythmia control and, in some cases, a cryoablation is indicated. Some patients may revert to sinus rhythm spontaneously after long periods on antiarrhythmic drug.
Currently, the arrhythmia prognosis has improved significantly since cryoablation development and the implementation of a more aggressive pharmacological treatment strategy.
The purpose of this review is to describe the natural history of idiopathic JET and treatment advances.
JET: Junctional Ectopic Tachycardia
AV: atrio-ventricular
VA: ventriculo-atrial
INRT: intra-nodal reentrant tachycardia
Non post-operative junctional ectopic tachycardia is an arrhythmia first described by Coumel in 1976 [1]. JET is a supraventricular tachycardia found in pediatric patients and requires multiple drugs to maintain arrhythmia control [2]. JET is associated with high mortality without drug treatment and, in certain patients, cryoablation is required [2-4]. Development and advances in ablation techniques such as cryoablation and 3D mapping may cure JET with an acceptable rate of success and low complications.
Some studies have demonstrated the existence of cases with spontaneous remission after long periods of treatment with antiarrhythmic drugs [4, 5].
JET Classification
Different types of JET have been described (Figure 1).
Appendix
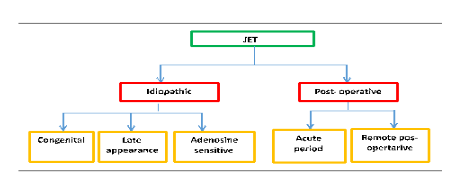
JET: Junctional Ectopic Tachycardia
We can classify JET into 2 groups. On one side those related to cardiac post-operative surgery, mainly those in which the surgery compromises the heart crux. Inside this group, the most frequent form appears during the early post-operative period, generally within the first 24-72 hours being less likely to find in the long term follow up [6-9]. The second group is idiopathic JET, which is divided into 2 subgroups: congenital JET which is the most prevalent and is diagnosed within the first year of life. Some of them can be detected on fetal stage [2-4]. The second form is late onset JET, which usually appears after the third year of life. Both types of idiopathic JET can be associated with congenital heart disease [4]. A third special form of JET, which is adenosine-sensitive and unrelated to postoperative cardiac surgery, can be observed in some complex congenital cardiomyopathies such as univentricular physiology, especially in patients with disbalanced AV defect, heterotaxy syndrome and corrected transposition of great vessels or, sometimes, even in patients without any type of structural cardiomyopathy [10].
Electrophysiologic mechanism
The most prevalent mechanism is an increase in automatism of muscular focus that can be found around the atrio - ventricular node (AV node) [11,12]. JET is generally not induced with atrial stimulation; it cannot be reverted by overstimulation and it can be provoked with isoproterenol infusion. There are some cases in which mechanism is triggered activity since, to be induced, the use of isoproterenol with atrial stimulation is required, and it can be reverted to sinus rhythm with adenosine administration [10].
In some patients, the existence of families with congenital JET suggests a genetic origin of the arrhythmia [2-5]. Xi et al reported a family of 6 members with progressive cardiac conduction defect; two of them also developed congenital JET. Whole exome sequencing was made and a Gen TNNI3K mutation was identified. This gene codifies a Cardiac Troponin linked to MAP kinase, which has been associated with dilated cardiomyopathy, electric conduction disturbance and atrial tachycardia [13].
Clinical manifestations
Congenital JET usually presents as an incessant irregular tachycardia, with a heart rate range between 140 and 370 bpm. In Maldonado et al, the average frequency was 192 bpm [2,3]. High heart rate during long periods of time, irregular rhythm, lack of AV synchrony and low contractile myocardial reserve favors the development of severe dilated cardiomyopathy and heart failure in newborns, sometimes leading to cardiogenic shock [2-5].
Villain et al. reported an incidence of 61.5% with heart failure and shortening fraction reduction [2]. Similar rates were observed in Sarubbi ´s work in which 44.4% presented heart failure and 66% ventricular systolic dysfunction [4]. In Maldonado et al, among 23 patients with congenital JET, 45.5 % had shortening fraction lower than 30%, and 62.5% were admitted into intensive care due to heart failure [5]. Some cases during fetal life have been reported. [14]
Collins et al included 94 patients with idiopathic JET, 16 patients (17%) were diagnosed during the fetal life, 4 of them presented hydrops. The same incidence was shown in Villain et al job, in which 15.3% of the cases were diagnosed in fetal period, all of them with hydrops [2,3]. In idiopathic JET of late onset, the most frequent form of presentation was palpitations. The incidence of tachycardia-induced cardiomyopathy is very low. In our experience, we have 9 patients with late onset JET, and none of them has developed ventricular dysfunction [5].
There are reports of sporadic cases that can develop complete AV block over time [15,16]. In Collins et al work, 3 patients (3,2%) developed AV complete block and a pacemaker was implanted. In Villain et al job, only one patient showed complete AV block (3,8%). In Sarubbi et al series, as well as in our registry, no case of complete AV block was diagnosed [2-4]. Another less frequent clinical presentation is dilated cardiomyopathy not related to tachycardia. In our registry, there were 2 male siblings with congenital JET, both treated with amiodarone and atenolol. A successful cryoablation of the ectopic focus was performed in one of them. The other patient, JET rate slowed down over time, evolving into an accelerated nodal rhythm, even without antiarrhythmic drugs. Both patients, despite having their arrhythmia under control, developed a severe dilated cardiomyopathy; one of them had ventricular fibrillation followed by sudden death, while an implantable defibrillator was indicated to the other patient as primary prevention [5].
Congenital heart disease association is less likely to be found, being it more frequent in patients with single ventricle, corrected transposition of great vessels, heterotaxy syndrome and AV canal defect [10]. Adenosine - sensitive JET is the most prevalent form in these cases. In our experience, a patient with corrected transposition of great vessels, without any surgical treatment, presented an adenosine-sensitive JET refractory to drugs, requiring cryoablation.
Some series show a familiar presentation above 50%. However, in our series only 8,6 % presented family history with JET.
Diagnosis
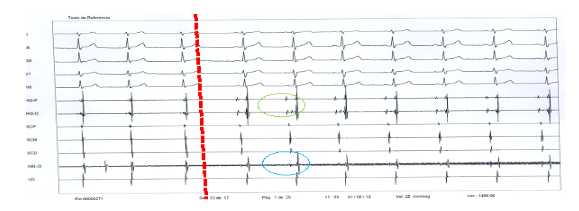
JET diagnosis is mainly electrocardiographic. It is a narrow QRS tachycardia, usually irregular, with AV dissociation. Sporadic sinus captures can be observed, as well as cool down- warm up phenomenon, with a heart rate average above the 95 percentile according to age. (Figure 2) They can sporadically show a 1:1 ventricular atrial conduction. In our work, out of 23 patients with congenital JET, 70% of them were incessant and 92.4% showed VA dissociation, unlike Collins et al report in which VA dissociation could only be found in 56% of Idiopathic JET [3;5]. As it is a tachycardia with very specific characteristics, it is easy to be diagnosed. However, in those variants with 1:1 retro-conduction, a differential diagnosis with nodal reentrant tachycardia has to be made [17].

A Prenatal JET diagnosis can be given with fetal doppler echocardiogram, using a cava / aorta window. The presence of ventricular activation interval faster than atrial and dissociated is characteristic of JET, being a possible differential diagnosis ventricular tachycardia [18].
Mortality
Initial works in congenital JET reported a high mortality. In Villain et al series, the incidence of mortality was 34%, being the cardiogenic shock and the high heart rate the main causes of death [2]. However, recent studies have demonstrated that using more aggressive pharmacological strategies, and arrhythmia ablation in some cases, significantly have improved JET prognosis. In Collins work, the mortality rate was 4%, being the main cause heart failure secondary to tachycardia [3] In Sarubbi et al job, no death cases were shown, while in our registry there was only one case (4,3%) with sudden death due to ventricular fibrillation secondary to severe dilated cardiomyopathy (Figure 3) [4;5]

Spontaneous remission
Natural history of congenital JET patients may have a different course. Some patients may evolve to a spontaneous resolution after long periods of pharmacological treatment. Some of them begin with a drop in the heart rate of the ectopic focus, reaching a normal range according to age, even without antiarrhythmic drugs. Finally, they show longer periods of sinus rhythm, until complete recovery. In our work, 15 % of congenital JET patients presented spontaneous resolution at the age of 4 and 62,5% at 10 years [5]. Collins et al reported 22,3 % patients with spontaneous remission to sinus rhythm and 11,7% evolved towards an accelerated nodal rhythm with controlled heart rate without pharmacological therapy [3]. The presence of an accelerated nodal rhythm without antiarrhythmic drugs, in our experience, is an early sign of congenital JET spontaneous resolution. In our series of 8 patients with late JET onset, all of them required cryoablation due to the symptoms.
Pharmacological treatment
Initial approach in congenital variant is pharmacological therapy. Many studies have evaluated different antiarrhythmic drugs: digoxine [2,3], propafenone [19], flecainide [20,21] sotalol, beta blockers and amiodarone [2]. Usually, the initial response to treatment is a heart rate slow down, often requiring more than one drug [2-5].
Amiodarone has demonstrated to be the most effective drug. In our job, 17.3% was used as a single drug and combined with beta blockers in 69.5%, getting arrhythmia control in 86.8% of the patients [5]. Despite Amiodarone side effects, the incidence in patients younger than 5 years old is lower than the reported among adult population. In our work, only 2 out of 23 patients treated with Amiodarone developed a TSH level increase without clinical manifestation, which reverted after drug discontinuation. One patient showed corneal deposits without visual compromise (13.3%) [5].Unlike congenital JET, patients with late onset JET required a less frequent use of combined drugs. In our experience, 87.5% of patients were controlled by using only one antiarrhythmic agent [5].
Recent studies reported congenital JET refractoriness to the combination of amiodarone and beta blockers, in which beta blockers were replaced by Ivabradine, an IF channel blocker present in cells with automatism, reaching sinus rhythm or an adequate heart rate control in all cases [21-25]. There are also reports of postoperative JET with positive results [26,27]. This drug has the advantage of giving an antiarrhythmic effect without affecting inotropism, with a low rate of side effects. In our experience, we only used it in one patient with congenital JET refractory to amiodarone and atenolol. Ivabradine allowed an adequate rate control of the arrhythmia, and due to significant drop in heart rate Amiodarone, it could be discontinued.
Nifekalant and Vernakalant are fast potassium currents (IKr) blockers that are located mainly in the atrial tissue, increasing refractory period. Aoki et al published a report of 2 patients with congenital JET refractory to multiple drugs, including amiodarone, in which patients were treated with Nikefelant, achieving arrhythmia control in both cases [28].
Non pharmacological treatment
Development of invasive procedures for treating arrhythmias lead to positive results as many of them could be treated without the need of AV node ablation and pacemaker implantation. The first studies published about JET ablation were with radiofrequency therapy. Although in most cases it could be ablated successfully. However, as the arrhythmogenic substrate is close to specialized cardiac conduction system, the risk of complete AV block is also higher than in other arrhythmia ablations. In Collins et al registry, 18% of JET patients in whom radiofrequency ablation was performed presented complete AV block due to the procedure [3]. In the last decades, a new technique of ablation using cold, known as cryoablation, has been developed. Cryoablation generates small regular lesions with no endothelium disruption, allowing application at intermediate temperatures of -30ºC (cryothermal mapping), which generates reversible lesions, helping to avoid an AV node or HiS damage. When the ectopic focus is eliminated and no conduction system disturbance is seen, temperature is reduced to – 80°C to generate an irreversible lesion. Generally a double freeze-thaw applications of 240 to 480 seconds are performed (figure 4).
Differential diagnosis
Differential diagnosis will depend on ventriculo-atrial (VA) conduction. If there is a VA relation 1:1, the main differential diagnosis to be made is with Intranodal Reentrant Tachycardia (INRT) since both of them show retro-conduction through the fast nodal pathway, generating a similar electrocardiogram. However, electrophysiological mechanism in INRT is reentrant, while in JET it is usually automatic or by triggered activity and all the electrophysiological maneuvers to distinguish one from another are based on this difference.
Wang et al, described a maneuver, which consists of performing a brief over atrial stimulation 30 ms faster than the tachycardia cycle length and evaluating the difference between the last entrainment VA interval (VAp) and the tachycardia VA interval (VAt). In patients with INRT, since the AV node is part of the circuit, the difference between the 2 intervals is similar, all patients with INRT had values less than 22,5 ms, whereas JET patients had more than 294,9 ms in all cases [31].
Srivathsan et al suggested entraining tachycardia from the base of the right ventricle and measuring delta HA between the last entrained beat and the one of the tachycardia. A delta HA > 0 ms was seen more frequently in JET patients (sensitivity of 89% and specificity of 83%) [32].
Padanilam et al mentioned the use of atrial extra-stimulus during tachycardia and to evaluate the effect on His activation. There are 2 moments in which the maneuver can be done: an extra stimulus given in a His refractory period, if His electrogram is advanced and the arrhythmia is an INRT, since the only way to obtain that response is by the existence of a nodal slow pathway, whereas if the next HH interval does not change its cycle, it is more likely to be a JET. The second moment in which extra-stimulus can be given is when His is permeable. If His is advanced and tachycardia is terminated, the arrhythmia is more likely to be an INRT, since the anterograde activation of the nodal fast pathway does not allow to be activated in a retrograde way as a result of being in a refractory period. If tachycardia continues, it is more likely to be JET since the nodal fast pathway is not a crucial part of the circuit [33].
Finally, Fan et al suggested entraining tachycardia from the atria 30 ms faster than the tachycardia cycle length, if tachycardia persists when the stimulation is stopped and the response obtained is AHHA, the tachycardia is a JET in 100 % of the cases, whereas an AHA response is observed in all patients with INRT [34].
In JET patients with VA dissociation, differential diagnosis is with nodo-fascicular orthodromic tachycardia, whose mechanism is reentrant. This tachycardia, unlike the JET, can be provoked with atrial or ventricular stimulation; it can also develop QRS pre-excited with rapid atrial stimulation, present a variation of the cycle tachycardia length with the development of bundle branch block, and stop the tachycardia or the advancement of His potential, with an extra-stimulus on His refractory [35].
JET location
With regards to ectopic focus location in JET, there are differences among published studies (Fig. 3). In Law et al work, cryoablation was performed in 6 patients; in 4 of them the focus was located in the upper third of the Koch triangle, near the His [30], whereas in the registry of Pierrick et al the focus location was: 4 in the posteroseptal, near coronary sinus ostium, 4 in the low middle septal, over coronary sinus ostium, 4 in high middle septal area and 2 in the antero-septal near His [29]. In our series of 13 patients with JET who went through cryoablation, the location was: right posteroseptal in 2 patients, 3 in low middle septal, 4 in high middle septal and 3 in anteroseptal, near His (figure 5) [5].
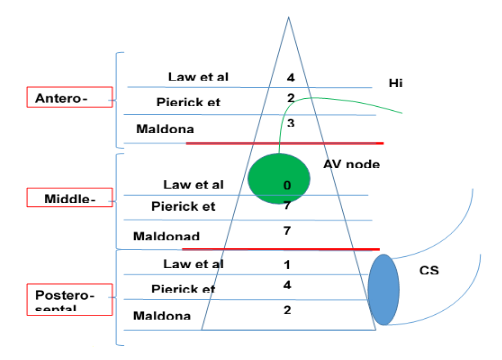
As Pierrick work, in our experience, the focus location in the lower 2/3 parts of Koch triangle was associated with a bigger success of the procedure, whereas those located in the upper third had a lower primary success or recurrence [29].
Therapeutic approach
In figure 6, a therapeutic approach for congenital JET patients is proposed. In those patients with low weight (less than 15 kg), cryoablation can only be contemplated when the patient is refractory to pharmacological treatment and hemodynamic decompensation secondary to the arrhythmia, or in the presence of antiarrhythmic side effects.
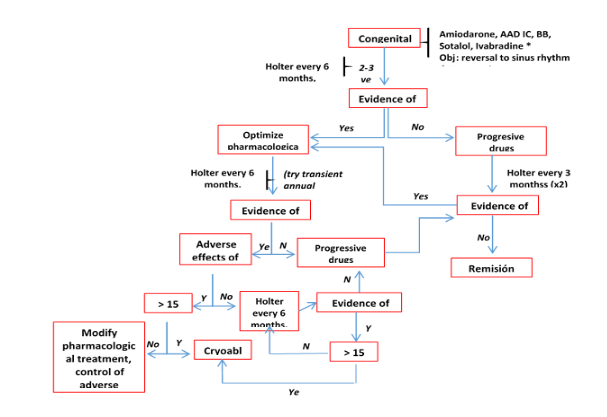
In those patients over 15 kg, cryoablation can be indicated. As many patients could evolve to spontaneous resolution of congenital JET over time, we believe, that cryoablation can be postponed for longer periods of time, if the patient tolerates pharmacological treatment, without side effects. With regards to late onset JET patients, no patient presented spontaneous arrhythmia remission, requiring a cryoablation in all cases [5,35,36].
Congenital JET is a rare tachycardia and, without an appropriate diagnosis or treatment, it is related to a high morbility and mortality. Currently, there are a wide number of antiarrhythmic drugs that help us control the arrhythmia and get a better prognosis. Development and advances in ablation techniques, particularly in cryoablation and 3D mapping, let us achieve the cure of JET in most cases with low complications.
none
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
