
Case Report | DOI: https://doi.org/10.31579/2690-8808/205
University of Utah, Dept. of Internal Medicine.
*Corresponding Author: Meenu Singh, University of Utah, Dept. of Internal Medicine.
Citation: Ryan Truitte and Meenu Singh (2024), Unveiling the Hidden Culprit: A Commonly Used Medication Triggers Persistent Hiccups, J, Clinical Case Reports and Studies, 5(5); DOI:10.31579/2690-8808/205
Copyright: ©, 2024, Meenu Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 June 2024 | Accepted: 25 June 2024 | Published: 03 July 2024
Keywords: dexamethasone; hiccups; chemotherapy
Hiccups are considered minor symptoms in general by patients and providers and are therefore often underreported. Persistent hiccups have the potential to cause significant discomfort affecting speech, oral intake, sleep, mood, exhaustion and pain. There is very limited data on incidence and prevalence of prolonged hiccups. This is compounded by under-recognition of some of the causes of hiccups, especially drug induced hiccups. The etiology of hiccups is vast. Commonly known causes include structural, infectious, and inflammatory processes involving abdominal and thoracic viscera, brain and electrolyte imbalances. Common medication triggers include benzodiazepines, barbiturates, opioids, antiemetics(ondansetron), antibiotics(azithromycin) and chemotherapy. Steroids, dexamethasone particularly, is an under-recognized and underreported cause of DIH. Oncology patients are particularly predisposed to hiccups secondary to frequent use of dexamethasone in this patient population besides use of other predisposing factors including chemotherapy, radiation, antiemetics and other structural causes. In oncology patient's hiccups is a less well researched symptom, though it has been reported to affect >20% oncology patients, with less than ten percent seeking care for the symptom. Corticosteroids have emerged as a relatively less well-known cause of hiccups in this population, with the first case of Dexamethasone Induced Hiccups (DIH) reported in 1982. Dexamethasone is more strongly associated with hiccups as compared to other steroids likely secondary to differences in permeability into blood brain barrier. Incidence of DIH has been reported to vary from 6.3% in a recent study in COVID patients to 61% with very high doses of dexamethasone. Our case describes a patient's experience with severe dexamethasone induced hiccups who failed to improve with conventional non-pharmacologic and pharmacologic first line therapies. Once dexamethasone was recognized as a possible cause, steroid rotation from dexamethasone to methylprednisolone led to quick hiccup resolution. Our case report aims to improve awareness of dexamethasone-associated hiccups in medical practitioners and provide a potential for simple effective treatment when association is recognized by the treating providers.
Steroids are one of most prescribed medications in oncology patients for anti-emetic, anti-inflammatory, antiproliferative, vasoconstrictive and immunosuppressive properties. Though steroids can help improve outcomes and quality of life, common adverse effectsinclude hypertension, hyperglycemia, neuropsychiatric side effects including insomnia, glaucoma, peptic ulcer disease, higher risk of infections, and reduced efficacy of Immune Checkpoint InhibitorTherapy. Persistent hiccups are a less well-known side effect of steroids [1]. To our knowledge the first case was reported in 1982 with dexamethasone use prior to resection of intracranial tumor [2]. Most of the cases of steroid induced hiccups have been reported in oncology patients, especially in association with dexamethasone [Peacock, 2013]. Stopping dexamethasone is not a feasible option in many patients especially with risk of recurrence of symptoms including nausea, emesis, pain and increased intracranial tension. There is limited literature on treatment of hiccups including DIH. Frequency of persistent hiccups can vary from 2-60 per minute. Rotation to methylprednisolone has been shown to reduce severity of DIH by 77% [4]. With the rising prevalence of cancer, and therefore increasing use of dexamethasone in oncology patients, it is important to be aware of unique drug specificside effects, and theirmanagement to improvepatient care and outcomes.
Our patient was a 62-year-old man with Stage IV EGFR-mutated adenocarcinoma of the lungs with widespread metastasis (brain, bone, adrenal glands, lymph nodes, pleura, and leptomeninges). He presented to the emergency department with posterior headaches, worsening confusion over the preceding ten days, and inability to void on the day of admission. He had recently been taken off the EGFR inhibitor Osimertinib due to continued diseaseprogression. Planned radiationtherapy was postponed due to his progressive confusionand headaches.
On presentation, his initial vital signs were normal. Physical examination revealed he was oriented only to self, had slurred speech, and slow verbal responses with unintelligible answers. An MRI of the brain showed worsened leptomeningeal diseaseand associated edema throughout the vermis and bilateral cerebellar hemispheres, causing effacement of the fourth ventricle and hydrocephalus (Figure 1). Previous bilateralfrontal and left temporal metastatic lesions were unchanged in size comparedto prior imaging.
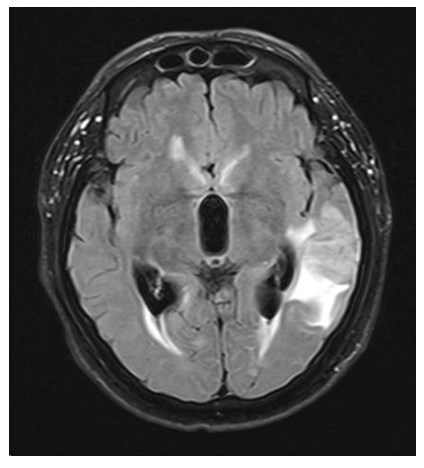
Figure 1: Brain MRI
He received 8 mg of dexamethasone and 1 g of Keppra and was admitted to the medical oncology unit with a continuation of dexamethasone 4 mg every 6 hours. On the first day of admission, he underwent right parietal ventriculo-peritoneal (VP) shunt placement to relievehydrocephalus. His mentalstatus gradually improvedto baseline over the next several days.
On the third hospital day, he began to experience hiccups, which disrupted his ability to eat and drink. By the fifth hospitalday, the hiccupshad increased in severity, interrupting his speech, sleep, oral intake, and other daily activities. At this point, he was unable to tolerate any oral intake, so all medications were switched to IV, and tubefeeding was initiated. Intravenous baclofen and nonpharmacological methods failed to improve the hiccups. The differential diagnosis for the hiccups included cancer progression involving the lung and brain, increased intracranial pressure, and iatrogenic causes related to the VP shunt and intubation in the operating room.
On the sixth day, dexamethasone was identified as a suspected trigger of his hiccups, leading to a transition to methylprednisolone 40 mg twice a day. By the ninth day of hospitalization, the hiccups had resolved. On the tenth day, the NG tube was removed as he was tolerating oral intake, and he was discharged to the inpatient rehabilitation center.
Hiccups result from involuntary, intermittent, synchronized, spasms of the diaphragm and intercostal muscles leading to sudden inhalation followed by closure of the glottis resulting in the characteristic sound. Most acute hiccup attacksare transient and resolve spontaneously. Persistent hiccups, lasting >48 hours, are more likely to be attributable to serious underlying pathology and have a greater effect on quality of life. Intractable hiccups are defined by hiccups lasting more than a month. Persistent or intractable hiccups can have a negative effect on activities of daily life, speech, eating and drinking, sleep and mood, weight loss, tiredness, exhaustion, and may increase intensity of pain [5], and may result in cardiac events [6]. Hiccups mayhave further sequelae as suggestedby a case report from 2013 describing a patient with pharyngitis who developed hiccups and bouts of convulsive syncope [7].
Most hiccups are triggered by structural, infectious, or inflammatory stimuliwhich impact either the central nervous system or the vagus or phrenic nerves or their branches [Peacock, 2013]. Specifically, within the oncology and palliative care patient population, causes include chemotherapy, steroids, antiemetics, electrolyte abnormalities, esophagitis, and neoplastic involvement of nervous, cardiothoracic or airway structures[5]. (Table 1)
| Cause of Hiccups | Example of triggers |
| CNS causes | Stroke, AVM, Intracranial neoplasms, abscesses, head trauma, multiple sclerosis hydrocephalus, syringomyelia |
Phrenicor Vagus nerveirritation | Goiter, pharyngitis, laryngitis, foreign body aspiration, head and necktumors, intubation, neck surgery, gastric distention, visceral organ traction |
| Gastrointestinal | GERD, ulcers, gastritis, pancreatitis, abdominal abscess, gallbladder disease, IBD, hepatitis, esophageal dysfunction, bowelobstruction |
| Respiratory | Pneumonia, lung neoplasm, empyema, bronchitis, asthma, pleuritis, mediastinitis, PE |
| Vascular | Temporal arteritis |
| Cardiogenic | MI, Pericarditis |
| Metabolic | Diabetes with poor glucose control, Hypocalcemia, hyperkalemia, hyponatremia |
| Infectious | Neurosyphilis, Malaria, TB, COVID- 19 |
| Toxins/irritants | Alcohol, Spicy foods, Carbonated beverages, Caffeine |
| Medications | Corticosteroids, Chemotherapy (especially platinum agents), antiemetics, alpha methyldopa, barbiturates, benzodiazepines |
| Psychogenic | Anorexia, conversion disorder, malingering |
Table1: Causes of hiccups
Some of the other causes of hiccups include intubation, sudden temperature changes, psychological causes, alcohol, smoking and phenothiazines. Although specific etiology is often not found, it is importantto obtain a detailed historyand physical examination as well as diagnostic testing to search for underlying disease and plan for targeted therapeutic intervention [9].
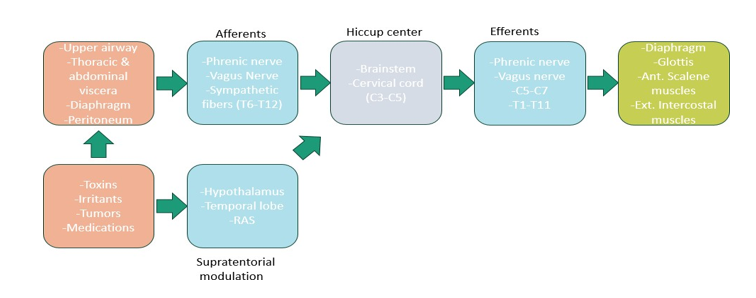
Figure 3: Hiccup Reflex Arc
Incidence of hiccups in cancer patients has previously been reported to be 0.4% [1]. Yet, reporting is widely variable and patients with advanced stage cancers in a study were noted to experience hiccups at rates as great as 1% to 9%. In a cross- sectional study of 160 cancer patients, >20% suffered from hiccups. Importantly, these are more likely to be defined as persistent or intractable [5]. Despite these overall seemingly low reported incidences of hiccups, nearly 4,000 cancer patients are hospitalized for this symptom in the US annually which likely represents a fraction of the totaldisease burden amongthis population [4]. Predisposing risk factors are not well-known. One study, in the setting of cancer, found risk factors for hiccups to include male gender, young age, overweight/obesity, the use of alkylating anticancer agents (particularly as the first anticancer drug), high levels of hemoglobin, serum creatinine, uric acid, and albumin, and an elevated body temperature [10].
Most hiccups, even amongst cancer patients, are self-limited and do not have dire consequences. It was found that only 10.8% of patients suffering from hiccups used pharmacological methods for relief and that 27% used nonpharmacological methods [5]. Treatment options include physical maneuvers, medications and surgical intervention. Non-pharmacological methods are first line intervention and include breath holding to induce hypercapnia, vagal stimulation by performing Valsalva maneuver or gently pressing on eyeball, drinking cold water, biting into lemon, pulling on tongue. Chlorpromazine is the only FDA (Food and Drug Administration) approved drug for hiccups. It has significant side effects including hypotension, sedation, urinary retention, and glaucoma.
Other agents commonly used include baclofen, metoclopramide, and empiric proton pump inhibitors [5]. Of these the first line options are unclear as there is a paucity of high-quality evidence to drive treatment algorithms [Steger et al., 2015]. The two medications most linked with hiccups are corticosteroids and benzodiazepines [Peacock, 2013]. Steroids associated with hiccups include dexamethasone, methylprednisolone, betamethasone, triamcinolone, through oral, intravenous, intra- articular, and epidural routes.
Dexamethasone is more strongly associated with hiccups than other steroids, likely secondary to increased permeability across blood brain barrier and ability to lower synaptic threshold compared to other steroids. This association has been seen to have a direct dose dependent relationship [5] with noted incidence of 63% with dexamethasone dose of 120 mg over 5 days in a study. Most cases of DIH have been described with doses ranging from 8-40 mg daily and onset 1 hour to 18-hour after first dose and duration lasting 1 to 9 days. Notably, Dexamethasone associated hiccups are seen approximately eleven times more commonly in males comparedto females [1] (Figure 3). It has been postulated to be secondary to males having higheraffinity for dexamethasone and wider steroidreceptor distribution.
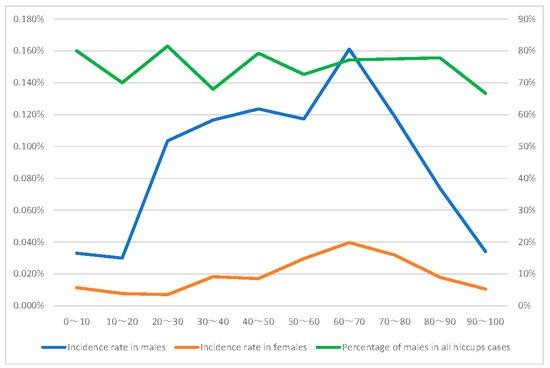
Figure 3: Male and female incidence rates and the percentage of males in cases of hiccups. The graph shows the age on the horizontal axis and the incidence rate (%) on the left vertical axis. The percentage of males in all hiccup cases is shown on the right verticalaxis.
Male and female incidence rates and the percentage of males in cases of hiccups. The graph shows theage on the horizontal axis and the incidence rate (%) on the left vertical axis. Thepercentage of males in all hiccup cases is shown on the right vertical axis.
Dexamethasone is frequently used to treat chemotherapy induced nausea and vomiting [1]. This is especially important when considering that 70-80% of cancer patients receiving chemotherapy experience nausea and vomiting during their treatment[10] and often are prescribed dexamethasone. Current guidelines recommenddexamethasone as part of multidrugregimen in prevention of nausea and vomiting before chemotherapy in patients receivingemetogenic antineoplastic agents or radiation therapy.
Of the few studies done to evaluate corticosteroid-induced hiccups, it appears that the phenomenon may be relieved by transitioning to a different steroid [1]. A small case series of five patients indicated that switching steroids alone may relieve the hiccups without additional baclofen, haloperidol, or metoclopramide [4]. The improvement in symptoms upon transitioning between corticosteroids hinges on their differing effects on the hiccup reflex arc with the shift from dexamethasone to another steroid, typically methylprednisolone, exhibiting greater efficacy compared to the reverse scenario [1]. Additionally, there has been some evidence of tolerance to dexamethasone where its reintroduction following complete resolution of an episode of hiccups did not involve a repeated episode of severe hiccups [4].
Corticosteroids are some of the most prescribed medications, especially in the field of oncology. Steroids, especially dexamethasone, have been associated with less commonly known unusual adverse effect hiccups. Hiccupping may often be consideredunimportant by patients and is underestimated by many clinicians, yet intractable hiccups can have serious consequences in cancer patients who are already an at-risk population. This together with the fact that most clinicians, including the ones whoprescribe steroids, are unaware of this side effect can lead to added patient suffering, poor quality of life, continuation of offending agent, unnecessary interventions and prolonged hospital stay. Our case report aims to improve awareness of dexamethasone-associated hiccups in medical practitioners and provide a potential for simple effective treatment of steroid rotation when association is recognized by the treating providers.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
