
Case Report | DOI: https://doi.org/10.31579/2768-2757/146
1 Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran.
2Department of Pulmonology, Guilan University of Medical Sciences, Rasht, Iran.
3 Department of Rdiooncology , Guilan University of Medical Sciences, Rasht, Iran.
4 Department of pathology, Guilan University of Medical Sciences, Rasht, Iran.
5 Department of Radiology, Guilan University of Medical Sciences, Rasht, Iran.
6 Inflammatory Lung Diseases Research Center, Department of Internal Medicine, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
*Corresponding Author: Manouchehr Aghajanzadeh., Department of Thoracic Surgery, Guilan University of Medical Sciences, Rasht, Iran.
Citation: Aghajanzadeh M., Gafernejad A., Hamidi S Saidi., Talebi A., Khyabani M., Omid M Rad., Sadin Z., and Farzin M., (2024), Unusual Presentation of a Posterior Mediastinal Schwannoma Associated with Chest Pain, Cough, Hemoptysis and Dyspnia., Journal of Clinical Surgery and Research., 5(8); DOI:10.31579/2768-2757/146
Copyright: © 2024, Manouchehr Aghajanzadeh., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2024 | Accepted: 25 November 2024 | Published: 29 November 2024
Keywords: neurogenic tumors; thoracic; pediatric; morphology
Neurogenic tumors(NT) are the most common of posterior mediastinal tumors an 80% of all posterior mediastinal tumors are (NT). They originate from the spinal cord, sympathetic ganglia, or peripheral nerve roots. A schwannoma is a slow-growing, encapsulated, and benign neurogenic tumor. Fewer than 9% of schwannomas are located in the mediastinum. Posterior mediastinal schwannomas originate from neural crest cells and typically from the intercostal nerves. Mediastinal schwannomas are often asymptomatic but may present with unusual symptoms as cough or dyspnea and hemoptysis because of pulmonary invovovement. Although a definitive diagnosis is made by histopathology and immunohistochemical analysis and electron microscopy can be used to help ite final diagnosis. We present a case of a benign posterior mediastinal schwannoma which present in CXR and computed tomography (CT) imaging as a cystic lesion in a 58-year-old woman who admitted to our hospital with back pain,cough,hemomptsis and dyspnea.
A 58-year-old woman was refered to our hospital with a history of recurrent right side chest wall pain ,cough ,night sweating ,hemoptysis and dyspnea for 4-6 weeks. A physical examination revealed respiratory sounds were decreased on the middle right side of chest. His complete blood count, erythrocyte sedimentation rate, CRP blood urea nitrogen (BUN) level, and creatinine level were normal and liver function tests (AST,ALT ,AKP and bilirubin ) and anti hydatid tests were normal . Poster anterior (PA) and lateral chest radiographs were performed . The PA chest radiograph (Figure 1)showed a well-defined 10- to 14-cm right paracardiac cystic mass located in the right middle zone of chest. The CT-scan showed a large well –defined hypo dense cystic mass measuring 112 mm is seen in superior segment of RUL.Sub segmental atelectasis also seen in right lung caused compressing. Left lung was normal . Figure 2(a,b,c,d,e,f,g,h,i) . In the CT –scan there was no invasion of the chest wall and others intrathoracic structures. CT images show no enlargement of lymph nodes and pleural effusion but lung parachymal was involved.The testes for hydatid cyst were negative .Ultrasonography of abdomen was normal . A classic right posterolateral thoracotomy in six intercostal space was performed. Around of cystic lesion was walling off with wet sponge with normal Saline (Fig 3). In the aspiration of the lesion there was a hemorrhagic dense viscous fluid .The cystic mass was completely removed without complications and free margin. On the operation time , macroscopic examination show hemorrhagic dense viscous fluid and debris was observed in the center of the lesion(Fig 4) Microscopic examination showed an encapsulated mesenchymal neoplasm composed of short fasciles of bland looking spindle cell which are diffusely positive for S100 and GEAP on immunohistochemically diagnosis was a schwannoma tumor. The patient was discharged on the 6 th postoperative day. The patient did not recurrence after 8 month of follow-up

Figure: 1 CXR show right side lung cyst.

Figure: A, B
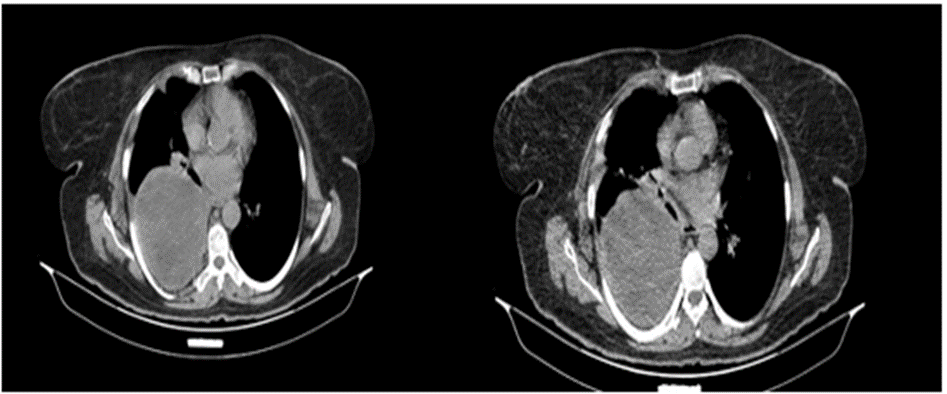
Figure: C, D
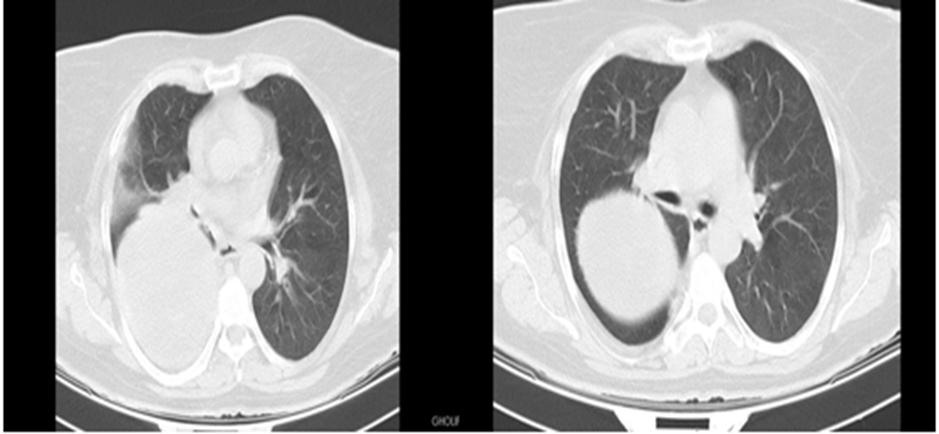
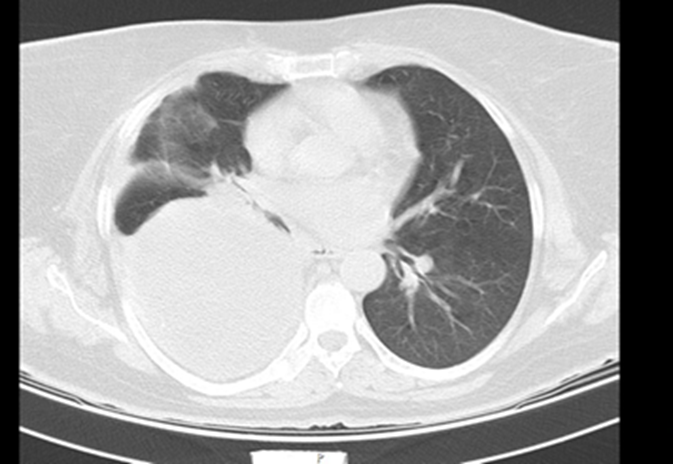
Figure: E,F,G
Figure: 2 CT -scan A, B, C, D, E, F, G show solid cystic lesion.
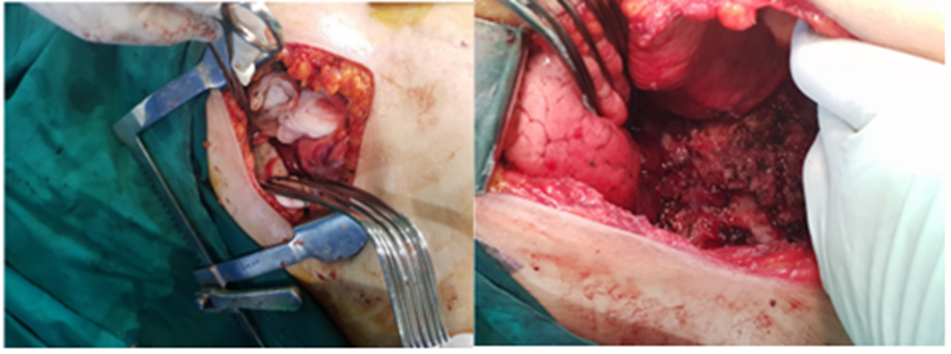
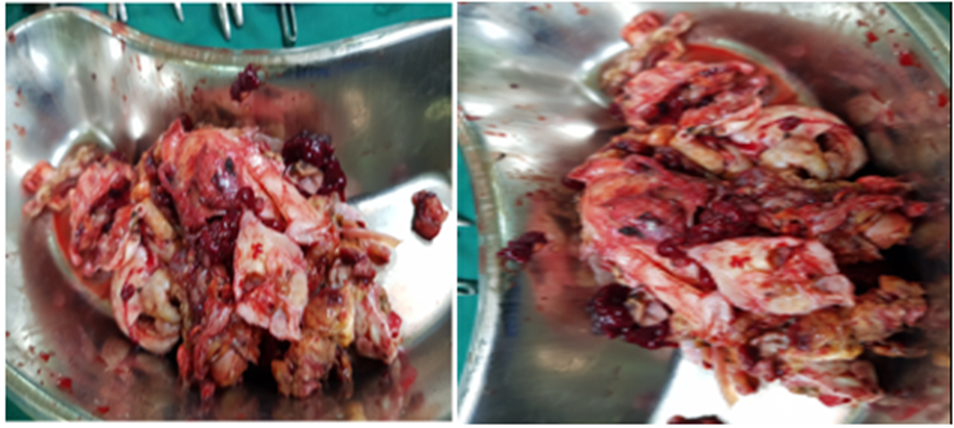
Figure: 3- A, B, C, D show walling of aroun cystic lesion for prevention of spillagechstic fluid and debris of cystic masses.
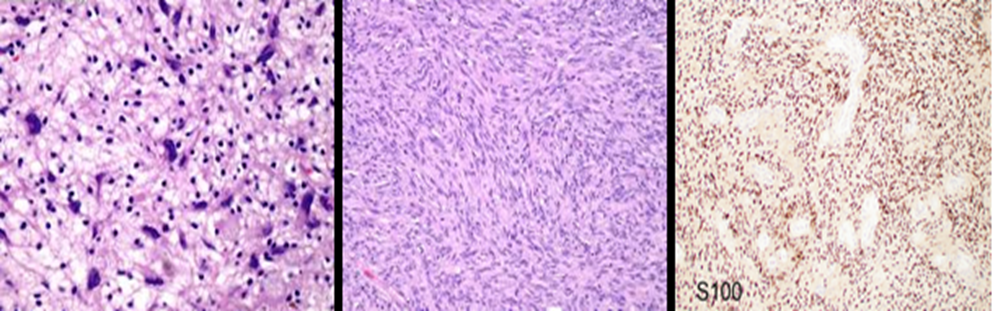
Figure: 4- A, B,C pathology Microscopic examination showed an encapsulated mesenchymal neoplasm composed of short fasciles of bland looking spindle cell which are diffusely positive for S100 and GEAP on immunohistochemically diagnosis was a schwannoma tumor.

Figure: 6 CXR 8 month postoperative.
The anterior border of The posterior mediastinum is pericardium and trachea, posterior border and lateral border is inner chest wall and the spine colom [2,3] Organs contains of posterior mediastinum include of descending aorta, esophagus, thoracic duct, and vagus nerve [1,2,3 14]. neurogenic tumors of posterior mediastinum originate from the neural crest as peripheral, sympathetic, or paraganglionic elements. tumors of lymphatic, vascular, and mesenchymal origin may also occur [1,2,3,4]. Posterior mediastinal masses and lesion according to their origin and morphology can divide as neurogenic, esophageal, cystic, extramedullary hematopoiesis, or lymphoma. 80% of posterior mediastinal masses are Neurogenic tumors 4. about 10- 20% of [2,3,4,7,8,22]. Lesions are malignant [3,4]. neurofibroma, schwannoma, neurogenic sarcoma originate from peripheral nerve roots. ganglioneuroma, ganglioneuroblastoma, and neuroblastoma originated from aorticosympathetic paraganglia and paravertebral paraganglioma or from sympathetic ganglia in the Posterior mediastinum or rarely, meningocele or meningomyelocele origenited from the intrathoracic spinal canal (1,2,3,4,5,9,10). Among mediastinal neurogenic tumors, schwannomas and neurofibromas arise from peripheral nerves and are more common in adults, whereas ganglioneuromas and neuroblastomas arise from sympathetic ganglia and are more common in children [3,4,5,6,7,11,12]. The most common pediatric mediastinal neurogenic tumors are the ganglioneuroma and neuroblastoma [2,3,4,5]. While the ganglioneuroma is a benign tumor, the neuroblastoma is highly malignant [2,3]. In the adult population, the neurofibroma and schwannoma are most common, with the schwannoma being the most common posterior mediastinal neurogenic neoplasm [2,3,4,6,8,9]. Schwannomas are often asymptomatic and incidentally detected during imaging. Schwannomas are mostly solid tumors, some of which may contain cystic degenerations or hemorrhages as our case. Rarely they present as a completely cystic lesion [8,9,10,11] . Schwannomas originating from the nerve roots are located in the paravertebral area, and in the anterior vertebral corpus and neural foramen. PA and lateral chest x-rays are usually the first test performed, as our case [2,3,4,5,15,16,22]. but a CT scan with intravenous contrast is the most valuable test for mediastinal lesions. In this case after CXR we used CT-scan [2,3,4,5,8], Posterior mediastinum masses usually compress the lung and produce Symptoms may occur due to the compression of adjacent mediastinal structures, such as the airway, esophagus, heart, and great vessels [2,3,5,15,16]. Although they are rarely malignant, they may cause respiratory symptoms, such as stridor, dyspnea, hemoptysis, and cough, or gastrointestinal symptoms, such as dysphagia, in the case of invasion to local structures [3,4,5,18].4. Our case present with cough, dyspnea, chest pain and hemopetsis. Symptoms of posterior mediastinum neurogenic tumors include compression of the airway, esophagus, heart, and great veins. Malignant tumors of this area can of invasion into the tracheobronchial tree, spinal canal, lungs, esophagus, superior vena cava, pleura, and chest wall, these invasion can produce cough, stridor, dyspnea, hemoptysis, dysphagia, pleural effusion, and superior vena cava syndrome and hoarseness, neuropathic pain, diaphragmatic paralysis, or Horner’s syndrome and Paraneoplastic syndromes.in our case presentation was due to compressions to adjacent organs involvement [2,3,4,5,9,18,19]. The initial workup of a posterior mediastinal mass involves radiographic evaluation, with the majority of asymptomatic masses discovered incidentally on posteroanterior (PA) and lateral radiographs [2,3,4,14]. Additional radiologic findings include enlargement of the neural foramina (creating a dumbbell shaped lesion), scalloping of posterior vertebral bodies, erosion of the ribs, pleural effusion, and scoliosis. Disruption of the azygoesophageal recess is a nonspecific finding seen in both middle and posterior mediastinal masses [3,16,17] Posterior masses generally have sharp margins due to their interface with the lung, CT imaging of the mass is useful in determining the exact location and its relationship to adjacent structures and may aid in differentiating tissue densities between cystic, vascular, and solid masses [2,3,4,6,7]. Due to high contrast resolution and multiplanar capability, MRI is the preferred modality of imaging as it provides better evaluation regarding the nature and extent of intraspinal involvement towards the neural and vertebral foramen [3,17]. The limitations of MRI compared to CT are the limited radiographic evaluation of calcifications and poorer spatial resolution [2,3,4,16,17] therefore, while an MRI is preferable it is not always necessary we do not MRI in our case [2,3,21]. Recent studies have offered ultrasound guided FNA as a viable diagnostic modality for accessible mediastinal lesions [2,3,23] allowing for formal diagnosis without the potential complications from more invasive procedures such as CT-guided biopsy, mediastinoscopy, or video-assisted thoracoscopic surgery which offer no benefit in the management of these tumors [2,3]. Because of suspicion of hydatid cyst our radiologist team do not use FNA [23.24]. ,hydatid cyst in IRAN are endemic [22].PET scans have shown the ability to distinguish between malignant peripheral nerve sheath tumors and neurofibromas with high accuracy but are not as helpful in distinguishing between benign and malignant peripheral nerve sheath tumors [2,3,16,17] Primary treatment of schwannoma and most neurogenic tumors are Surgical resection [2,3,4,5,19]. schwannomas mayoriginate from the vagus, phrenic, or any part of the intercostal nerve and removed of tumor should be removed by a saving the involved nerve [2,3,18.19], Radiation therapy may be used postoperatively to control residual disease in malignant schwannomas, but its benefit is unknown [2,3,4,5]. No known chemotherapeutic regimens are effective against these tumors [3,5,6,7]. Since serologic markers are absent and characteristic imaging abnormalities are variable, tissue pathology and immunohistochemistry are required for a diagnosis [11,12,13] . Schwannomas are composed of spindle cells with twisted nuclei, amphophilic cytoplasm, and rare mitoses [2,3.11,12,13]. Patients with neurofibromatosis are likely to display a variant form called plexiform schwannoma [12,13]. Another variant, the melanocytic schwannoma, has a pronounced brownish cytoplasmic pigment and malignant potential [11,12,13]`. The malignant schwannoma, the most dangerous variant, is a soft gray-pinkish tumor with central necrosis and microscopically consists of sheets of pleomorphic spindle cells with numerous mitotic figures and necrotic areas [3,11,12,13]. Malignant schwannomas may also exhibit a variety of cellular components such as clusters of epithelial cells; mucin-secreting glands; and even mesenchymal features such as bone, cartilage, or skeletal muscle [3,10,11,12,13]. Patients who undergo resection of a benign schwannoma are generally followed up to monitor wound healing and resumption of daily activities. Routine follow-up of patients who undergo curative resection of a malignant neoplasm has not demonstrated a survival benefit in randomized controlled trials due to the variety and infrequency of malignant mediastinal tumors [2,3,12,15,16]. Overall, patients with benign schwannoma have excellent survival following complete resection, whereas those with malignant tumors have a poorer prognosis [2,3,5,22,23,24].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
