
Case Report | DOI: https://doi.org/10.31579/2641-0419/453
1Department of Cardiac An aesthesia Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
2Department of Cardiac Surgery, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
*Corresponding Author: Ajmer Singh, Director, Cardiac An aesthesia Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
Citation: Ajmer Singh, Ganesh Rasamalla, Ravina Mukati, Anil Bhan, (2025), Unroofing of Anomalous Right Coronary Artery: Interesting Images, J Clinical Cardiology and Cardiovascular Interventions, 8(3); DOI: 10.31579/2641-0419/453
Copyright: © 2025, Ajmer Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 February 2025 | Accepted: 21 February 2025 | Published: 28 February 2025
Keywords: anomalous right coronary artery; Malignant course; Unroofing; Multi-detector computed tomography
Anomalous origin of the coronary artery from the opposite sinus can potentially lead to life-threatening complications including myocardial infarction, arrhythmia, or sudden death. The interarterial course between the aortic root and pulmonary artery, the so-called malignant course, can cause compression of the artery; and can lead to adverse outcomes including death. The unroofing technique is suitable for those with intramural course, and it creates a new coronary ostium in the correct sinus of Valsalva. We describe a thirteen-year-old patient with an anomalous right coronary artery arising from the left sinus of Valsalva. The interarterial course of the right coronary artery was lying between the aorta and pulmonary artery. The patient underwent an unroofing of the right coronary artery and made an uneventful recovery.
Anomalous origin of the coronary artery from the opposite sinus can potentially lead to life-threatening complications including myocardial infarction, arrhythmia, or sudden death. The most common anomaly of this type is the anomalous origin of the left circumflex coronary artery from the right sinus, followed by the right coronary artery (RCA) from the left sinus of Valsalva, and the left main coronary artery from the right sinus of Valsalva.1 The interarterial course between the aortic root and pulmonary artery is the so-called malignant course and is most likely associated with an adverse outcome, including death. Surgery is recommended when the course of the anomalous artery is interarterial between the aortic root and the pulmonary artery. The type of surgical repair is influenced by the morphologic details, mainly the ostial status and intramural course. The unroofing procedure is a technique suitable for those with the intramural course, and it creates a new coronary ostium in the correct sinus of Valsalva, thereby eliminating the course between the pulmonary artery and aorta and the intramural course. An unroofing procedure obviates the need for coronary reimplantation, patch angioplasty, or coronary artery bypass grafting.
A thirteen-year-old girl presented to our institution with a history of angina on exertion (New York Heart Association functional class II-III) for the last six months. Two-dimensional echocardiography showed an anomalous origin of the RCA from the left sinus of Valsalva. This was confirmed on multi-detector computed tomography (MDCT), which showed RCA arising from the left sinus of Valsalva with a slit-like orifice and a significant intramural course (Figure1). The patient was scheduled for repair of the anomaly by unroofing the RCA.
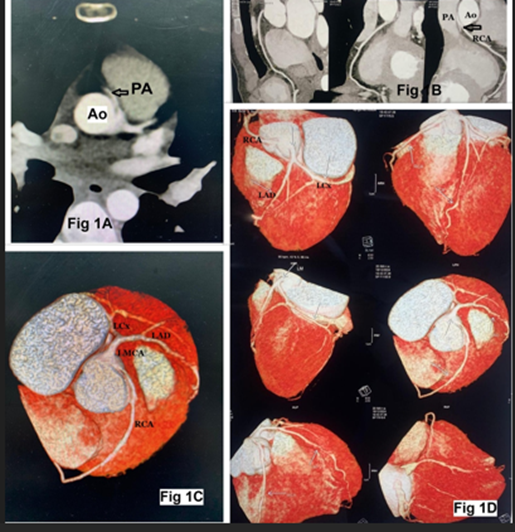
Figure 1: Multi-detector computed tomography (MDCT) showing an anomalous origin of the right coronary artery arising from the left sinus of Valsalva with an interarterial course (arrow, Fig 1A, 1B). Volume-rendering image showing the interarterial anomalous right coronary artery (RCA) arising from left sinus of Valsalva (Fig 1C, 1D). Ao: aorta, PA: pulmonary artery, LMCA: left main coronary artery, LAD: left anterior descending, LCx: left circumflex artery
Using standard anesthetic technique and standard monitoring, including transesophageal echocardiography (TEE), the surgical procedure was performed via median sternotomy. TEE images were consistent with MDCT images (Figure 2). Cardiopulmonary bypass (CPB) was instituted after aortocaval cannulation and cardioplegic arrest was achieved. Dissection began between the great arteries to identify the RCA as it exited from the aorta. An aortotomy was then performed just superior to the sinotubular junction and the orifice of the RCA arising from the left sinus of Valsalva was identified (Figure 3A). The right and left coronary commissures were detached to expose the intramural portion of the artery. A 2 mm coronary probe was inserted into the RCA and the length of the intramural segment of the RCA was assessed. An unroofing then began with the probe as a guide. The roof of the tunnel was excised up to the right coronary cusp, and stay sutures helped in providing the necessary traction for this (Figure 3B, 3C). Once this has been done, the intima of the aorta and the coronary artery were tacked together using interrupted 7-0 monofilament sutures. The final probe confirmed that the orifice was widely patent. The left and right coronary commissures were resuspended using 3 mm x 3 mm pledgeted sutures. The aortotomy was closed after checking the aortic valve for competence. The cross-clamp was released, and the RCA was inspected as it exited the aorta to make sure that there was no bleeding. The heart was de-aired, the aortic cross-clamp released, the heart resumed activity in sinus rhythm, and the patient was weaned off CPB. The duration of the aortic cross-clamp was 50 min and the duration of CPB was 58 min. Further course of the patient in the hospital was uneventful and she was discharged on postoperative day seven. At a six-week follow-up, the patient was asymptomatic and MDCT imaging confirmed that the coronary anomaly has been corrected (Figure 3D).
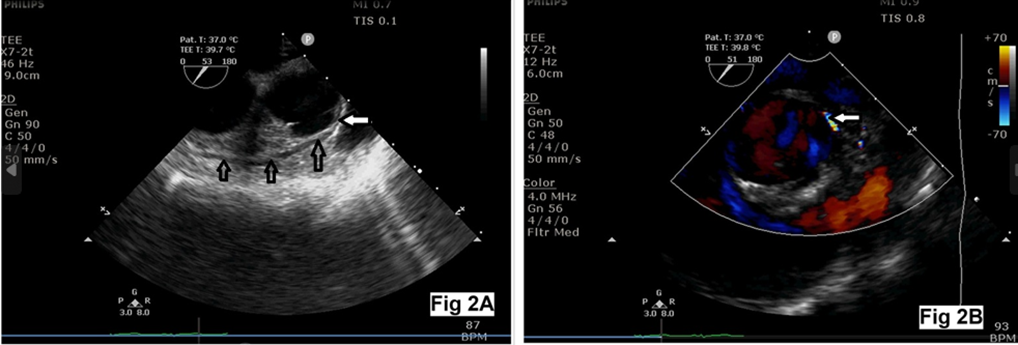
Figure 2: Two-dimensional echocardiographic aortic valve short-axis view showing anomalous right coronary artery arising from left sinus of Valsalva with an intramural course (arrows, Figure 2A). Color Doppler interrogation showing linear diastolic flow signal in the intramural segment (Figure 2B)
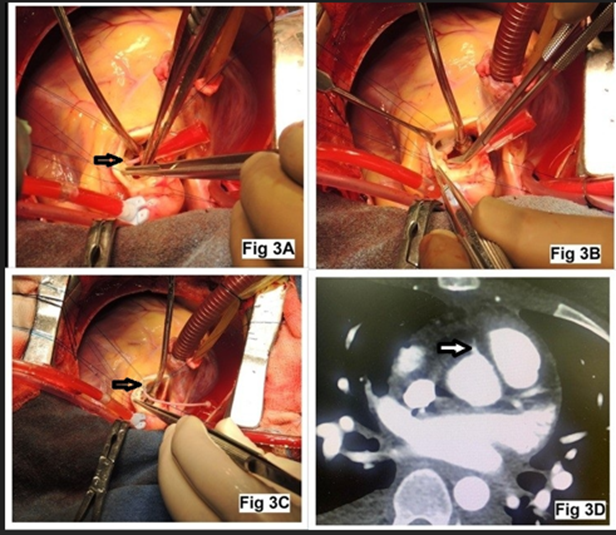
Figure 3: Surgical photographs showing anomalous origin of the right coronary artery (RCA) from the left sinus of Valsalva (probe in the RCA ostium, Figure 3A), unroofing of the RCA (Figure 3B), and RCA ostium in the correct sinus (Figure 3C). Multi-detector computed tomography showing origin of the RCA from the right sinus of Valsalva (arrow, Figure 3D)
The incidence of coronary arterial anomalies including the anomalous origin of the RCA in a normal heart ranges from 0.2% in patients undergoing echocardiography to 1.2% of patients at angiography.3 The anomalous left main coronary artery with an interarterial course is considered to be a high-risk lesion, and even without symptoms, surgical correction is recommended.4 Although a surgical correction is indicated in symptomatic anomalous RCA, the correction in asymptomatic patients remains controversial, but it is still a widely recommended operation. In patients with anomalous RCA anatomy and symptoms, such as the case described here, the surgery should not be delayed. Congenital coronary anomalies are the fifth most common cause of sudden cardiac death behind cardiomyopathies, acquired coronary artery disease, cardiac conduction disease, and myocarditis.5
Transthoracic echocardiography or TEE can be an effective and reliable tool in the accurate identification of these life-threatening coronary artery abnormalities. An assessment of coronary origins should be part of the standard imaging protocol for all echocardiographers with targeted views and focused color Doppler interrogation of the anterior aortic wall.6 MDCT provides an excellent two- and three-dimensional delineation of the anomalous coronary arterial origin and course. It also provides an excellent definition and spatial resolution of the unusual origin and intramural course of the coronary arteries, providing the information needed for the correct surgical procedure. Many surgical strategies have been suggested to treat this defect, including coronary reimplantation, patch angioplasty, unroofing the intramural segment, and coronary artery bypass grafting. The type of surgical repair is influenced by specific morphologic details, mainly the ostial status and the intramural course. The unroofing procedure, first described by Mustafa et al, is suitable for those with intramural course.7 This technique creates a new coronary ostium in the correct sinus, eliminates the course between the aorta and the pulmonary artery, and eliminates the intramural course. During the aortotomy, great care should be taken to prevent any inadvertent injuries to the anomalous coronary artery. The unroofing technique involves opening the slit-like ostium with fine scissors. The shared wall between the coronary artery and the aortic lumen is excised to the extent of its intramural course. Extreme care should be taken not to be too aggressive and cut beyond the shared wall to the outside of the aorta. If the intramural course is at or below the commissural attachments of the aortic valve, the commissure may require detachment and reattachment to the aortic wall at the appropriate level to prevent prolapse of the aortic leaflets and aortic insufficiency. An alternative procedure is the fenestration or limited unroofing which avoids the manipulation of the commissural attachment and the risk of aortic insufficiency.
The advantage of unroofing is that it relocates the functional orifice to the appropriate sinus and enlarges the orifice considerably. Also, it eliminates the intramural portion of the anomalous artery as well as the segment that lies between the great arteries. Potential pitfalls of the unroofing technique include aortic incompetence from damage to the commissures, aortic dissection if the layers are not tacked, and external bleeding if the unroofing has been overaggressive. Tacking together of the intimal layers of the aorta and the coronary artery helps avoid the risk of aortic dissection when the aortic root is pressurized. The postoperative MDCT imaging can confirm the new origin of the anomalous artery from the correct sinus of the Valsalva.
In conclusion, anomalous coronary artery anatomy is frequently characterized by an intramural course, which can be reliably identified by echocardiography, and confirmed by MDCT imaging. The intramural form can be repaired by unroofing the intramural segment without early morbidity or mortality.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
