
Research Article | DOI: https://doi.org/10.31579/2641-0419/209
*Corresponding Author: Ranjit Kumar Sharma, Department of Cardiology, Nepal Mediciti, Lalitpur 44600 Nepal
Citation: Ranjit Sharma, Anish Hirachan, Milan Gautam, Prabesh Neupane (2021) Unprotected Left Main is now no more Domain of Surgeon. J. Clinical Cardiology and Cardiovascular Interventions, 4(14); Doi:10.31579/2641-0419/209
Copyright: © 2021 Ranjit Kumar Sharma, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2021 | Accepted: 16 August 2021 | Published: 20 August 2021
Keywords: coronary artery; coronary artery bypass surgery; left circumflex
Unprotected Left Main Coronary Artery (ULMCA) disease is defined as significant stenosis in the Left Main Coronary Artery (LMCA) and there were no previous Coronary artery bypass surgery (CABG) or patent bypass grafts to the left anterior descending (LAD) or left circumflex (LCX) arteries
Unprotected Left Main Coronary Artery (ULMCA) disease is defined as significant stenosis in the Left Main Coronary Artery (LMCA) and there were no previous Coronary artery bypass surgery (CABG) or patent bypass grafts to the left anterior descending (LAD) or left circumflex (LCX) arteries [1]. It is associated with high mortality as it supplies a large area of the myocardium—approximately 84% of the left ventricle in the right dominant system and 100% in a left dominant system [2]. ULMCA disease constitutes 5 to 7% of the patients undergoing coronary angiography [3]. The LMCA disease (i.e., > 50% stenosis) was found in 1477 (7.3%) of 20 137 patients in the Coronary Artery Surgery Study (CASS) registry [4]. Significant LMCA stenosis is defined as a >50% diameter stenosis, and the left main equivalent disease is defined as severe (70%) diameter stenosis of the proximal LAD and proximal left circumflex as judged by contrast angiography [5].
The left main coronary artery (LMCA) usually arises from the left coronary sinus, It passes between the pulmonary trunk and the left atrial appendage and just under the appendage in 70% of individuals bifurcates into the left anterior descending artery and left circumflex artery, and 30% trifurcates into an additional ramus intermedius [6]. An anomalous take-off from or above the right sinus of Valsalva represents a relatively common anatomic variant. Notably, the rare (estimated prevalence 0.03%) LM with an anomalous origin from the right coronary sinus and "intra-arterial" course between the aorta and pulmonary artery is associated with the risk of sudden death [7].
The LMCA contains a higher elastic tissue component compared to the rest of the coronary tree which can explain elastic recoil and high restenosis rate following balloon angioplasty. The ostium of the LMCA lacks the tunica adventitia and is richer in smooth muscle cells and elastic tissue than any other portion of the LMCA and its branches [8]. The LM is a large diameter artery with important variability across different individuals. The mean "reference" diameter, derived from a large intravascular ultrasound (IVUS) study is 5 mm and ranges between 3.5 and 6.5 mm with a mean length of 10.5±5.3 mm [9]. Usually, the short ostium is associated with the bicuspid aortic valve [10]. When considering the side branch relevance according to the amount of myocardium supplied, the left main bifurcation is known to have its major side branch (i.e., the LCX) supplying >10% of the myocardial mass in more than 95% of cases [11].
The left main disease most commonly occurs due to atherosclerosis, whereas other less common causes include vasospasm, arteritis, radiation, extrinsic compression [12]. LM disease is categorized into “ostial”, “mid-shaft” or “distal” based on angiography [13]. The distribution of LMCA lesions is approximately 10% ostial, predominantly occurring in young women, about 70% in the distal left main artery, and the remainder 20% in the shaft. In >80% of the cases, it is associated with multivessel involvement [14].
In up to 40% of patients, LM disease is associated with significant carotid artery stenosis [15]. In a study by Oviedo, it was found that continuous plaque from the LMCA into
the proximal LAD artery was seen in 90%, from the LMCA into the LCX artery in 66.4%, and from the LMCA into both the LAD and LCX arteries in 62%. Plaque localized to either LAD or LCX ostium and not involving distal LMCA was seen in only 9.3% of LAD arteries and 17.1% of LCX arteries [16]. When the LM bifurcation is diseased, intimal atherosclerosis is accelerated primarily in the area of low shear stress in the lateral wall close to the LAD and Lacs bifurcation and the carena is frequently free of disease [17].
Trial Evidence for LM Stenting
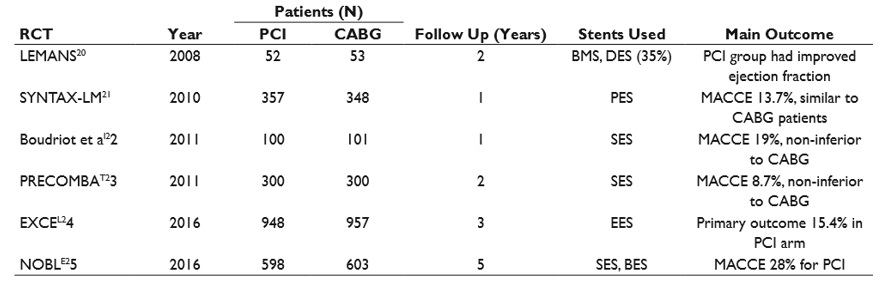
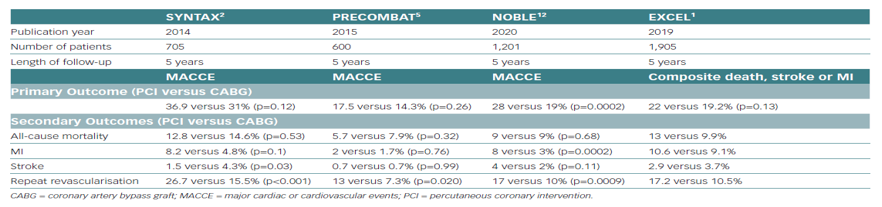
The SYNTAX trial included a subset of 705 patients with LM disease. There was no significant difference in MACCE (death, MI, stroke, and repeat revascularization) at 5 years (36.9% in PCI patients and 31% in CABG patients) (HR 1.23; 95% CI: 0.95–1.59; p = 0.12).
Mortality was 12.8 and 14.6% in PCI and CABG patients, respectively (HR 0.88 [0.58, 1.32]; p = 0.53). Stroke was significantly increased in the CABG group and repeat revascularization in the PCI arm. MACCE was similar between arms in patients with low/intermediate SYNTAX scores but significantly increased in PCI patients with high scores (≥ 33) [24].
In the EXCEL (Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) trial, 1,905 patients—with ULMCA disease with ≥ 70% diameter
stenosis, or ≥ 50% or ≤ 70% with either (1) noninvasive evidence of LM ischemia, (2) intravascular ultrasound-derived minimal lumen area (IVUS-MLA) ≤ 6.0 mm2, or (3) fractional flow reserve (FFR) ≤ 0.80, SYNTAX score ≤ 32, and clinical and anatomic eligibility for both PCI and CABG as agreed to by the local heart team—were randomized to PCI with fluoropolymer-based cobalt-chromium everolimus-eluting stents or CABG. The primary endpoint, the composite of death from any cause, stroke, or MI at 3 years occurred in 15.4% of patients who underwent PCI group versus 14.7% of the patients who underwent CABG group meeting the noninferiority criterion. The secondary endpoint event of death, stroke, or MI at 30 days was lower in the PCI group (4.9% in the PCI group vs. 7.9% in the CABG group). The secondary endpoint event of death, stroke, MI, or ischemia-driven revascularization at 3 years occurred in fewer patients in the PCI group. CABG patients had fewer primary endpoint events than the PCI group patients between 30 days and 3 years after the procedure. Revascularization rates at 3
Years were higher with PCI than with CABG (12.6 vs. 7.5%) whereas the rates of early MI and major adverse events were lower with PCI than with CABG (8.1 vs. 23.0%) [25].
The EXCEL trial enrolled predominantly males (76%). Most patients were clinically at low risk (60% had stable ischemic heart disease and most patients had normal ejection fraction). Thirty percent were diabetic. According to the sites, the SYNTAX was low (≤ 22) in 60.5% of the patients and intermediate (23–32) in 39.5% of the patients. The core laboratory assigned higher scores, low in 35.8% of the patients, intermediate in 40.0%, and high (≥ 33) in 24.2%, the group that met the exclusion criteria. Most of the patients (80.5%) had distal left main bifurcation or trifurcation disease, and two- or three-vessel coronary artery disease was present in 51.3% of the patients. Average 1.9 lesions were treated per patient. A mean of 2.4 stents with a mean total stent length of 49.1 mm was implanted per patient. Femoral access was used in 73% of patients, and IVUS guidance was used in 77% of patients. Off-pump CABG was performed in 29%. Internal mammary artery (IMA) was used in 98.8% with bilateral IMA in 28.8% of patients.
NOBLE (Nordic-Baltic-British Left Main Revascularization Study) trial11 randomized patients with significant LM lesion visually assessed stenosis diameter ≥ 50% or FFR ≤ 0.80 and no more than three additional non-complex lesions (additional non-LM complex lesions were chronic total occlusions, bifurcation lesions requiring two-stent strategies, calcified or tortuous lesions). A total of 1,201 patients were randomly assigned to PCI or CABG. Kaplan-Meier 5-year estimates of MACCE (death from any cause, nonprocedural MI, repeat revascularization, or stroke) were 29% for PCI and 19% for CABG (HR 1.48; 95% CI: 1.11–1.96) with CABG being significantly better than PCI. Though all-cause mortality was not different, the rates of MI, revascularization and stroke were higher in PCI patients compared with CABG patients. Repeat revascularization was higher due to de novo lesion and target non-LMCA lesion revascularization. Notably, 1-year MACCE was the same in both groups. Surprisingly there was no association between the SYNTAX score and MACCE. Twenty percent of the population was female with 15% diabetics. Eighty percent had stable angina and most had preserved ejection fraction. Eighty-eight percent had distal LM lesions. Elective double stenting was used in 35% with culotte being the preferred technique. 11% of PCI cases received the first-generation DES in the LM. Kissing balloon inflation (KBI) was done in 55%, and any ostial circumflex post-dilatation was done in 79%. Complete revascularization was achieved in 92%. IVUS was done pre-PCI in 47% and post-PCI in 74%. CABG was done with the on-pump technique in 84%, with 93% of patients receiving left internal mammary artery. The number of grafts per patient was one in 4%, two in 52%, three in 39%, four in 4%, and five in < 1>
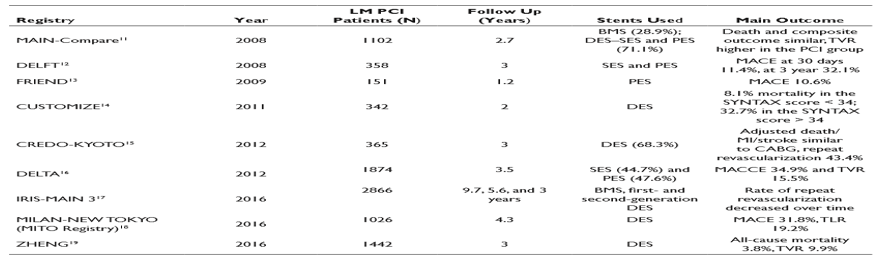
At present, combined data from the above six trials of 2355 patients randomized to LM PCI and 2362 patients randomized to CABG suggest non-inferiority of PCI about survival. However, higher repeat revascularizations in the PCI group remain a concern when compared to CABG. It may be concluded that PCI works best for Ostial and shaft lesions and in patients with SYNTAX score < 33> 33, CABG may be preferred although an individualized approach may be prudent [27].
1. Differences between studies in patient assessment, risk profiles, trial process, or procedural characteristics.
2. Differences in the stent used: EXCEL used a thin strut fluoropolymer-based cobalt-chromium everolimus-eluting stents whereas NOBLE used first-generation sirolimus-eluting Cypher stent (11%) or the biolimus-eluting Biomatrix Flex stent (89%), resulting in a substantial difference in-stent thrombosis (0.7 vs. 3%). As a result, the rate of stent thrombosis or symptomatic graft occlusion was much higher after CABG than after PCI (5.4 vs. 0.7%) in EXCEL but similar (4 vs. 3%) in NOBLE.
3. Strategy of stenting: Both trials used a provisional stenting approach. In approximately 75% of patients, IVUS was used. Data were not available from EXCEL regarding the two-stent strategy. Thirty-five percent needed a two-stent strategy with the culotte technique being used in the majority in NOBLE.
4. Differences in primary endpoint used: EXCEL used death, MI, and stroke. Investigators included periprocedural MI. The EXCEL trial did not include repeat revascularization. The NOBLE trial, on the other hand, used only nonprocedural MI in the endpoint, and repeat revascularization was part of the primary composite endpoint. In the NOBLE trial, there was not much difference in target LM artery revascularization but more than a twofold increase in de novo lesion revascularization in the PCI group with most patients undergoing repeat PCI (96%). 5. Difference in trial duration: EXCEL reported data at 3 years whereas NOBLE reported data at 5 years. Remarkably in NOBLE, the 5-year mortality was not different in PCI and CABG groups whereas death, stroke, and repeat revascularization was higher in the PCI group. Data from EXCEL may look similar to NOBLE if repeat revascularization is included with an evaluation done at 5 years.
6. An unexplained higher risk of stroke after PCI in NOBLE, which was more than twice after PCI than CABG.
Although opposing findings may have an uncertainty on the optimal revascularization strategy, these trials also demonstrated how much PCI has been improved for LMCA treatment.
Technical Considerations in LM Stenting
When performing LMCA interventions, the following technical considerations are important.
1. Patient comorbidities: Elderly age, diabetes, renal failure, acute coronary syndrome on presentation, left ventricular dysfunction, concomitant valvular disease, previous cerebrovascular events, and so on.
2. Lesion morphology: Lesion location—Ostial, shaft, or bifurcation, presence of calcification, angulation, smaller LMCA diameter < 3> 70% and lesion length > 10 mm or if it satisfies two of the following six minor criteria: (1) moderate to severe calcification; (2) multiple lesions; (3) LAD-LCX bifurcation angle > 70 degrees; (4) main vessel reference vessel diameter < 2> 25 mm.
3. Use of additional equipment: To optimize and safely accomplish the LMCA intervention, consideration must be given to the use of additional equipment such as intravascular imaging, physiologic assessment, mechanical circulatory support, and ventilatory support.
Role of Coronary Imaging for LM Stenting
The results from the multicenter LITRO study indicated that LMCA intervention may be safely deferred if the minimal lumen area by IVUS is > 6 mm2. In this study comprising of 354 patients, LMCA intervention was deferred in 179 of 186 patients and undertaken 152 of 168 patients based on the minimal lumen area cut-off value of 6 mm2. During a 2-year follow-up, no difference was observed in cardiac death or events [28]. It is important to perform IVUS pull back from LAD and LCX into LMCA to assess the plaque burden at the Ostia of these branches and also to disengage the guide catheter to assess the plaque burden at LM ostium. An MLA < 3> 56% in the LCX ostium is a predictor of the need for a second stent after provisional stenting of the main vessel and LM ostium should be stented if the plaque burden is > 50% at the ostium [29]. Further IVUS also helps to assess the degree and depth of calcification and guides to decide for debulking strategy such as rotablation. Poststent IVUS run will help to detect stent under expansion and mal apposition Poststent minimal stent area to predict angiographic restenosis. The best IVUS criteria of minimal stent area predicting angiographic restenosis were 5.0 mm2 for the left circumflex artery ostium, 6.3 mm2 for the LAD ostium, 7.2 mm2 for the polygon of confluence, and 8.2 mm2 for the proximal LMCA above the polygon of confluence (so-called 5-6-7-8 rule of criteria) [30].
Optical coherence tomography (OCT) is the newer imaging modality with higher resolution and faster pull-back speed to assess the intravascular characteristics of the vessel and plaque. OCT is especially useful to identify stents under expansion and malposition with more precision compared to IVUS. Although at present no guideline recommendations are available for OCT-derived LM for intervention [31].
Strategies for LM Stenting
Ostial and shaft lesions may be easily carried out by appropriately sized stents and optimizing the result with post-dilation using a non-compliant balloon. When treating ostial LM lesions one or two struts should be positioned into the aorta and adequate dilatation should be done without causing dissection of the aorta.
Distal LM lesions may be treated by several approaches:
1. Cross-over strategy: Stent placement across LM into either LAD or LCX and optimizing the LM stent. In the LMCA bifurcation, intimal atherosclerosis is accelerated primarily in the area of low shear stress in the lateral wall close to the LAD and LCx bifurcation. Thus, the carena is frequently free of disease and this can explain the reason why the single-stent strategy can be successfully performed in patients with no or moderate disease by angiography.
2. Provisional stenting strategy: In this strategy, most commonly LM–LAD stent is done with a wire protecting the LCX. If there is a significant compromise of LCX or associated with angina or hemodynamic changes, bail-out stenting of LCX may be carried out using T and small protrusion (TAP) or culotte techniques. Before LM stenting, IVUS is helpful to decide in favor of provisional stent strategy. If the IVUS-derived minimal lumen is > 3.7 mm2 or plaque burden is < 56>
3. Two stent strategy: This strategy may be considered if the LCX is a dominant vessel if LCX ostium has a significant disease, LCX diameter > 2.5 mm, or the angle between LAD and LCX is narrow. Preferred techniques in this situation include T-or TAP-stenting, culotte, and mini-crush or double kissing (DK) crush techniques. If the LCX is smaller than LAD with a bifurcation angle > 70%, DK crush is ideal, and if it is < 70>
Mechanical Circulatory Support
IABP is the most commonly available device with easy and expeditious insertion but is associated with low efficacy to augment cardiac output. It may be useful in pre-shock/shock patients, electively, or during emergency crash situations during LM PCI. Impella provides a higher cardiac output and may be considered in high-risk LM PCI or during severe shock. Tandem heart and ECMO are mainly useful for cardiac arrest situations. It is very important to plan the device strategy before the commencement of LM intervention [35].
Percutaneous intervention with stent implantation for LMCA disease has become a standard procedure in contemporary practice with safety, expedited recovery, and durability. Precise selection of the strategy aided by intracoronary imaging, functional evaluation, and mechanical support when needed has improved the immediate and long-term results in this high-risk intervention. It is however important to have a team approach and operator expertise before embarking on LMCA interventions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
