
Case Report | DOI: https://doi.org/10.31579/2641-0419/303
Department of Cardiology, Arrazi Hospital, Mohammed VI University Hospital, Marrakesh, Morocco
*Corresponding Author: Zakaria Wakrim, Department of Cardiology, Arrazi Hospital, Mohammed VI University Hospital, Marrakesh, Morocco
Citation: Zakaria Wakrim, Mohammed El Jamili, Mustapha El Hattaoui (2023), Unkind Reminder: Never Pretreat Nstemi Patients Until Their Anatomy is Known, J. Clinical Cardiology and Cardiovascular Interventions, 6(3); DOI:10.31579/2641-0419/303
Copyright: © 2023 Zakaria Wakrim, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 January 2023 | Accepted: 20 March 2023 | Published: 04 April 2023
Keywords: aortic dissection; pretreatment; chest pain; non-ST-elevation acute coronary syndrome
This case report describes the presentation and management of a 71-year-old male patient with sudden onset of chest pain. Despite an initial diagnosis of acute myocardial infarction (AMI) and pre-treatment with clopidogrel, further evaluation revealed the patient to have acute aortic dissection. The patient's condition rapidly deteriorated and ultimately led to his death.
This case highlights the importance of careful diagnostic consideration when presented with symptoms of chest pain, particularly in high-risk patients, and the potential consequences of routine pre-treatment with P2Y12 inhibitors in such cases.
Acute aortic dissection (AAD) is a rare but life-threatening condition that requires prompt diagnosis and management [1]. The presentation of AAD can be nonspecific, and the differential diagnosis includes other causes of chest pain, such as acute myocardial infarction (AMI). This case report describes the presentation and management of a 71-year-old male patient with hypertension who presented to a community health center with sudden onset of chest pain radiating to the back. The patient was initially diagnosed with AMI but was later found to have AAD, culminating in his death. This case highlights the importance of considering AAD in the differential diagnosis of chest pain and the challenges in managing this condition in the setting of prior antiplatelet therapy.
Case Description
A 71-year-old male tailor presented to a community health center with sudden onset of ‘ripping’ chest pain radiating to the back. The patient had a known history of hypertension, which had not been effectively managed with medication, and no significant past medical history or family history of cardiovascular disease. Vital signs were within normal limits, but an electrocardiogram (ECG) revealed ST-depression and inverted T waves in leads V5, V6, D1, and aVL, and high-sensitivity troponin levels were elevated. The patient was initially diagnosed with acute myocardial infarction (AMI) without ST segment elevation (NSTEMI) and received a full-loading dose of clopidogrel, aspirin, and heparin. He was then transferred to a tertiary care hospital for further evaluation and management.
On examination in the emergency department, the patient complained of severe pain, sweating, and nausea. Systolic blood pressure asymmetry was observed, with a reading of 90/54 mmHg in the right arm and a pulse deficit compared to a reading of 142/59 mmHg in the left arm. No focal neurologic deficit or signs of heart failure or limb ischemia were noted. Repeat ECG showed no new changes, but transthoracic echocardiography (TTE) revealed an enlarged aorta with an intimal flap that did not affect the origins of the coronary arteries. Additionally, mild aortic regurgitation was observed. The left ventricular function and dimensions were within normal limits, however, a small slide of pericardial effusion was also identified. (Figures A)

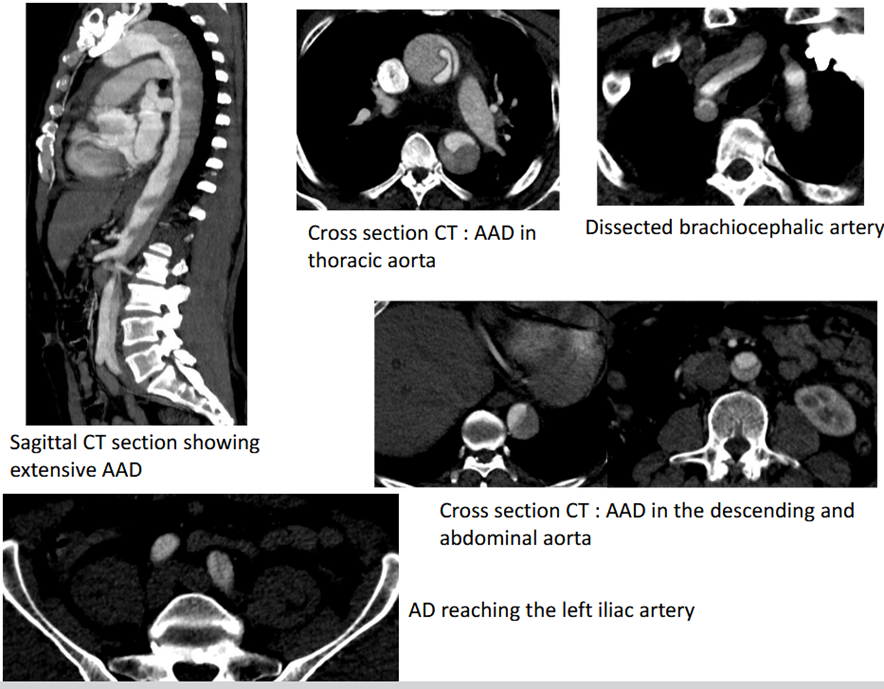
In light of these findings, an urgent computed tomography (CT) scan was performed, which definitively confirmed the diagnosis of acute aortic dissection (AAD). It revealed that the dissection was originating beyond the sinuses of Valsalva, ascending to the brachiocephalic artery, and dissecting along the thoracic and abdominal aorta, ultimately reaching the left iliac artery. (Figures B)
The patient was given intravenous beta-blockers, but his condition was too complex for urgent surgical intervention to be performed, especially with the prior administration of clopidogrel. Unfortunately, the patient's condition continued to deteriorate resulting in his demise the following morning.
Discussion
The present case report highlights the potential for diagnostic confusion between acute aortic dissection and acute myocardial infarction and the subsequent administration of P2Y12 inhibitors.
Among patients presenting with acute chest pain in emergency departments, the prevalence of myocardial infarction MI is typically around 30%[2]. Other conditions, such as AAD, myocarditis, and pulmonary embolism, can also cause elevated cardiac troponin levels and should be taken into account as potential diagnoses for patients experiencing acute chest pain[2].
A patient's medical history serves as a crucial foundation for identifying the potential causes of cardiac symptoms. However, underlying causes may manifest differently in each individual, thus additional information beyond the patient's history may be necessary to make a definitive diagnosis. Sudden onset of severe, ‘tearing’ or ‘ripping’ chest pain, particularly in individuals with hypertension or preexisting conditions such as a bicuspid aortic valve or aortic dilatation, should raise suspicion for the presence of an acute aortic syndrome, such as AAD[3].
Despite the activation of blood platelets and the coagulation cascade playing a key role in the initial phase and evolution of NSTE-ACS, there is a lack of large-scale randomized trials supporting an upfront pre-treatment strategy of P2Y12 receptor inhibitors such as clopidogrel in NSTE-ACS patients. The Downstream Versus Upstream Strategy for the Administration of P2Y12 Receptor Blockers In Non-ST Elevated Acute Coronary Syndromes With Initial Invasive Indication [DUBIUS] trial[4] was aborted prematurely because of the unlikelihood of increased efficacy of one strategy over the other.
The ACCOAST[5] trial compared the use of prasugrel as a pretreatment at the time of diagnosis in patients with NSTE-ACS to administering it selectively after angiography in patients undergoing PCI. 4033 patients were included, with those in the pretreatment group receiving a loading dose of prasugrel before angiography and additional 30 mg at the time of PCI, while the control group received 60 mg of prasugrel at the time of PCI. Results showed that pretreatment with prasugrel did not reduce the rate of major ischemic events but increased the rate of major bleeding complications[5,6].
The utilization of P2Y12 receptor inhibitors as a routine pre-treatment strategy for patients presenting with chest pain and meeting the criteria for non-ST-elevation acute coronary syndrome (NSTE ACS) may be detrimental for a considerable proportion of individuals who are subsequently diagnosed with conditions other than type 1 myocardial infarction, such as aortic dissection, tension-pneumothorax, or stroke. The administration of these inhibitors may increase the risk of bleeding complications or delay surgical procedures for patients scheduled for surgery[2]. However, the recommended standard therapy with potent P2Y12 receptor inhibitors has a rapid onset of action and allows for administration of LD after diagnostic coronary angiography and directly before PCI. Therefore, as per the guidelines of the European Society of Cardiology[2], echocardiography is recommended as a means of evaluating left ventricular function and ruling out differential diagnoses (COR: I; LOE: C) and routine pre-treatment with a P2Y12 receptor inhibitor in patients with NSTE ACS whose coronary anatomy is unknown and for whom early invasive management is planned is not recommended because of the lack of established benefit (COR: III, LOE: A).
Acute aortic syndromes (AAS) are a group of life-threatening conditions characterized by a breach in the integrity of the aortic wall, which can lead to rupture if left untreated. The most common forms of AAS include aortic dissection, intramural hematoma, and penetrating atherosclerotic ulcer [1].
Aortic dissection specifically is defined as a disruption of the media layer of the aorta caused by intramural bleeding [7], resulting in the separation of the layers of the aortic wall and the formation of a dissection flap that divides the true lumen from a newly formed false lumen [1]. The incidence of AD is higher in men than in women and increases with age[8]. Historically, “acute” aortic dissection (AAD) has been defined as occurring within the first two weeks of symptom onset. The most common risk factor associated with AAD is hypertension, present in 65-75% of individuals[9], often poorly controlled like in the case of this patient. Other risk factors for AAD include preexisting aortic or aortic valve disease, a family history of aortic disease, a history of cardiac surgery, smoking, direct chest trauma, and connective tissue disease. Drug use, particularly cocaine, can cause dissection even in the absence of other risk factors[3].
Transthoracic echocardiography (TTE) is a non-invasive imaging technique that can be utilized to differentiate the various causes of acute chest pain, including acute aortic dissection [3]. Computed tomography (CT) is the most commonly used imaging technique for the evaluation of AAS[9,10]. The diagnostic accuracy of CT in detecting AAD involving the thoracic aorta is exceptional; the 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease recommends CT as the initial diagnostic imaging tool in patients with suspected AAS, due to its high availability, accuracy, and speed, as well as the level of anatomic detail it provides (COR :1; LOE: C-LD)[1].
The failure to promptly diagnose acute aortic dissection, in this case, may have been due to several potential contributing factors. One of which is the lack of measurement of blood pressure in both arms during the initial presentation, which could have led to an underestimation of the patient's clinical condition. Additionally, it is possible that the community healthcare staff may have been inadequately informed about the signs and symptoms of AAD or the differences in pre-treatment of STEMI and NSTEMI with P2Y12 inhibitors. Furthermore, the examination may have been normal upon admission, and the AAD may have been evolving and ascending, making it challenging to diagnose.
Prompt surgery is the treatment of choice for acute aortic dissection [1,7]. According to the International Registry of Acute Aortic Dissection, mortality in patients with surgical treatment delayed beyond 24 hours was 17.1%[11]. Untreated acute aortic dissection of the ascending aorta is associated with a high mortality rate, particularly in the early stages of symptoms, with a mortality rate of 1-2% per hour after symptom onset.[12]. It should be noted that this rate is likely to be even greater in patients who have extensive aortic dissection and are already receiving a loading dose of anticoagulant and dual antiplatelet therapy.
Despite the possibility of performing cardiothoracic surgery while under the effect of clopidogrel, the heart team in this case felt that their technical expertise and resources were not adequate to handle such a complicated procedure. Additionally, there is currently no available way to reverse the effects of clopidogrel. Due to the patient's extensive acute aortic dissection and the fact that he was not in hemodynamic distress, a more cautious approach was taken. However, this approach proved to be ineffective.
The current case report underscores the necessity for a comprehensive evaluation of diagnostic possibilities in patients presenting with chest pain, as well as the potential hazards of utilizing P2Y12 inhibitors as a pre-treatment option in patients with NSTE-ACS whose coronary anatomy remains undetermined. Additionally, it serves as a reminder of the importance of maintaining an appropriate level of training and resources to efficiently manage complex cases in the future.
Conclusion:
Acute aortic dissection is a rare but life-threatening condition that can mimic symptoms of myocardial infarction. This case illustrates the importance of considering alternative diagnoses in patients presenting with chest pain, particularly in those with known hypertension and a history of smoking. It also highlights the potential consequences of routine pre-treating patients with NSTEMI with P2Y12 inhibitors without a definitive diagnosis of type 1-MI. The prompt recognition of AAD is crucial for the appropriate management and to improve the chances of survival.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
