
Short Communication | DOI: https://doi.org/10.31579/2690-4861/393
1 Departments of Diagnostic Pathology, Tottori Prefectural Kousei Hospital, Kurayoshi-city, 682-0804 Tottori, Japan.
2 Thoracic Surgery, Tottori Prefectural Kousei Hospital, Kurayoshi-city, 682-0804 Tottori, Japan.
3 Medical Central Laboratory, Tottori Prefectural Kousei Hospital, Kurayoshi-city, 682-0804 Tottori, Japan.
*Corresponding Author: Yuji Ohtsuki MD, PhD., Department of Diagnostic Pathology,Tottori Prefectural Kousei Hospital, Kurayoshi, Tottori 682-0804, Japan.
Citation: Ohtsuki Yuji, Fukino Shunsuke, Irie Aiko, Tatsushima Junji, Nagao Mizuho, et al, (2024), Unique Distribution of Minute Meningothelioid Nodules at The Alveolar Mouths of Peripheral Airways within the identical lung harboring Adenocarcinoma, International Journal of Clinical Case Reports and Reviews, 16(3); DOI:10.31579/2690-4861/393
Copyright: © 2024, Yuji Ohtsuki. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 January 2024 | Accepted: 13 February 2024 | Published: 17 February 2024
Keywords: .
.
Minute meningothelioid nodules (MMNs) are not rare lesions in the lungs; however, their specific origin and functions remain unknown [1]. In a previous study, among 81 cases of resected lungs, MMNs were detected in 69 out of 500 surgical biopsies (13.8%) and 12 out of 25 lobectomies (48%) via detailed histochemical examination, with a female predominance at an average age of 62, and only 4 out of 81 cases involved patients younger than 40 years [1]. These findings indicate that MMNs are not congenital in origin [1]. In another report, MMNs were detected in 121 out of 1724 resected lungs (7%) via pathologic examination, with a female predominance [2].
Here, we investigated a pulmonary adenocarcinoma case with unique distribution of MMNs at the alveolar mouths (AMs) of lungs. To the best of our knowledge, such a case has not yet been described even in a report on more than 100 cases of MMNs [2]. Moreover, this report is the first to demonstrate the distribution of MMNs at the AMs of lung peripheral airways.
A lung tumor (size: 1.6 × 1.6 × 1.3 cm) was detected on the lower right lobe of the lungs in a mid-seventieth female with computed tomography (CT), followed by thoracoscopic lobectomy.
Histopathological diagnosis was pulmonary papillary adenocarcinoma with MMNs in vicinity. Many eosinophilic intranuclear bodies were observed in the cancer cells (Figure. 1A), which were immunohistochemically positive for the surfactant protein A(SP-A) (Figure. 1B).
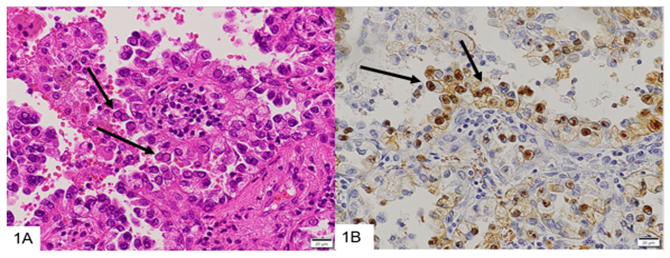
Figure 1: Eosinophilic intranuclear inclusions are found in the tumor cells (1A, arrows), and these inclusions are positive with SP-A antibody with immunohistochemical stain (1B, arrows).
We were interested in the unique microscopic distribution of proliferating meningothelioid cells at the AMs, as shown in Figure. 2A. Meningothelioid cells proliferate in a nest-like or whirl arrangement along the peripheral airways, including the alveolar duct and AMs, and their cell borders are obscure. Here, meningothelioid cells proliferated at the AMs as minute discontinuous nodules (Figure. 2B). The nuclei were small and positive for the progesterone receptor (PGR) (Figure. 2C), vimentin, and epithelial membrane antigen (EMA) (Figure. 2D), but not for neuroendocrine markers. They were morphologically, light microscopically [3], immunohistochemically [4], and ultrastructurally [5] similar to meningothelial cells. Notably, the cells were positive for somatostatin receptor (SSTR)-2a and -5 (Figure. 2E) and immunopositive for antibodies against vimentin and CD56 (N-CAM) but negative for synaptophysin, chromogranin, S100, cytokeratin, and transcription termination factor (TTF)-1 (Figure. 2F), suggesting that proliferating meningothelioid cells are not neuroendocrine in origin but exhibit meningothelial cell differentiation [3,4]. In sharp contrast to TTF-1-positive type II alveolar cells, the proliferating cell nuclei of MMNs were TTF-1-negative. This distribution of MMNs may be due to a function of the chemoreceptors [6,7]. As shown in Figure. 1B, PGR-positive nuclei of MMNs were located at the AMs as isolated discontinuous minute nodules in the stroma. PGR-positivity may be a factor controlling the growth of MMNs [8]. Both SSTR2a and NF2 may be involved in the proliferation, progression, and growth of MMNs [4].

Figure 2: MMN cells are located in the AMs (Fig. 2A, 2B, arrows), positive for PGR(2C, arrows), EMA(2D,arrows),SSTR-5(2E,arrows), but negative for TTF-1(2F,arrows) besides positive original type II alveolar cells in 2F(arrowheads)To date, no studies have indicated the presence of MMNs at the AMs as demonstrated in this report. AMs are important for alveolar epithelial cells and very unstable in response to any kind of microstimulus. AMs are considered as locus minoris resistentiae in the peripheral airways of the lungs. Masson bodies [9] and hyaline membranes [10] arise from the AMs and are induced by internal and external stimuli. In addition to being positive for SSTR-2a and -5, their location at the AMs may aid MMNs in playing key roles as chemoreceptors.
Meningothelioid cells are predominantly monoclonal in growth [11] and exhibit an NF2 deletion [3], which is a common mutation in meningiomas of the central nervous system F(3). Moreover, MMNs constitutively express SSTR2a [4]. Here, proliferating cells and MMNs were positive for SSTR-2a and -5.
MMNs may arise due to ischemic or reactive changes rather than neoplastic changes [8,11]. Moreover, MMNs may be transitional forms between reactive and neoplastic forms [12,13]. Although the exact origin of MMNs, even in the cell lineage, remains unclear, they are often detected in the vicinity of lung cancer [2,8], as observed in the present case.
MMN distribution at the AMs, as demonstrated in this report, is unique and rare. Although the specific functions and origin of MMNs remain ambiguous, they may arise due to ischemic or preneoplastic changes [13].
To the best of our knowledge, this report is the first to show the unique distribution of MMNs immunopositive for SSTR-2a and -5 at the peripheral airways of human lungs. These receptors are involved in cell secretion and proliferation [4].
Therefore, immunopositivity for SSTR-2a and -5 should be considered in addition to meningothelial cell differentiation when determining the functions of MMNs.
The author(s) declare(s)that there is no conflict of interest regarding the publication of this paper.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
