
Case Report | DOI: https://doi.org/10.31579/2690-8808/164
Division of Internal Medicine and Cardiovascular Medicine, Larkin Palm Spring Community Hospital, Hialeah, Florida
*Corresponding Author: Sabas Gomez, Division of Internal Medicine and Cardiovascular Medicine, Larkin Palm Spring Community Hospital, 1475 W 49th Pl, Hialeah, FL 33012
Citation: Hudson Franca, Sergio A. Sanchez, Sahar S. Abdelmoneim, Abelardo Broceta Martinez, Sabas Gomez, et all (2023) Unique Approach to Management of Hypertrophic Obstructive Cardiomyopathy within a Resource-Limited Hospital. J, Clinical Case Reports and Studies, 4(2); DOI:10.31579/2690-8808/164
Copyright: © 2023 Sabas Gomez, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 November 2022 | Accepted: 30 December 2022 | Published: 06 February 2023
Keywords: hypertrophic obstructive cardiomyopathy; pure α-agonist; phenylephrine
LVOT obstruction in HCM results from systolic anterior motion (SAM) of the anterior leaflet of the mitral valve and is often a dynamic process (increasing with volume depletion and decreases with volume repletion or afterload augmentation). Hence, understanding the underlying pathophysiological process is crucial in tailoring management decisions.
We herein present a case of a 57-year-old female who presented to the emergency department with complaints of shortness of breath (SOB), cough and borderline blood pressure who further decompensated during hospital course, suffering from acute hypotension related to dynamic LVOT obstruction. The patient was managed with a pure α-agonist, phenylephrine.
This case report highlights the importance of having a high index of suspicion to early recognize such dynamic LVOT obstruction and further highlights the uniqueness of managing symptomatic hypotension in HCM with LVOT obstruction in an under-resourced hospital.
Hypertrophic cardiomyopathy (HCM) is a genetic cardiomyopathy caused by mutations of the cardiac sarcomere, with respect to the extent, location, and distribution of left ventricle (LV) wall thickening as well as a diverse clinical course including sudden death, heart failure, and stroke (1). Patients with LV outflow tract (LVOT) obstruction may have a harsh crescendo-decrescendo systolic murmur. Symptoms associated with HOCM include dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, chest pain, palpitations, presyncope/syncope, postural lightheadedness, fatigue, or edema [1].
Challenging management decisions for patients with HCM in general and for specific symptoms are highlighted in the 2020 ACC/AHA guidelines on the Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy [2]. LVOT obstruction in HCM results from systolic anterior motion (SAM) of the anterior leaflet of the mitral valve and is often a dynamic process (increasing with volume depletion and decreases with volume repletion or afterload augmentation). Hence, understanding the underlying pathophysiological process is crucial in tailoring management decisions [1]. Sudden acute symptoms including hypotensive episodes can be catastrophic in HCM patients. The goals of treatment for acute symptoms in HCM is centered on volume replacement, vasoconstrictors, and controlling tachycardia, while long-term treatment focuses on incorporating negative inotropes, negative chronotropes, risk stratifications, and invasive interventions to reduce obstruction [3]. A pure α-agonist such as phenylephrine is shown to be the agent of choice in managing symptomatic hypotension in HCM with LVOT obstruction [2]. We herein present a case of a 57-year-old female who presented to the emergency department with complaints of shortness of breath (SOB), cough and borderline blood pressure who decompensated during the hospital course and suffered from acute hypotension related to dynamic LVOT obstruction. This case report highlights the importance of having a high index of suspicion to recognize such dynamic LVOT obstruction and further highlights the uniqueness of managing symptomatic hypotension in HCM with LVOT obstruction in an under-resourced hospital.
A 57-year-old female with a past medical history of essential hypertension and peripheral neuropathy and a strong family history of hypertrophic obstructive cardiomyopathy (HOCM), and one sudden cardiac death in her family. The patient presented to the emergency department (ED) with complaints of shortness of breath (SOB) and cough. She had experienced shortness of breath and cough intermittently for 8 years and was evaluated by various specialties without an identifiable cause found. Her symptoms then progressively worsened over a two-week period. She became short of breath walking short distances within her own home and by tying her shoes (indicating Bendopnea). She stated that the chronic cough has been associated with SOB made worse when lying down. She sleeps using 3 pillows (indicating orthopnea). She denied paroxysmal nocturnal dyspnea. The patient denied any sputum associated with cough, recent infection, fever, chills, chest pain, palpitations, headache, blurring of vision, loss of consciousness. Her home medications included Lisinopril 10 mg orally once daily and as needed Albuterol inhaler (as needed which provides temporary SOB symptomatic relief). Vitals in the ED were sinus tachycardia (119 bpm), Temperature (100.4 F), respiratory rate 22/min, Saturation 98% on room air, and blood pressure (106/81 mm Hg). On physical examination, the patient was in Non-Acute Distress (NAD), Alert and oriented times three. Bilateral lower limb edema +2 and raised Jugular Venous Pressure (JVP) were noted. Chest and heart examination revealed bilateral diminished basilar breath sounds and a grade 3/6 systolic murmur best at the apex and left lower sternal border on auscultation. Remainder of the examination was unremarkable. Labs on admission showed: Hematology: WBC 4.7 (reference 4-11 103/uL); RBC 2.06 (reference 3.8-5.20 106/uL); Hgb 11.4 g/dL (references 12-15 g/dL); hematocrit 35.8% (reference 35-45%); MCV 65 (reference 80-100L); RDW 14.7%. Complete metabolic panel included Na 138, (reference 135-147 mmol/L0; Chloride 101 (reference 98-107 mmol/L); Potassium 3.4 (reference 3.5-5.1 mmol/L); calcium 8.5 mg/dL(reference 8.4 -10.2 mg/Dl); anion gap 8.0 mmol/L (reference 4-13 mmol/L) ; serum osmolarity 271 mOsm/kg (reference: 285-305 mOsm/kg); creatinine 0.65 (reference 0.52-1.04 mg/dL); BUN 17 (reference 7-17 mg/dL); glomerular filtration rate (GFR) 73ml/min/1.732, Liver function tests were consistent with hepatocellular injury as follows: alkaline phosphatase (ALKP): 126 U/L (reference: 38-126 U/L); elevated alanine aminotransferase (ALT): 133 U/L (reference 0-35 U/L). Elevated aspartate aminotransferase (AST): 105 U/L (reference 15-46 U/L). Total bilirubin: 0.7 mg/dL (reference: 0.2-1.3 mg/dL), albumin: 4.2 (reference: 3.5-5.0 g/dL). Total protein: 7.9 g/dL (reference: 6.3-8.2 g/dL). Globulin: 3.7g/dL (reference: 2.3-3.5 g/dL). AG ratio: 1.1 (low) and BNP 1310 pg/ml (reference 0-98 pg/ml). Coagulation profile included PT 11.1 (reference 9.4- 11.6 seconds); INR 1.03 (reference 0.8-1.2); and aPTT 32 sec (reference 23-35 seconds). Baseline troponin was unremarkable. COVID-19 test, Influenza A & B tests were negative. Blood gas on admission showed acute hypoxemic respiratory failure. Chest X-ray (Figure 1) showed enlarged cardiac silhouette and bibasilar opacities which may represent infectious/inflammatory process and/or pulmonary edema. ECG (Figure 2) demonstrated sinus tachycardia with ST Depression in leads I, II, III, aVF, V4, V5, V6. On this ECG The Sokolow-Lyon Criteria was not fulfilled for left ventricular hypertrophy (which is the sum of the S-wave in V1 plus the R wave in V5 or V6 is not greater than 35 mm). Chest CT scan was performed without intravenous contrast and demonstrated relatively extensive left lower lung predominant tree-in-bud and ground-glass opacities representing small airways infectious process and enlarged main pulmonary trunk (measuring 3.1 cm). Patient was admitted to the Cardiology unit for further management with provisional diagnosis of community acquired pneumonia and acute exacerbation of heart failure. Mycoplasma and strep pneumoniae antigen levels were ordered. Empiric treatment with antibiotics (Azithromycin 500 MG IV Q24H, and ceftriaxone 1 GM 1000 MG IV Q24H) were initiated, along with oxygen orders (2 L NC) to maintain a goal of saturation above 92%. Given the extensive cardiac history, the patient underwent Two-dimensional echocardiography (Figure 3) which was significant for the findings of severe basal septal hypertrophy (1.79 cm end-diastolic interventricular septum thickness ), decreased LV cavity size, preserved LV ejection fraction (LVEF of 60-65 %), no LV segmental wall motion abnormalities , impaired diastolic function (grade 1-2) , normal right ventricular (RV) size and function, severe chordal SAM with severe Mitral Regurgitation (MR). The resting gradient of the LVOT was elevated to ≥50 mmHg at rest during systole. Tricuspid valve was normal in structure and mild tricuspid regurgitation, with no evidence of severe pulmonary hypertension (calculated RV systolic pressure from tricuspid valve regurgitation to be 17 mmHg) were noted. The inferior vena cava size was normal with > 50% collapsibility (i. e. estimated right atrial pressure of five mmHg). Echo findings consistent with hypertrophic cardiomyopathy. During the hospital's first day of admission, the patient developed SOB and hypotension with vitals BP 95/65 mmHg, pulse 118/minutes. STAT CTA was performed showing no CT angiographic evidence of acute pulmonary embolism, aortic aneurysm, or aortic dissection but grossly unchanged ground-glass nodular /tree-in-bud opacity in the left lower lung suggestive of small airway infectious process. Management was directed at resuscitation Intravenous fluid NS 0.900ccbolus. However, into the second fluid bag, the patient became SOB, tachypneic, and had an increasing cough with hemoptysis. Symptoms further worsened with reverse Trendelenburg positioning, and the patient remained hypotensive despite fluid administration. Hence, fluid was discontinued, BIPAP (EPAP13/ IPAP 6/ rate 23/FiO2 30%) was started, and the patient was transferred to the Intensive Care Unit with vitals HR 132, BP 97/53, SAT 94%on BIPAP. In the ICU, Vasopressors phenylephrine 40 MG IV titrated per ICU unit protocol was started, and the patient was closely monitored to maintain mean arterial pressure > 70 mmHg for adequate cerebral perfusion, and strict Ins and outs were documented. Additionally, antimicrobials were continued, verapamil 120 mg Q 8 hours was added to avoid tachycardia, oxygen was maintained on BIPAP as tolerated (with follow up arterial blood gas: PH -7.43, PCO2- 37, PO2- 124, HCO3- 23.9), nebulizers levalbuterol inhalers 0.63 MG/3 ML 0.63 mg Q 6 Hrs therapy as tolerated, dexamethasone 10 MG IV daily, and benzonatate 200 mg orally TID. The mycoplasma serology Negative, and two sets of blood culture were negative at 48 hours. CBC and CMP during hospital admission did not significantly change. Repeat echocardiogram with and without the phenylephrine showed reduced LVOT gradient and MR with phenylephrine and SBP of 130 mmHg, while LVOT gradient and MR increased off the phenylephrine with SBP <100>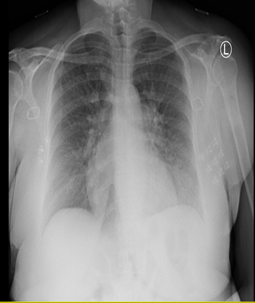
Figure 1: Chest X-ray showing enlarged cardiac silhouette and bibasilar opacities which may represent infectious/inflammatory process and/or pulmonary edema.

Figure 2. ECG on Admission showing Sinus Tachycardia. The Sokolow-Lyon Criteria is not fulfilled for left ventricular hypertrophy (which is the sum of the S-wave in V1 plus the R wave in V5 or V6 is not greater than 35 mm).

Figure 3. Two Dimensional transthoracic echocardiography (TTE) showing A) Parasternal Long Axis view (LAX) in end diastolic frame (Mitral Valve open) showing marked left ventricular hypertrophy in the septum; B) Parasternal LAX view showing Systolic in systolic frame (Mitral Valve closed) anterior motion of the mitral valve (SAM) with dependent significant eccentric and posteriorly directed mitral regurgitation (MR) on Color Doppler (mosaic patterns) with color acceleration; C) Continuous Wave Doppler showing MR with peak Gradient of 138 mmHg; Continuous-wave Doppler signals showing a dynamic gradient with late-systolic peaking and a maximum velocity of 3.7 m/second (maximum pressure gradient 56.46 mmHg), not shown here.
Acute hypotension is a common problem in HCM patients with dynamic LVOT related to SAM of the MV. We herein present a case of a 57-year-old female who presented to the emergency department with complaints of SOB, cough and borderline blood pressure who decompensated and suffered from acute hypotension related to dynamic LVOT obstruction. A pure α-agonist such as phenylephrine is shown to be the agent of choice in managing symptomatic hypotension in HCM with LVOT [2]. Indeed, our patient responded to phenylephrine and was stabilized as a bridge until alcohol septal ablation is arranged (i.e bridge to intervention). This case report highlights the importance of having a high index of suspicion to early recognize such dynamic LVOT obstruction and further highlights the uniqueness of managing HCM patients in an under-resourced hospital utilizing pure α-agonists in managing symptomatic hypotension in HCM with LVOT obstruction.
The hemodynamic goals in patients with HCM relies on the pharmacologic therapies to control symptoms and exercise limitations through reduction of the dynamic LVOT obstruction [3]. Hence, short goal treatment is centered on volume replacement, vasoconstrictors, and controlling tachycardia, while long-term treatment focuses on incorporating negative inotropes, negative chronotropes, risk stratifications for sudden cardiac death (SCD) [4], and invasive interventions to reduce LVOT obstruction [2]. Hypovolemia, tachycardia, systemic vasodilation, and increased contractility all exacerbate the obstruction. Our patient did not improve on aggressive fluid management in an attempt to maintain preload and her symptoms of heart failure worsened.
The use of pure α-adrenergic receptor agonists was the preferred vasoconstrictor agent in this case of HCM with acute hypotension related to dynamic LVOT obstruction [2]. Pure α-adrenergic receptor agonists do not cause tachycardia (i.e., increased oxygen demand), and thus the diastolic filling time is maintained and hence coronary perfusion pressure, and in that regard they are the drug of choice in these cases with acute hypotension refractory to intravenous fluid boluses [5]. Worth mentioning, that in an undifferentiated shock not responding to fluid resuscitation, norepinephrine (an inotrope and a vasopressor) should be the first line vasopressor to use. The increased cardiac contractility is the sole action of Inotropes, which in turn improves cardiac output, facilitating the maintenance of mean arterial pressure (MAP) and perfusion to the body. However, in cases with known or suspected HCM with LVOT obstruction with acute hypotension, the utilization of inotropes should be avoided due to the resultant increase of LVOT gradient, hence the judicious use of vasoconstrictive agents should be considered [2]. The role of phenylephrine in HCM with dynamic LVOT obstruction has been highlighted in a study by Moreno and colleagues, in which utilizing the phenylephrine dynamic drug suppression test (phenylephrine provocation procedure [PPP]) was helpful to guide septal reduction planning in patients with HCM on perioperative transesophageal echocardiography (TEE) [7]. The authors reported [7] that Phenylephrine administration resulted in a change from average baseline MR severity grade of 4.60±0.12 (moderate/severe) to 2.06±0.17 (mild/moderate) with a concomitant increase in SBP of 43±3 mm Hg. Similarly in our patient, the repeat TTE with phenylephrine showed reduced LVOT gradient and mitral regurgitation (MR) grade to mild with an increase in SBP of 130 mmHg, while without phenylephrine, the LVOT gradient increased and MR gradient increased to moderate-severe while SBP was <100>
This case highlights a clinical scenario in which utilizing a pure α-adrenergic receptor agonist in an under-resourced hospital can bridge treatment in the management of patients with Acute refractory hypotension secondary to HCM with dynamic LVOT obstruction. It also further illustrates the key role of comprehensive echocardiography as indispensable modality for the diagnosis, clinical risk stratification, hemodynamic assessment, and the interventional management of patients of HCM.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
