
Case Report | DOI: https://doi.org/10.31579/2641-0419/464
1Director, Cardiac Anaesthesia Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
2Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
*Corresponding Author: Ajmer Singh, Director, Cardiac Anaesthesia Medanta-The Medicity, Gurgaon (Haryana)-122001, India.
Citation: Ajmer Singh, Ravina Mukati, (2025), Unilateral Hilar Prominence: A Diagnostic Dilemma!, J Clinical Cardiology and Cardiovascular Interventions, 8(5); DOI: 10.31579/2641-0419/464
Copyright: © 2025, Ajmer Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2025 | Accepted: 01 April 2025 | Published: 10 April 2025
Keywords: hilum; chest X-ray; unilateral prominence
The radiographic density of the hilum is mainly contributed by the pulmonary arteries and veins, major bronchi, and lymph nodes. Superior pulmonary veins make a small contribution. Though both hila should be indistinguishable in size and density, we do not get equal hila in all the chest X-rays. Rotational malpositioning must be kept in mind, while interpreting chest radiographs of unequal hilum. There are numerous causes of hilar enlargement. It is the clinical presentation which will help in reaching the differential diagnosis. Asymmetric hilum is a challenging subject for clinicians. Interpretation of unequal hilum depends on findings of detail history, meticulous clinical examination, and appropriate investigation.
Interpretation of the hilum is the most difficult part in a chest X-ray. The hilum is composed of pulmonary arteries and veins, major bronchi, and lymph nodes anatomically.[1] Normally bronchi and lymph nodes do not cast any radiological shadow and pulmonary arteries make up most of the radiographic density of the hila. Superior pulmonary veins make only a smaller contribution. Most of the pathological conditions of hila cause bilateral and symmetrical enlargement. Unilateral hilar prominence is rarely seen. The differential diagnoses to be considered include patient rotation, primary or metastatic tumors such as lymphomas or other mediastinal masses, lymphadenopathy, pulmonary artery aneurysm, or pulmonary venous/arterial hypertension.[2]
A 56-year -old man with triple vessel coronary artery disease was admitted for coronary artery bypass graft (CABG) surgery. The physical examination, laboratory tests and electrocardiogram were normal. Chest X-ray showed a prominent shadow in the left hilar region (Figure 1). There was no history of smoking, loss of weight, cough, fever, pulmonary tuberculosis, radiation, or malignancy. The unilateral hilar enlargement gave rise to diagnostic dilemma!
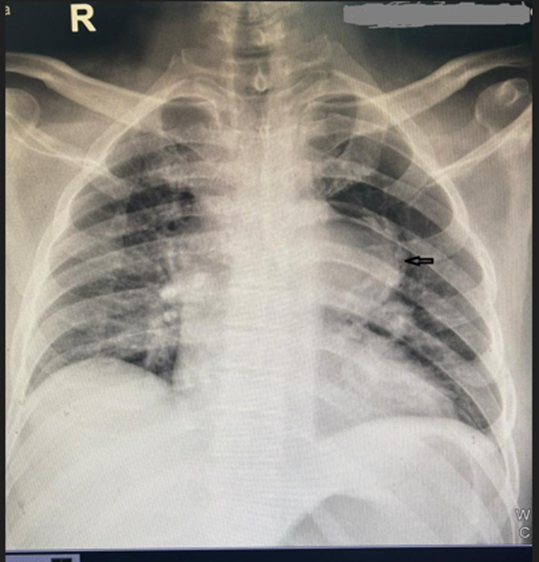
Figure 1: Chest radiograph showing left hilar prominence (arrow) and increased pulmonary vascularity
Further evaluation with two-dimensional echocardiography showed a restrictive subpulmonic ventricular septal defect (VSD) with a peak gradient of 108 mmHg and a left to right shunt. The other echocardiographic findings were a normal left and right ventricular function, left ventricular dilation (end-diastolic dimension 56 mm), trace tricuspid valve regurgitation with pulmonary artery systolic pressure of 21 mmHg. The patient was taken for VSD closure and CABG surgery. Upon opening of the chest, left pulmonary artery was seen prominently protruding to the left side, consistent with the chest X-ray findings. Pulmonary artery catheter used for intraoperative monitoring showed normal pulmonary artery pressures and a step-up in oximetry saturation from right atrium to pulmonary artery. The right atrial saturation was 49.1% and the pulmonary artery saturation was 80.2%, suggestive of a left to right shunt at the ventricular level. Intraoperative transesophageal echocardiography (2D and 3D) confirmed the presence of subpulmonic VSD (Figure 2, Figure 3). The patient underwent Dacron patch closure of VSD and triple vessel CABG surgery using cardiopulmonary bypass. Post cardiopulmonary bypass echocardiography showed no residual left to right shunt (Figure 3C); and the saturations of the right atrium and the pulmonary artery were equal (65.8 percentage each). The further course of the patient in the hospital was unremarkable.
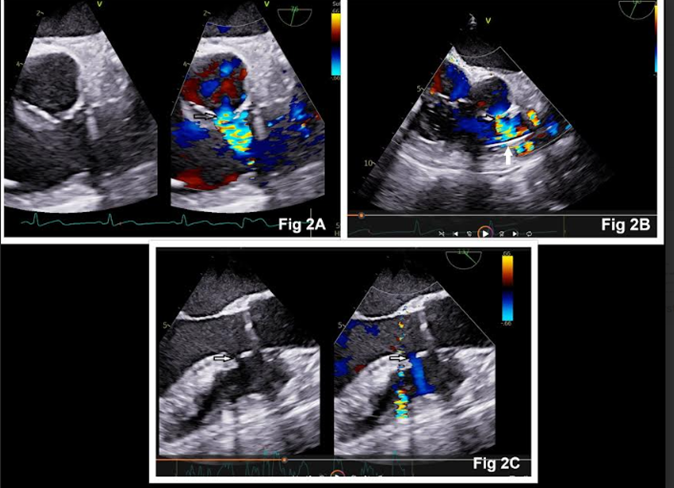
Figure 2: Transesophageal echocardiography showing subpulmonic ventricular septal defect (arrows) in aortic valve short-axis view (Figure 2A), right ventricular inflow-outflow view (Figure 2B), and long-axis view (Figure 2C). Pulmonary artery catheter is seen in Figure 2B (white arrow)
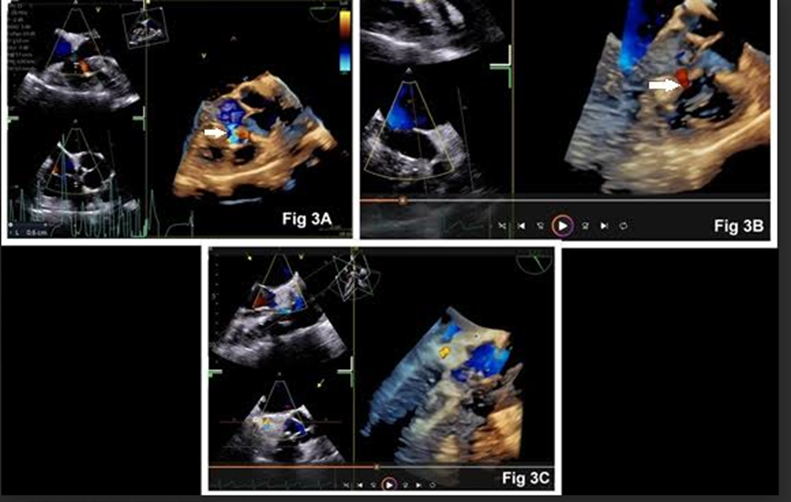
Figure 3: Three-dimensional echocardiography showing ventricular septal defect (arrows) in Figure 3A and Figure 3B. No residual defect was seen after surgery (Figure 3C)
The hilum consisting of blood vessel, bronchi, and lymph nodes, can show enlargement which may be unilateral or bilateral, symmetrical or asymmetrical.2 In combination with clinical information, each of these patterns is often helpful in reaching a diagnosis. Bilateral, symmetrical hilar enlargement should raise the suspicion of sarcoidosis, particularly if there is evidence of paratracheal enlargement, or lung parenchymal shadowing.[3] It should however, must be differentiated from lymphoma, lymphadenopathy, pulmonary venous hypertension, pulmonary arterial hypertension, metastatic disease or infection which may look similar. Lymphadenopathy or tumor are visualized as rounded, non-branching structures in which the radiopacity abruptly diminishes at the margin of the tumor or lymph node. Pulmonary venous hypertension causes increased vascular density in the upper half of the hilum due to enlargement of superior pulmonary veins. Pulmonary arterial hypertension causes dilation of central (main) pulmonary artery which tapers abruptly. Increased pulmonary blood flow caused by left to right shunt, as observed in this patient, results in increased central and peripheral pulmonary vascular markings (peripheral lung markings become visible in the peripheral 1–2 cm of the lung).
Unilateral hilar prominence, however, is rarely seen in patients with increased pulmonary blood flow, making it a unique case. The left pulmonary artery is very characteristic in its appearance on the posteroanterior film, creating a density above and lateral to left main bronchus. The left main pulmonary artery arches over the left main bronchus and parallels the inferior border of the aortic arch. The ‘hilum convergence sign’ is a useful chest radiograph sign to help distinguish a bulky hilum due to pulmonary artery dilation. Pulmonary vessels can be seen to converge and join a dilated pulmonary artery. The sign is useful to distinguish between a prominent hilum and an enlarged pulmonary artery.[4] If branches of pulmonary artery converge towards central mass, it is an enlarged pulmonary artery rather than mass or lymph node in the hilum. Unilateral aplasia of the branch pulmonary artery can also cause enlargement of the opposite pulmonary artery. Pulmonary artery aneurysm can cause focal dilation involving all three layers of the vessel. Common causes of pulmonary artery aneurysm include congenital heart diseases, particularly those resulting in left-to-right shunts, pulmonary hypertension, pulmonic stenosis, and vasculitides, such as Behçet disease and Hughes-Stovin syndrome.[5]
Asymmetrical hilar prominence may also be seen in patients with infections caused by fungal, atypical mycobacteria, viral, silicosis, drug reaction, breast cancer, other malignant diseases, mastectomy, aortic aneurysm, or radiation fibrosis. Multimodal imaging consisting of chest radiography, bronchoscopy, mediastinoscopy, echocardiography, contrast-enhanced computed tomography, positron emission tomography, and magnetic resonance imaging may be required to confirm the etiology and diagnosis. Radiographic features of tuberculosis include enlarged hilar lymph nodes with or without a discrete parenchymal infiltrate.[6] In lymphadenopathy, there is enlargement of anterior mediastinal lymph nodes in addition to hilar node prominence. Pulmonary embolism can be diagnosed by pulmonary arteriography.[7] In some cases, a biopsy of the enlarged lymph nodes or lung tissue may be necessary to determine the underlying cause. Hilar malignancy treated with radiation therapy can cause tracheal deviation and loss of lung volume in the affected hemithorax. Thoracic aortic aneurysm may cause mediastinal widening, prominent aortic knuckle, tracheal deviation, and tortuous descending aorta.
Unilateral hilar prominence is a challenging subject for the clinicians. Interpretation of unequal hilum depends on findings of detail history, meticulous clinical examination, and appropriate investigation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
