
Research Article | DOI: https://doi.org/10.31579/2641-0419/442
1Cardiology Department - ERRAZI Hospital - Mohammed VI University Hospital, Marrakech.
2Physiology Department - ERRAZI Hospital - Mohammed VI University Hospital, Marrakech.
*Corresponding Author: Rim Zerhoudi, Cardiology Department - Errazi Hospital - Mohammed Vi University Hospital, Marrakech.
Citation: Rim Zerhoudi, Halima Eljazouli, El Qadi CA, Joumana Elmasrioui, Abdelkarim A. Yahya, et al, (2025), Unforeseen Threats: Mechanical Complications in the Aftermath of Acute Coronary Syndromes, J Clinical Cardiology and Cardiovascular Interventions, 8(3); DOI: 10.31579/2641-0419/442
Copyright: © 2025, Rim Zerhoudi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 January 2025 | Accepted: 31 January 2025 | Published: 13 February 2025
Keywords: acute coronary syndrome; mechanical complications; heart murmur; st-segment elevation; echocardiography; cardiogenic shock
Introduction: Acute coronary syndromes (ACS) are cardiovascular emergencies resulting from the rupture or erosion of atherosclerotic plaque in the coronary arteries. Despite therapeutic advances that have reduced mortality, serious mechanical complications, such as myocardial rupture, acute valvular insufficiency and ventricular septal defect, can still occur, increasing the risk of mortality. The present work aims to describe mechanical complications in ACS in our setting, examine their frequencies, pathophysiological mechanisms and therapeutic approaches through our series and literature review.
Materials and methods: This retrospective study included 20 patients with mechanical complications of myocardial infarction, mainly diagnosed at the thoracic pain unit of the Mohammed VI University Hospital, Marrakech, and hospitalized in cardiology over a two-year period. Selected patients presented with myocardial rupture, acute mitral insufficiency, interventricular septal rupture, right ventricular free wall rupture or left ventricular aneurysm. Data on incidence, diagnosis and clinical outcome were analyzed.
Results: During the study period, 20 patients, with a mean age of 69 and a female predominance, presented with post-infarction mechanical complications without a history of ischemic heart disease. The main complications included ventricular septal defects (50%), intramyocardial dissections (15%), acute mitral insufficiency (15%) and ventricular wall rupture. Echocardiography enabled rapid diagnosis. Half the patients were stable on admission, while three quarters progressed to cardiogenic shock, often fatal.
Discussion and conclusion: Mechanical complications of ACS are rare but serious events that complicate patients' prognosis. Early detection by echocardiography or cardiac MRI, followed by surgical management, remains crucial to improving survival. Advances in early revascularization, notably coronary angioplasty, have helped to reduce the incidence of these complications, but optimal treatment of advanced cases relies on an experienced multidisciplinary team.
Acute coronary syndromes (ACS) represent a group of cardiovascular emergencies linked to the rupture or erosion of atherosclerotic plaque in the coronary arteries. Although current treatments significantly reduce mortality, serious mechanical complications can still occur, particularly in the absence of prompt intervention. These complications include myocardial wall rupture, acute valvular insufficiency and ventricular septal defect, each contributing to a high risk of mortality.
The present work aims to describe mechanical complications in ACS in our setting, examine their frequencies, pathophysiological mechanisms and therapeutic approaches through our series and literature review.
This was a retrospective study of 20 patients with a mechanical complication of myocardial infarction diagnosed mainly in the thoracic pain unit and subsequently hospitalized in the cardiology and vascular diseases department at the Mohammed VI University Hospital, Marrakech, over the past two years.
Inclusion criteria included clinical studies of patients with myocardial infarction complicated by myocardial rupture, acute mitral insufficiency, interventricular septal rupture, LV free wall rupture and LV aneurysm. Data on incidence, diagnostic methods and clinical outcomes were extracted and analyzed
During the study period, 20 patients developed post-infarction mechanical complications. The mean age of the patients was 69 years, with an age distribution ranging from 60 to 85 years, and a predominance of women. No history of ischemic heart disease was found in this cohort. All cases presented to the emergency department with acute coronary syndrome, characterized by ST-segment elevation beyond the therapeutic window for thrombolysis.
Of the complications observed, 50% corresponded to post-infarction ventricular septal defects with left-to-right shunting, 15% of cases were intramyocardial dissections, while the same percentage involved acute mitral insufficiency linked to papillary muscle dysfunction. Ten percent of patients presented with right ventricular free wall rupture, and the remaining cases were left intra-ventricular aneurysms. Anterior involvement on the electrocardiogram was the most frequent, and echocardiography was decisive in establishing the diagnosis of mechanical complications on admission.
Half the patients were admitted in stable clinical condition, while the remainder had left ventricular failure graded between Killip III and IV. Three quarters of patients progressed to cardiogenic shock, with a fatal outcome in hospital.

Figure 1: This is a 76-year-old patient admitted with inferobasal STEMI. The echocardiography showed segmental hypokinetic heart disease with preserved systolic function, a ruptured image in the inferobasal segment of the interventricular septum, and a breached right ventricle opposite its free wall, with systolic dysfunction.
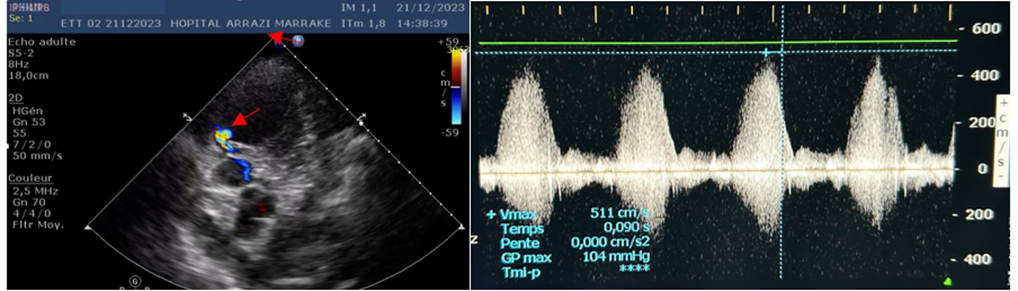
Figure 2: This 66-year-old patient was admitted with STEMI anteriorly. Echocardiography showed segmental hypokinetic heart disease with severe LV dysfunction (30-35%), the site of an apical aneurysm, associated with a 7 mm apical muscular IVC image responsible for a left-right shunt.
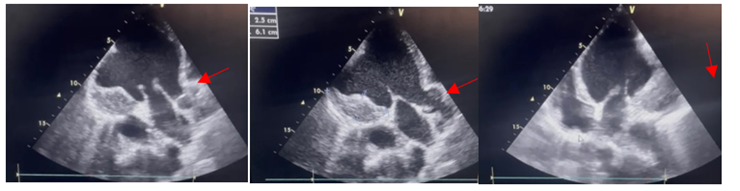
Figure 3: This 70-year-old patient was admitted with extensive anterior STEMI. Echocardiography showed segmental hypokinetic heart disease with severe LV dysfunction (20-25%) and an aneurysmal anterolateral wall containing a thrombus measuring 6.1 x 2.5 mm.
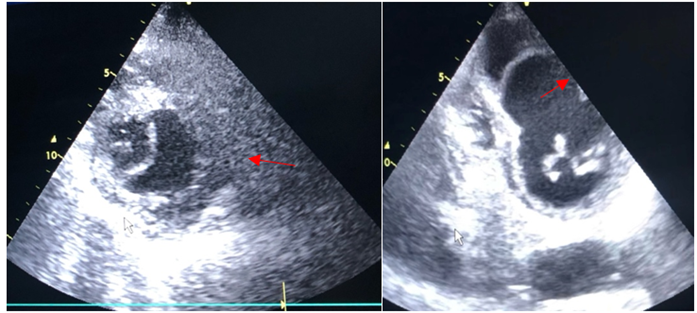
Figure 4: This 84-year-old patient was admitted with STEMI anteriorly. Echocardiography showed segmental hypokinetic heart disease with severe LV dysfunction (30%), a thickened, pulsatile LV cavity with dyskinetic motion, surrounded by a thin endomyocardial membrane in association with a haematoma secondary to intra-myocardial rupture.
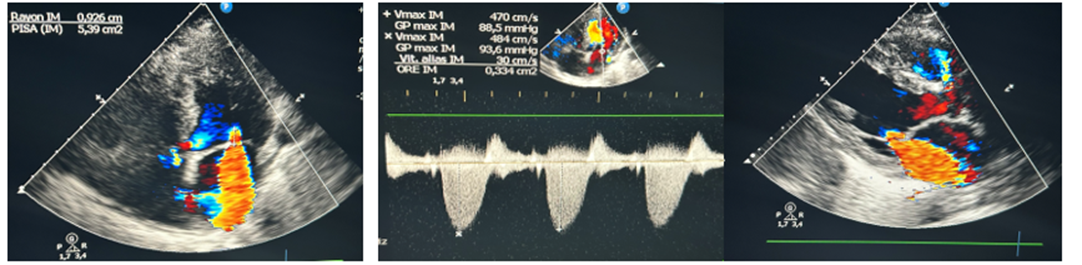
Figure 5: This 77-year-old patient was admitted with post-MI angina in inferior position, extended to the right shunts at H24, complicated by cardiogenic PAO. Echocardiography showed acute mitral insufficiency, on segmental hypokinetic cardiopathy with severe 30-35% LV dysfunction.
Reperfusion therapies have significantly reduced the frequency of mechanical complications following acute myocardial infarction. Studies estimate that after a myocardial infarction with ST-segment elevation, between 0.27% and 0.91% of patients develop mechanical complications. Papillary muscle rupture, ventricular wall rupture, and septal rupture occur in 0.05% to 0.26%, 0.01% to 0.52%, and 0.17% to 0.21% of cases, respectively [1,2]
Unfortunately, mortality rates associated with these complications have not significantly decreased over the past two decades, and patients with such mechanical complications are four times more likely to die in the hospital than those without complications. Although rare, mechanical complications remain a critical determinant of post-infarction prognosis [1,2,3]. While the proportion of patients with ST-segment elevation myocardial infarction has decreased over time, contemporary patients facing mechanical complications are often older, predominantly female, with a history of heart failure and chronic kidney disease, and frequently experiencing their first myocardial infarction [4,5,6]. Furthermore, socioeconomic disparities have a substantial impact on post-MI outcomes [7].
These complications include; Rupture of the left ventricular free wall, Acute severe MR, papillary muscle displacement, papillary muscle rupture, Ventricular septal rupture, Pseudo aneurysm formation, RV infarction, Dynamic LV outflow obstruction, LV thrombus.

Figure 6: Characteristics of mechanical complications of acute myocardial infarction (7).
HF indicates heart failure; LA, left atrium; LV, left ventricle; and MR, mitral regurgitation. ©2020 Devon Medical Art LLC.

Table 1: Summary of Major Mechanical Complications of Acute Myocardial Infarction (8)
1.Post-myocardial infarction ventricular septal defect:
Post-infarction ventricular septal rupture (VSR) is defined as a rupture of the interventricular septum at the boundary between healthy and infarcted tissues [9,10]. The underlying mechanism involves the formation of an intramural hematoma within the infarcted area, leading to tissue dissection followed by rupture. The rupture typically occurs within 5–7 days after myocardial infarction (MI) but can sometimes occur within the first 24 hours due to a direct tear of the interventricular septum. The hemodynamic consequences include the presence of a left-to-right (L-R) shunt, resulting in volume overload of the left ventricle and pressure and volume overload of the right ventricle, which leads to biventricular failure with a predominance of right-sided failure [9,10].
The incidence of VSR represents 0.2% of all STEMI cases, compared to 1–2
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
