
Research Article | DOI: https://doi.org/10.31579/2578-8868/219
1 PhD, Senior Neuropsychologist, Associate Professor, Department of Psychology.
2 MD, PhD, Consultant Physiatrist, Department of Community Medicine and Rehabilitation, Umeå University, 901 87, Umeå, Sweden
*Corresponding Author: Xiaolei Hu, MD; PhD; Consultant physiatrist Department of Community Medicine and Rehabilitation Umeå University, 901 85 Umeå, Sweden.
Citation: Eva Elgh and Xiaolei Hu (2021). Subjective and Objective Assessments of Executive Functioning among Persons 10 years after Stroke Onset. J. Neuroscience and Neurological Surgery. 10(1); DOI:10.31579/2578-8868/219
Copyright: © 2021 Xiaolei Hu, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 23 November 2021 | Accepted: 30 November 2021 | Published: 06 December 2021
Keywords: executive function; stroke; cognition; patient-reported outcome measurements; neuropsychology assessment; caregivers
Aim: This study aimed to investigate executive functioning (EF) among patients 10 years after stroke onset through comparing subjective patients’ and informants’ perceptions as well as objective neuropsychological assessments (NPAs).
Materials and Method: One month prior to the neuropsychological assessment, 36 patients and their informants completed the Behaviour Rating Inventory of Executive Function - Adult Version (Brief-A) around 10 years after stroke onset. The patients’ EF was assessed with verbal fluency (FAS), backward Digit span backward and Trail making test (TMT)-B.
Results: We found no significant differences between patient and informant ratings on EF on a group level, but more patients reported clinically significant executive dysfunctions (T > 65) than their informants. Only poor to slight agreements were observed between the patient and informant ratings of the BRIEF-A. Digit span backward was the only executive test that demonstrated significant improvement of EF 10 years post-stroke in the cohort. Neither patient nor informant ratings on EF showed any significant association with objective EF test performance.
Conclusions: Mismatch patient-informant agreement on perceived executive dysfunction showed no clear association with EF test performance in this study. This may indicate the complexity of EF among persons with stroke at chronic phase.
Impairment of executive function (EF) is a common cognitive sequelae after stroke with profound negative effects on patients’ activity of daily living and participation [1] . The prevalence of executive dysfunction after stroke varies from 19% to 75
Study design and procedure
Data of this study were collected in a single-centre prospective, longitudinal cohort study of stroke survivors with three consecutive follow-ups over a 10-year period after a first-ever stroke. The cognitive functions of stroke survivors were assessed prospectively at 10-year follow-up, then compared retrospectively with data collected 1 week after and 7 months after stroke before the study was planned [2,17]. The study was conducted at a Department of Neuro-Rehabilitation, University Hospital of Umeå. Ethical approval was obtained from the regional Ethical Review Board in Umeå, Sweden, D-nr 2015/144-31.
All young (18 to 65 years) patients who had suffered a first-ever stroke between January 2004 and December 2007 and undergone neuropsychological assessment (NPA) within the first year after stroke were contacted. Participants were informed about the study and provided with written consent forms via letter, and research staff made contact via telephone with all eligible patients in order to improve the recruitment rate. Patients with severe dementia, severe aphasia, severe comorbidity, recurrence of stroke or transient ischemic attack, or other physical or psychiatric disease after first-ever stroke, along with those who were not community-dwelling, were excluded [2]. After a thorough recruitment process taking place from 2015–2016, 49 of the total 102 first-ever young stroke patients with acute NPAs declined, and 15 others were excluded for a variety of reasons. In this study, two of 38 participants were excluded because of missing values in BRIEF-A. Seven participants lived alone without relative. Only 26 informants completed BRIEF-A without missing values. All were native Swedish citizens. The 38 participants provided their written informed consent to participant the study and assessed by NPAs. Baseline data were collected from the Riksstroke registry and from patients’ medical records.
Behaviour Rating Inventory of Executive Function - Adult Version (BRIEF-A)
For subjective assessment of executive functioning, both participants and informants completed the BRIEF-A one month prior to the scheduled appointment for NPA.
BRIEF-A measure executive functions in daily living through self- and informant assessment [13]. The BRIEF-A consists of 75 items that measure different aspects of EF in the real-life situation. Answers are given on three options (i.e. never a problem =1, sometime a problem =2 and often a problem =3). Three index score were derived: 1) Behavioural Regulation (BRI) refers to the ability to control behaviours and emotions, consisting of subscale inhibit, shift, emotional control and self-monitor; 2) Metacognition (MI) refers to the ability to maintain attention and the ability to solve problems, consisting of subscale initiate, working memory, plan/organize, task-monitor and organization of material; 3) Global Executive Composite (GEC) is a summary scale for all subscales. The American standards were used to convert raw points into T-points [13]. Higher T scores indicate higher degree of executive dysfunction. T scores at and above 65 are considered as clinically significant impairments on EF [13].
In order to objective assess patients’ executive function, three neuropsychological assessments were used in the current study and described below.
Verbal fluency
Phonemic fluency (FAS) is included in the executive test battery Delis-Kaplan Executive Function System (D-KEFS). The battery is standardized for individuals between the ages of 8 and 89 [8]. In this study, the patients were asked to say as many words as possible starting with a certain letter (F, A and S) for 60 seconds to measure the ability to orally produce words [8].
Digit Span
Digit Span from Wechsler Adult Intelligence Scale (WAIS) -IV was used to assess the working memory´s number storage capacity. Notably, WAIS-R and WAIS-III was replaced by WAIS-IV at 10-year follow-up due to practical reason. Previous validation studies have shown that WAIS-IV have the same construction as WAIS-III/R [18] with very high correlation between subscales (r = .82-94) [9]. Swedish norms for WAIS-IV were used as control [9].
Trail making test (TMT) - B TMT-B intends to measure the executive function mental flexibility, i.e. the ability to switch between different stimuli under time pressure [19]. An upper time limit was used (190 seconds) [19].
Data presentation and statistical analysis
Demographic characteristics are presented as Mean ± SD, number with/without number of cases (%) or median (25%- 75% interquartile ranges (IQR)) as appropriate.
Data from Brief-A were analysed using Wilcoxon matched-pairs signed rank test. The Cohen’s kappa coefficient was used to measure the agreement between the patient and informant rating of the BRIEF-A (0= poor agreement, 0.2 = slight agreement, 0.4 = fair agreement, 0.6 = moderate agreement, 0.8 = substantial agreement and 1.0 = almost perfect agreement) [20].
The NPA at the early stage were presented at two time-points, i.e. one week and seven months with some missing values. Instead of ANOVA, Kruskal-Wallis test was chosen for nonparametric multiple comparisons between three time-points because of the relatively small sample size. Each p value was adjusted to account for multiple comparisons with Dunn’s multiple comparisons test.
The level of associations between BRIEF-A and neuropsychological data were explored by using Spearman correlation coefficients. The statistical analyses were performed by using the software product GraphPad Prism, version 6.0 or IBM SPSS as appropriate. P value 0.05 was considered as significant.
Demographic and medical characteristics
Demographic and medical characteristics of the participants at 10-year follow-up after stroke onset are presented in Table 1.
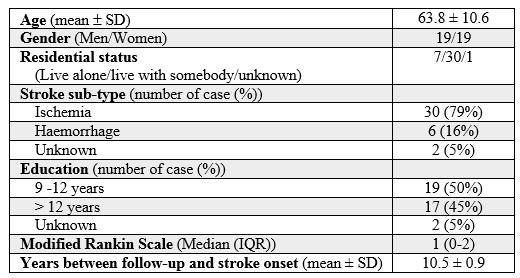
The mean age of participants was 63.8 (SD 10.6) with 50 percentage female participants. Most of the participants (n= 34, 34/37, 92%) had no or only slight disability (mRS= 0-2). Ischemia was the dominate stroke sub-type (79%). Almost half of the participants (n= 17, 17/37, 46%) had more than 12 years education. The more detail characteristics of the participants have been described in the previous studies [2,17].
Comparison of patient and informant rating on the BRIEF-A
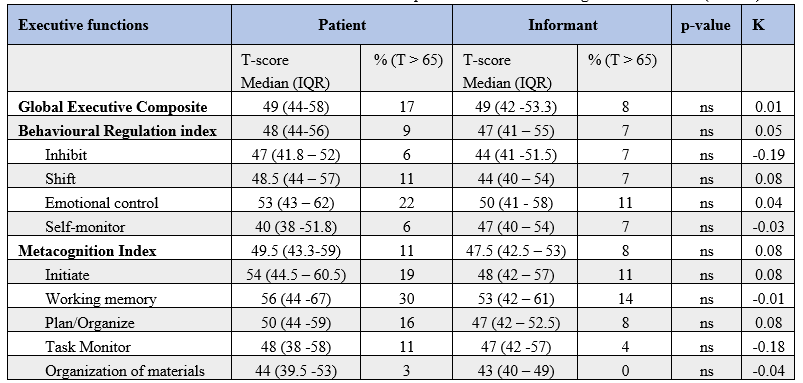
Descriptive data from patient and informant ratings of the BRIEF-A were presented in Table 2.
On a group level, there was no median score of any subscale or main indexes of the BRIEF-A over 65 points i.e. the level for clinically significant impairment; but more patients reported clinically significant executive dysfunctions (T > 65) than their informants did. However, the statistical analyses demonstrated no significant differences between patients and informants reporting on any of the subscales or main indexes on BRIEF-A. Similar medians of global executive function (GEC) were rated by patients and informants. A slightly higher score were observed on BRI and MI among patients, but no significant difference.
Cohen k statistics demonstrated poor to slight agreements between the patient and informant ratings of the BRIEF-A (Table 2).
Neuropsychological data
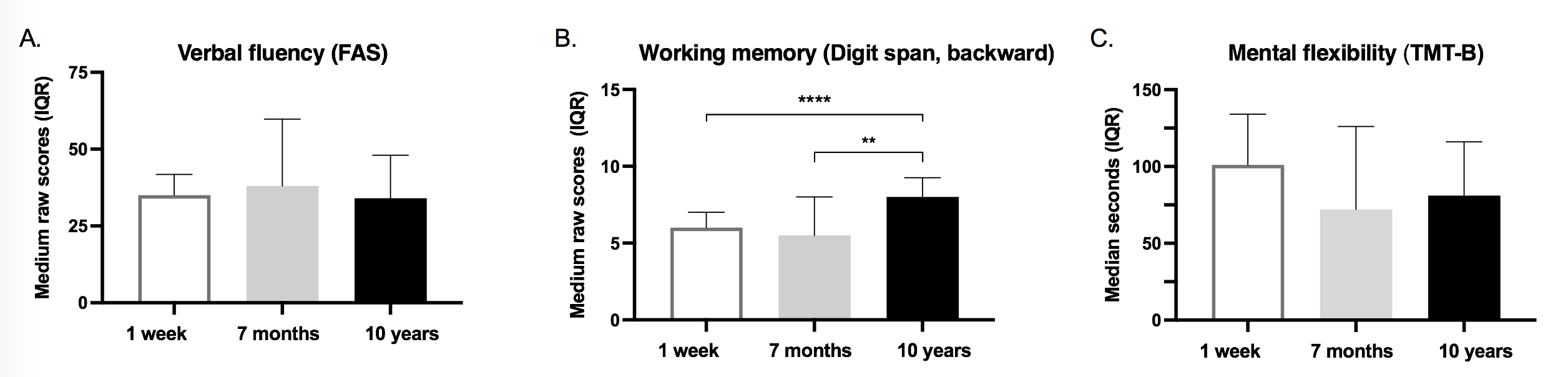
Three NPA test data over 10-year follow-up are shown as median (25%- 75% IQR) in Figure 1. Compared to results at one-week post-stroke, no significant enhancements on working memory were observed at 7 months after stroke onset assessed by WAIS-Digit span [9]. However, striking significant improvements were demonstrated at 10-year follow-up in Digit span (backward) score (8 (6-9.3)) (Figure 1B). However, Verbal fluency (FAS) (34 (25.8-48)) and TMT-B (81 (62 – 116)) at 10-year follow-up demonstrated no significant differences compared to the data at the early time-points, respectively (Figure 1A and 1C).
Associations between subjective and objective EF
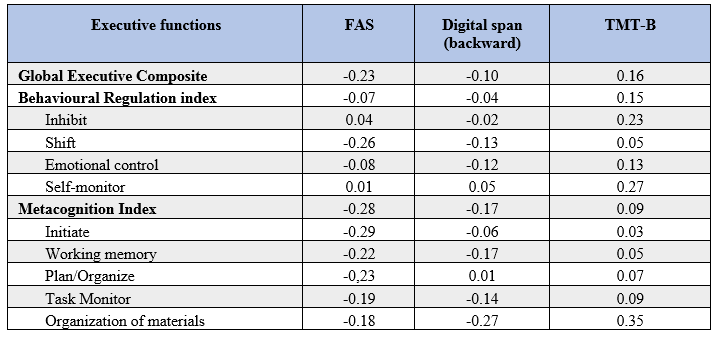
No significant association was found between patients perceived
executive dysfunction and any of the tests of executive function (Table 3). Similarly, informant ratings of executive function didn’t show any significant relationship with objective assessments of EF (Table 4).

This study aimed to investigate EF among patients at 10-year after stroke onset through comparing subjective patients’ and informants’ perceptions of EF as well as objective assessments of EF. We found that patient and informant reported EF similarly on a group level, but more patients reported clinically significant executive dysfunctions than their informants did. Mismatches were observed between the patient and informant ratings of the BRIEF-A. Digit span backward was the only executive test that demonstrated significant improvement of EF at 10-year post-stroke in the cohort. However, performance-based EF tests did not demonstrate any significant association with patient nor informant ratings on EF.
Our data presented only subtle executive dysfunction in the participants from both patient and informant ratings on EF, which is congruent with highly independence in daily living reported by the participants. More patients reported clinically significant executive dysfunctions than their informants did. This may suggest that perceived executive dysfunction by patients is not always noticed by their relatives. The current results are also in line with many early studies where discrepancies between patient- and informant-reported EF impairments were demonstrated among patients with dementia or traumatic brain injury [10, 15, 16].
Among three performance-based executive tests, Digit span backward assessing working memory was the only test that demonstrated significant improvement over 10-year post-stroke in the cohort. No significant alteration was observed on mental flexibility (TMT-B) and verbal fluency (FAS) over 10-year follow-up. The reason for these discrepancies on NPA results are not fully understood but the tests measure different aspects of executive function located in different parts of the frontal lobes [21]. One possible explanation is that working memory, but not mental flexibility and verbal fluency, could be trained by active daily living [1, 2]. This is supported by the finding that more than 90% of participants in the cohort were independent in their daily activities. Another possible reason is that verbal fluency and TMT-B, unlike Digit span, have a time aspect as part of the test [9, 19]. This time pressure could make it more difficult for the patient. Furthermore, higher education level among the participants has in a previous study predicted better improvement of working memory, but not mental flexibility or verbal fluency (unpublished data [22]); and in this study a majority had more than 12 years of education.
Neither patient nor informant ratings on EF showed any significant association with objective performance-based EF tests in the study. The very small, non-significant correlations observed in the current study suggested that these three different tests should not be considered equal nor be used interchangeably [10]. Our results were consistent with many previous studies among patients with acquired brain injury or dementia [14-16] but not all [10]. The BRIEF-A provides a more complex, integrated and dynamic information on EF in the daily living [13] while NPA detects specific EF domains in a well-controlled standardized condition [9]. They may thus provide certain complementary information on EF. The clinical implication of the present findings may suggest that persons with stroke need both subjective and objective assessments on executive dysfunction due to its complex nature. It is necessary to performed these assessments in a large amount of stroke patients over a long-term follow-up to confirmation the generalisability of the current findings; and to enhance the knowledge of executive dysfunction after stroke.
The strength of the current study was the very long-term follow-up duration with repeated objective EF assessments at acute, sub-acute, and chronic phases over ten years after stroke onset. However, we are aware of the small number of participants as one of the limitations. Furthermore, stroke characteristics, such as stroke location and size, were not taken into account in the data analysis even though stroke severity is an important predictor of outcomes [23, 24]. This is why it is not possible to generalize the findings to the entire young stroke population. Nevertheless, the current study provided some interesting insights into subjective and objective EF assessments.
We demonstrated that mis-match patient-informant agreement on perceived executive dysfunction showed no clear association with EF test performance in this study. This may indicate the complexity of EF among persons with stroke at chronic phase. Both subjective and objective assessment might provide certain complementary information on EF. A large-scale study is needed to confirm the generalisability of the current findings among stroke patients.
The authors would like to thank each participant and assessor for their patience and time. We also wish to acknowledge rehabilitation coordinator Catharina Elback for her excellent recruitment work.
This study was supported by the Västerbotten County Council and Umeå University (ALF Foundation), the Swedish Stroke Foundation (Stroke Riksförbundet) and the Northern Swedish Stroke Fund (Strokeforskning i Norrland Insamlingsstiftelse).
The authors report no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
