
Review | DOI: https://doi.org/10.31579/2578-8949/075
Department of dermatology, Saudi German hospitals and clinics, Hessa Street 331 West, Al Barsha 3, Exit 36 Sheikh Zayed Road, Opposite of American School, Dubai, United Arab Emirates.
*Corresponding Author: Piyu Parth Naik, Department of dermatology, Saudi German hospitals and clinics, Hessa Street 331 West, Al Barsha 3, Exit 36 Sheikh Zayed Road, Opposite of American School, Dubai, United Arab Emirates.
Citation: Piyu P Naik. (2021) Tyrosine kinase inhibitors in dermatology: A systemic review. Dermatology and Dermatitis. 6(1); Doi:10.31579/2578-8949/075
Copyright: © Piyu Parth Naik, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 May 2021 | Accepted: 21 May 2021 | Published: 24 May 2021
Keywords: tyrosine kinase inhibitors; jak inhibitors; alopecia areata; atopic dermatitis; baricitinib; psoriasis; ruxolitinib; tofacitinib; vitiligo
The inhibition of enzyme subgroups of tyrosine kinases can block the ability of various cytokines at the same time. Tyrosine kinase inhibitors are a class of drugs that can be used either primarily as oral medicines or in dermatological definitions locally. In several skin problems, restraint of tyrosine kinases has been demonstrated to be advantageous. Aim of this article is to explore the role of tyrosine kinase inhibitors in various skin diseases. Tyrosine inhibitors have demonstrated a guaranteed response in psoriasis, alopecia areata, Vitiligo, while the variable response in other skin disorders, including atopic dermatitis, chronic actinic dermatitis, dermatomyositis, erythema multiforme, graft-versus-host disease, hypereosinophillic syndrome, STING vasculopathy, palmoplantar pustulosis and lupus. The approach of Tyrosine inhibitors in dermatology has been met with incredible interest. This class of prescriptions can generously propel the treatment of inflammatory and immune mediated dermatoses. It is still too early to make a strong inference regarding these medicines' place in dermatological treatment, even though the evidence provides promising results.
Our understanding of the pathogenesis of provocative and immunological infections has gained extraordinary advancement over recent years, thus revealing novel remedial goals. Protein tyrosine kinases (PTKs) handle cell multiplication, immune response and bolstering signaling in cells within theoretical models. Unchecked movements from tyrosine kinase receptors and intracellular tyrosine kinases can lead to fiery reactions of cytokines and lead to autoimmune diseases, dermatitis and even malignancy [1].
The Tyrosine kinase inhibitors, necessary for the downstream motioning of inflammatory cytokines, are among late perceived targets [1]. In dermatology, tyrosine kinase inhibitors have their spot in the blockage of cytoplasmic Janus kinases, which is a subclass of huge tyrosine kinase family. Various investigators have thought about aiming Janus kinases or JAKs starting late due to promising initial results. New disclosures in JAK-STAT pathway and the improvement of medications that block their related activity have made new entryways for treating issues related to this system's dysregulation [2].
After clinical fundamentals performed, with first generation of JAK inhibitors like tofacitinib, ruxolitinib, baricitinib and oclacitinib, dermatological conditions like psoriasis and atopic dermatitis, received the dermatology field's most significant advantage [2].
Another condition that has shown promising outcomes from treatment with JAK-inhibitors is Alopecia areata (AA). Other immune mediated cutaneous disorders where JAK-inhibitors are useful include Vitiligo, atopic dermatitis (AD), chronic actinic dermatitis, chronic mucocutaneous candidiasis, cutaneous T-cell lymphoma, dermatomyositis, hypereosinophillic syndrome, cutaneous Graft Versus Host Disease (GVHD), cutaneous mastocytosis, palmoplantar pustulosis, STING vasculopathy, and lupus erythematosus [2].
The current systematic review has followed Preferred Reporting Items for Systematic Reviews (PRISMA) method [3]. A systematic review comprises the structured collection of evidence-based articles followed by systematically discussing their findings based on the review's aim.
An articles search was undertaken electronically using online databases such as Google Scholar, MEDLINE, PubMed, Scopus and Cochrane databases with the appropriate key terms (MeSH). We were looking specifically for articles on Tyrosine kinase inhibitors in dermatology. The keywords were changed according to each database's searching protocol, including "Tyrosine kinase inhibitors," "JAK inhibitors," "Dermatology." Bibliographic sources were also screened.
The articles published related to Tyrosine kinase inhibitors in dermatology were included in this review. The research articles, case studies, studies related to other than dermatological disorders, review and systematic review and articles published other than the English language were excluded in this study.
The initial literature search revealed 717 articles. Relevant articles were chosen for full-text screening after the application of the eligibility criteria.
The literature search yielded 717 articles from various databases, including PubMed, Ovid, Science Direct and Google Scholar, of which 305 articles were excluded at the initial stage due to repetition and irrelevance. Out of 412, 278 articles were further excluded after analyzing the titles and abstracts at the first screening level. Finally, 134 studies meeting the current systematic review's inclusion criteria as detailed in the PRISMA flow chart were included in this review. (Figure 1)

The references to each relating articles have additionally been looked up. Furthermore, clinical trials were further used to look for clinical preliminaries.
Our hunt yielded 134 items, comprising 44 review articles, 78 unique original articles (53 clinical investigations and 25 preclinical examinations in vitro and in vivo), and 12 reports on adverse events.
Among the clinical examinations (43%) and clinical trials (38.7%), Psoriasis was the most well-known skin disease found, which responded to this group of medicines. The other common condition considered in preclinical investigations was dermatitis (Table 1).

The adequacy of Tyrosine Kinase inhibitors in the treatment of skin and hair problems was accounted for in 29 of the 46 papers recognized.
The pathway of tyrosine kinase and associated cytokines to action and dysregulation has been connected as a potential psoriasis disease component. Either oral or topically administered tyrosine kinase inhibitors have been beneficial in the treatment of Psoriasis. The most extensively read finished paperwork for Tyrosine Kinase inhibitors in dermatology have been in the subject of Psoriasis to date.
The efficacy of oral tofacitinib was studied in chronic plaque psoriasis in phase 3 randomized controlled trials by Papp et al. in 2015, which showed noteworthy effectiveness in patients with moderate-to-severe psoriasis [4]. In another assessment by Bachelet et al., the Psoriasis Area Severity Index (PASI) responded to oral tofacitinib by 39.5% in 5 mg dose group and 63.6 % in 10 mg dose group at 12 weeks [5]. Tofacitinib in 10 mg dosage was non-inferior to etanercept therapy in moderate-severe cases of plaque psoriasis [5]. For the 5 mg and 10 mg divided frameworks of tofacitinib, adversarial events were similar for tofacitinib and etanercept [5]. Similar improvement was also observed in another study done by Boy et al [6]. However, FDA has not yet approved tofacitinib for psoriasis and its role still remains investigational till date.
Vesely et al. observed substantial improvement in a refractory, severe case of chronic actinic dermatitis to tofacitinib [7]. Infect, same patient was put on multiple immunomodulatory agents prior to tofacitinib administration, which shows zenith of JAK inhibitors, especially tofacitinib [7].
Role of tofacitinib in cutaneous manifestations of polyarteritis nodosa (PAN) was highlighted by Rimar et al. in 2016 [8]. A young adult with chronic symptoms of livedo reticularis and skin nodules, previously treated with azathioprine and methotrexate in remission when showed flaring up of disease showed response to tofacitinib [8].
Seventeen examinations were assessed for the utilization of tyrosine kinase inhibitors in AA. Harel et al observed that local treatment of human and mouse skin with JAK-inhibitors culminated in swift transition of anagen phase of hair cycle and hence hair growth [9]. Core pathogenesis of alopecia areata by interferon gamma and gamma chain cytokine receptors was studied by Xing et al., which also demonstrated the positive role of JAK inhibitors in hair regrowth and turnaround of entrenched AA [10]. These outcomes can clarify the rationale and benefits of tyrosine kinase inhibitors therapy in patients with AA. Sixty-six patients with AA treated by tofacitinib were assessed by Crispin et al. in open -label study in 2016. The impact of tofacitinib was significant. In 32 percent of patients, significant improvement was illustrated in form of regrowth of scalp hair. [11].
Another investigation, including 90 AA patients treated with Tofacitinib, announced clinical response in 77% of cases. In this particular study, response in AA was more marked in comparison to alopecia totalis or alopecia universalis [12]. Additionally, Craiglow et al. displayed the encouraging role of tofacitinib in teenage group cases of AA [13].
In a pilot study, ruxolitinib was given to 12 patients of moderate-to-severe alopecia areata. Striking hair regrowth was seen in 9 patients after 3 to 6 months of treatment with ruxolitinib [14]. Additional investigation on eyebrow and scalp with ruxolitinib brought complete eyebrow hair regrowth and 10% of scalp hair regrowth [15].
Study done by Jabbari et al. illustrated that another tyrosine kinase inhibitor named Baricitinib may be fruitful treatment of AA [16]. Same Baricitinib also attained remarkable amelioration in moderate-to-severe patients of psoriasis and PASI-75 showed revamp after 12 weeks of treatment [17, 18].
JAK inhibitor, tofacitinib showed marked repigmentation in a case of vitiligo, which was attributed to modern discovery in pathogenesis of vitiligo [19]. Similar efficacy of oral ruxolitinib was visualized in a case of coexistent vitiligo and AA by Harris et al [20]. Recent clinical trial by Rosmarin et al. showed successful repigmentation of vitiligo patches with ruxolitinib cream [21].
Reduction in the overall surface area of dermatitis with associated reduction of excoriation and erythema as well as lichenification was detected after Oral tofacitinib usage in recalcitrant atopic dermatitis with 66.6% reduction in AD index [22]. Bissonnette et al. noticed pronounced effectiveness of tofacitinib ointment for atopic dermatitis in a randomized trial [23]. They even considered topical route propitious in atopic dermatitis cases [23].
Ruxolitinib was triumphant against a difficult-to-treat case of chronic mucocutaneous candidiasis as reported by Mossner et al. with IL-6 being used as feedback variable [24].
Cutaneous T cell lymphoma are a subgroup which comes under the broad heading of non-Hodgkin lymphoma which harbors mutations in T cell receptor complex and JAK-STAT signaling pathways. These collectively make tyrosine kinase inhibitors exciting novel weapon against cutaneous T cell lymphoma. However, this prospective functionality needs future trials [25].
Kurtzman et al. delineated foremost utilization of tofacitinib in treatment of refractory dermatomyositis [26]. Likewise, revocation of recalcitrant dermatomyositis was discovered by Hornung et al., when Ruxolitinib was dispensed in a case of myelofibrosis where dermatomyositis was associated finding [27].
Tofacitinib treatment in 10 mg dosage led to full recovery in a case of idiopathic recurrent erythema multiforme as stated by Damsky et al [28]. A multicenter survey exhibited the positive role of ruxolitinib in steroid resistant cutaneous findings of graft-versus-host disease after stem cell transplantation [29]. Reduction in blood eosinophilic count as well as improvement in dermatitis and itching was depicted after treatment with JAK inhibitors in hypereosinophillic syndrome with dermatological manifestations [30].
Chilblain lupus erythematosus, which is a rare autoimmune disorder, was also controlled by ruxolitinib treatment as stated by Wenzel et al [31]. Ruxolitinib also improves quality of life and symptoms in systemic mastocytosis [32]. Even rarer STING vasculopathy which is linked with TMEM1J3 mutation, improved with ruxolitinib in three children [33]. Koga et al. reported therapeutic favorable outcome in patients of palmoplantar pustulosis treated by JAK inhibitors [34].
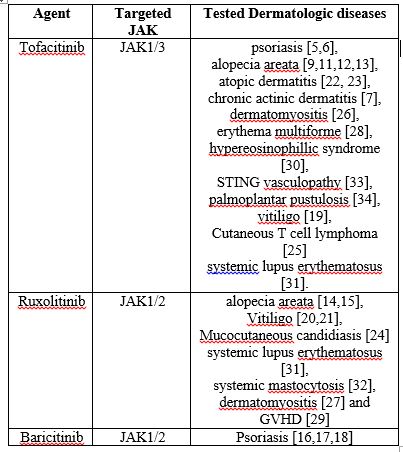
Thus, Tyrosine kinase inhibitors are now a major class of drugs in dermatology treating a plethora of cutaneous conditions. (Table 2)
Though tyrosine kinase inhibitors have many applications in the vast field of dermatology, this group is not free of side effects. Though tyrosine kinase inhibitors used in clinical oncology have predominant skin and cardiovascular toxicities, TKI which are having skin applications do not demonstrate them [35-38].
Ruxolitinib was most commonly associated with urinary tract infection when it was used in treating myelofibrosis [39]. On the other hand, tofacitinib increased the risk of reactivation stage of varicella zoster virus [40]. Response to vaccination could be impeded with tofacitinib and ruxolitinib, which requires healthcare strategist to plan vaccinations before starting treatment with these tyrosine kinase inhibitors [41].
As JAK2 inhibition is more profound with ruxolitinib as compared with tofacitinib, cytopenia, which is primarily mediated by JAK2, is more common with ruxolitinib [42]. However, in a study carried out by Mackay-Wiggan et al. AA dealt with ruxolitinib in therapeutic doses did not demonstrate cytopenia [14].
Neoplasia risk is definitely a reason of apprehension among scientists with the use of Tyrosine kinase inhibitors, albeit theoretically. 1% of renal transplant patients treated with tofacitinib developed post-transplant lympho-proliferative disorder [43]. Nevertheless, no obvious malignancy risk was perceptible when tofacitinib or ruxolitinib were used to treat inflammatory diseases till date [44-47].
Conclusions:
Tyrosine inhibitors have demonstrated response in multiple skin disorders, including Psoriasis, alopecia areata and Vitiligo. Clinical information indicates that the treatment of numerous other dermatological conditions can be achieved through tyrosine hindrance. The approach of Tyrosine inhibitors in dermatology has been met with incredible interest. This class of prescriptions can generously propel the treatment of inflammatory and immune mediated dermatoses. Another exhilarating age of JAK inhibitors/ tyrosine kinase inhibitors is in progress.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
