
Case Report | DOI: https://doi.org/10.31579/2690-4861/594
1 Department of Medical Oncology Haematology, All India Institute of Medical Sciences, Bhopal, India.
2 Pediatric Hematology, Institute of Child Health and Hospital for Children, Madras Medical College, Chennai, India.
3 Department of Hemato-oncology, Artemis Hospital, Gurugram, India.
4 Department of Pathology, All India Institute of Medical Sciences, Rishikesh, Dehradun, India.
5 Department of Medical Oncology Haematology, All India Institute of Medical Sciences, Rishikesh, Dehradun, India.
*Corresponding Author: Gaurav Dhingra, Department of Medical Oncology Haematology, All India Institute of Medical Sciences, Bhopal, India.
Citation: Gaurav Dhingra, Karthik Kumar, Sashikant Singh, Neha Singh, Uttam K. Nath, (2024), Tyrosine Kinase Inhibitor-Associated Aplastic Anemia- A Lethal Adverse Effect and its Management Difficulties, International Journal of Clinical Case Reports and Reviews, 19(5); DOI:10.31579/2690-4861/594
Copyright: Copyright: © 2024, Gaurav Dhingra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 October 2024 | Accepted: 12 November 2024 | Published: 22 November 2024
Keywords: Key words: lethal; hypoplastic marrow; febrile neutropenia; pancytopenia; dasatinib; tyrosine kinase receptor inhibitors; chronic myeloid leukemia (cml)
In the pre-tyrosine kinase inhibitors era, allogenic bone marrow transplant was the treatment of choice for chronic myeloid leukemia-chronic phase (CML-CP). In the tyrosine kinase inhibitor (TKI) era life expectancy of CML-CP patients has matched the general population making it the treatment of choice. TKI is associated with hematological and non-hematological side effects. TKI-associated bone marrow hypoplasia is a rare complication and can be lethal if the patient presents with severe sepsis. Here we describe two fatal cases of TKI-associated bone marrow hypoplasia. The first patient was a 50-year-old newly diagnosed CML-CP patient who had a complete hematological response with BCR ABL quantitative 10.6% at 3 months of Dasatinib therapy. After four and half month’s patient presented with severe sepsis, grade-4 pancytopenia, and hypoplastic marrow and succumbed despite the best supportive care, growth factors, and stoppage of TKI. The second patient was a 50-year-old case of CML-CP refractory to 3 lines of TKI therapy. After 2 months of 4th-line Bosutinib therapy, the patient presented with sepsis, grade 4 pancytopenia, and hypoplastic marrow. This patient also succumbed despite the best supportive care, growth factors, and stoppage of TKI therapy. So TKI-associated bone marrow hypoplasia is a fatal side effect. It should be suspected in patients presenting with grade-4 pancytopenia either after 3 months of 1 st line TKI therapy or before 3 months of TKI therapy in patients on 2 nd or more lines of TKI therapy due to refractory disease.
Chronic myeloid leukemia- Chronic phase (CML-CP) is the most common myeloproliferative neoplasm, representing 15-20% of newly diagnosed leukemia [1]. With the approval of tyrosine kinase inhibitor (TKI) and subsequent introduction of second and third-generation TKI, the life expectancy of CML patients has reached age-matched individuals in the general population [2]. As these TKI need to be continued lifelong till the progression of the disease so drugs drug-associated side effect is an important concern. TKI is also associated with various hematological and non-hematological side effects. Hematological side effects are more common during the first 4-6 weeks of treatment [3]. Hematological toxicity is the major cause of treatment discontinuation or dose reduction [3]. Grade 3-4 neutropenia was seen in 12%, 21%,11%, and 20
Case 1
A woman in her 50s presented to the hematology outpatient department with weakness, arthralgia, and early satiety for 2 months. On examination, the patient had massive splenomegaly (10 cm below the left costal margin) and mild hepatomegaly (2 cm below the right costal margin). There was no lymphadenopathy. Routine investigation showed hyperleukocytosis with left shift and basophilia. BCR ABL qualitative was positive for major transcript (p210). Peripheral smear and bone marrow aspirate were consistent with CMLCP. Karyotying showed 46 XX, t (9;22) (q34; q11). The patient was diagnosed with chronic myeloid leukemiachronic phase with Sokal high risk and ELTS -intermediate risk group. The patient was started on Tab Dasatinib 100 mg once a day and was regularly followed up. After 3 months of TKI therapy, the patient had a complete hematologic response and BCR ABL quantitative was 10.6% on an international scale. So, patient continued on the same treatment. After four and half months of therapy patient presented to the emergency with complaints of weakness, oral ulcers, and pedal edema for 7 days. On examination, the patient had oral candidiasis, pedal edema, and hypotension. Complete blood count showed grade-4 cytopenia (Hemoglobin 60gm/L, WBC - 0.15 ×109/L, and platelet 10 × 109/L). So patient was diagnosed with TKI-induced severe myelosuppression and was managed conservatively with antibiotics, antifungal, growth factor, vasopressor, and blood products and TKI was withheld. The patient recovered from septic shock but given persistent grade-4 cytopenia even after stopping TKI and 12 days of growth factors, bone marrow aspiration, and biopsy were done which were suggestive of severely hypoplastic-marrow with few areas showing small clusters of blast-like cells but were CD34 negative. So, the impression was drug-induced aplastic marrow (Figures 1 and 2). The patient was started on thrombopoietin analogue and danazol. Patient cytopenia persisted with continuous requirement of blood product support. On day 25 of admission, patient again developed septic shock, required mechanical ventilator support, and later succumbed to illness.
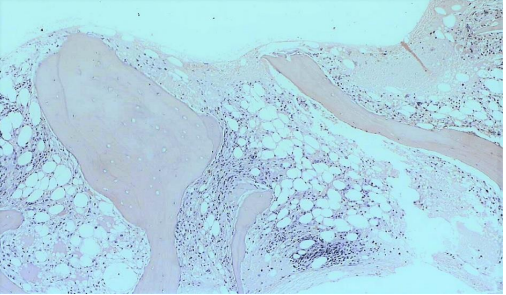
Figure 1: Scanner view showing hypocellular marrow spaces with a predominance of lymphocytes (H&E stain, x40)
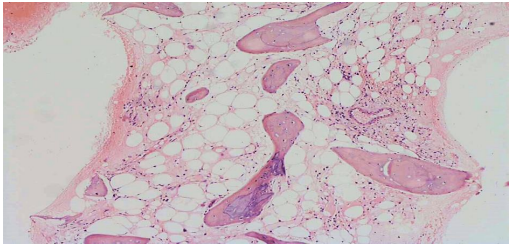
Figure 2: Hypocellular marrow showing predominantly fat and increased number of lymphocytes and plasma cells. No hematopoietic elements are seen. (H&E stain, x100)
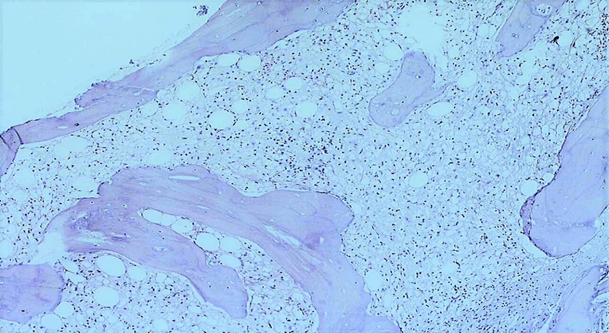
Figure 3: Hypocellular marrow spaces with stromal edema and predominance of lymphocytes (H&E stain, x100)
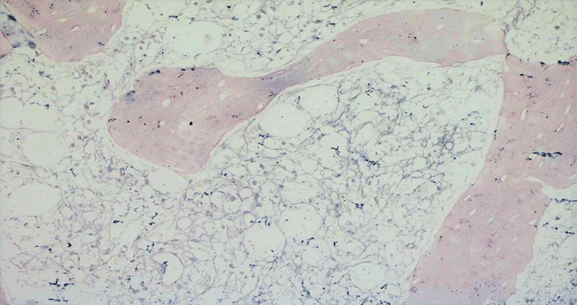
Figure 4: Same case as Figure 3, showing diffusely increased reticulin fibres with extensive intersection – WHO Grade 2 fibrosis (Reticulin stain, x400)
Case 2
A woman in her 50’s was diagnosed with CML-CP with a low sokal score in 2014. She was started on Imatinib therapy. She achieved all the milestones and achieved MMR at 12 months of therapy and maintained MMR till May 2018. In 2018 she relapsed so bone marrow aspirate, karyotyping, and tyrosine kinase mutation studies were done which showed disease in the chronic phase with no additional cytogenetic abnormality and no evidence of TKI resistant mutation respectively. The patient was started on Dasatinib therapy. She again achieved MMR. In October 2020 she relapsed again and on repeat evaluation showed disease in the chronic phase with no additional cytogenetic abnormality and no evidence of TKI-resistant mutation. So, she was started on Nilotinib but failed to achieve a haematological response at 3 months so was counseled regarding Ponatinib and bone marrow transplant but due to financial constraints was started on generic Bosutinib in August 2021. In October 2021 the patient was admitted with complaints of fever and breathing difficulty. CECT chest showed consolidation in right upper lobe and complete blood count showed grade 4 cytopenia (Hemoglobin 72 g/L, Total leukocyte count -0.2 × 109/L, and platelet 20 × 109/L). Due to breathing difficulty patient was put on a mechanical ventilator and started on IV empirical antibiotics, antifungal, growth factors, and other supportive care with blood products. TKI was withheld considering drug-induced cytopenia. In view of persistent cytopenia, on Day 7 of admission, the patient was started on subcutaneous Injection romiplostim(weekly). The patient clinical condition progressively worsened and continued to have persistent grade 4 pancytopenia requiring daily support with platelets. So, on day 12 of admission, bone marrow aspiration and biopsy was done which was suggestive of severely hypoplastic marrow with grade 2 fibrosis on reticulin stain. So, impression was Hypocellular marrow with grade 2 fibrosis (Figure 3 and 4). Patient clinical condition further worsened in spite of escalation of antibiotics and antifungal and she developed refractory septic shock and on day 16 succumbed to her illness.
In CML patients tyrosine kinase-associated bone marrow hypoplasia can occur for two reasons. Firstly, delayed recovery of normal hemopoietic cells during the first 3 months of the start of therapy: In patients with CML, myelosuppression occurs after 4-6 weeks of the beginning of TKI therapy due to reduction of BCR-ABL positive leukemic stem cells and delayed recovery of prolonged suppressed normal hemopoietic stem cells [3]. So early myelosuppression during the first 3 months is an indicator of the efficacy of TKI therapy. However, this myelosuppression can be grade 3-4 and can even lead to prolonged bone marrow hypoplasia in patients who are receiving TKI as 2nd line or 3rd line therapy due to resistant disease [3,7-11]. Secondly, True therapy-related hypoplasia, occurs after 3 months of TKI therapy in responding patients due to drug-associated myelosuppression.
All TKI are associated with myelosuppression; however, dasatinib is associated with the greatest hematologic toxicity, which also depends on dose and schedule [3]. In patients on dasatinib, grade 2 to 4 neutropenia or thrombocytopenia occurs in 87% of patients in 1st 90 days and is also associated with recurrence of cytopenia after 90 days in 88% of patients [12]. It is also known that dasatinib inhibits the proinflammatory function of mature neutrophils [13]. So, myelosuppression and anti-inflammatory action of dasatinib can cause severe infections in CML patients.
So, case 1, had true therapy-related bone marrow hypoplasia as it occurred at 4 and 1/2 months after optimal response with the normal count at 3 months of dasatinib therapy. Secondly, due to myelosuppression and anti-inflammatory action of dasatinib, our patient presented with severe sepsis. In case 2, prolonged pancytopenia with hypoplastic marrow occurred after 8 weeks of starting bosutinib as 4th line therapy in imatinib, dasatinib, and nilotinib-resistant disease. So prolonged cytopenia could be due to prolonged suppression of normal hemopoietic stem cells due to resistant disease.
Management of TKI-associated myelosuppression requires withholding TKI in grade 3-4 cytopenias and starting at a lower dose when cytopenia improves to less than grade 3. Recurrent grade 3-4 cytopenia require a change of therapy but there is a chance of recurrence due to cross intolerance to hematological side effects [3].
Management of TKI-associated bone marrow hypoplasia is still not well defined and this condition can be lethal if not addressed on time. Below are the case reports of CML-CP which we could find from a literature search who developed TKI-associated bone marrow hypoplasia. In two cases reported by Ramdial et al., case 1 developed pancytopenia and bone marrow hypoplasia after 8 months of imatinib therapy, which required discontinuation of treatment for two months. The patient was later started on Dasatinib due to 95
Bone marrow aplasia is a fatal rare adverse effect of TKI in CML-CP patients. It should be suspected in patients who develop prolonged pancytopenia on TKI as 2nd or 3rd line for resistant disease or in patients who develop prolonged pancytopenia on TKI after achieving optimal response at three months of therapy. Also, TKI-associated bone marrow hypoplasia is associated with prolonged and repeated discontinuation of TKI therapy, which is associated with either suboptimal response or disease progression. Hypoplasia can recur if the same TKI is continued or another TKI is started due to cross intolerance. Few cases can recover with growth factors and immunosuppressive agents but the ultimate treatment of TKI-associated bone marrow hypoplasia is an allogeneic bone marrow transplant due to the high incidence of recurrence or cross intolerance of hematological complications.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
