
Case Report | DOI: https://doi.org/10.31579/2640-1045/106
MD Assistant Professor of Medicine Department of Medicine, Division of Cardiology Thomas Jefferson University Hospital, USA.
*Corresponding Author: Drew Johnson, 925 chestnut street, Mezzanine Philadelphia, PA 19007, USA.
Citation: Drew Johnson (2022). Type 1 Brugada pattern induced by DKA. Endocrinology and Disorders. 6(1): DOI:10.31579/2640-1045/106
Copyright: © 2022 Drew Johnson, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 September 2021 | Accepted: 15 December 2021 | Published: 04 January 2022
Keywords: brugada syndrome; genetic testing; antiarrhythmic drugs
A 25-year-old man with a past medical history of type 1 diabetes presented to the emergency department with 2 days of progressive abdominal pain, nausea, and vomiting after stopping insulin. His heart rate was 125 and the respiratory rate was 26. The glucose was 832 mg/dl, the potassium was 6.6 mmol/L, the beta-hydroxybutyrate was 111.8 mg/dl, and the pH was 6.95.
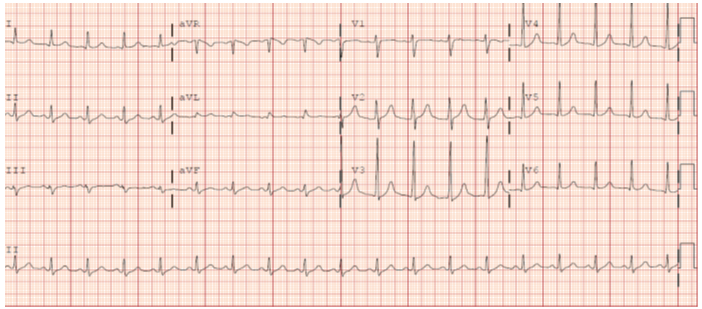
A 25-year-old man with a past medical history of type 1 diabetes presented to the emergency department with 2 days of progressive abdominal pain, nausea, and vomiting after stopping insulin. His heart rate was 125 and the respiratory rate was 26. The glucose was 832 mg/dl, the potassium was 6.6 mmol/L, the beta-hydroxybutyrate was 111.8 mg/dl, and the pH was 6.95. The electrocardiogram (ECG) showed sinus tachycardia with anterior ST segment elevations, and a right bundle branch block pattern, consistent with Brugada type 1 pattern (Panel A). On review, his family history was unremarkable. The patient did have a history of three prior vagally-medicated syncopal episodes. The remainder of his history and physical exam were unremarkable. He was diagnosed with diabetic ketoacidosis and was given IV fluids and insulin. Three hours later the glucose was 318 mg/dl, the potassium was 4.5 mmol/L, and the pH was 7.18. A repeat ECG (Panel B) showed sinus tachycardia with resolution of the previously noted ST changes and right bundle branch block. The patient was diagnosed with Brugada type 1 pattern on his ECG. He was counseled about avoidance of excessive alcohol intake, aggressive treatment of fevers with antipyretics, counseled to treat future syncopal events as an emergency, asked to visit Brugadadrugs.org to review what medications are safe in Brugada syndrome, and scheduled for outpatient electrophysiology follow up for additional evaluation. Until he can undergo genetic testing for Brugada syndrome the patient is assumed to have Brugada syndrome.

Brugada syndrome is divided into three types. Type 1 is diagnosed when there is >2 mm ST segment elevation in ≥1 of the right precordial leads either V 1 or V2, positioned in the 2nd, 3rd, or 4th intercostal space occurring either spontaneously or after provocative drug test with intravenous administration of class 1 antiarrhythmic drugs [1]. Brugada syndrome is a genetic condition that was first described in 1992 that increases patient's risk for sudden cardiac death [2]. The syndrome is most commonly caused by a mutation in the sodium channel SCN5A gene [3]. However, ECG and clinical manifestations are variable. ECG manifestations in particular may be intermittent. There are known triggers to finding a Brugada pattern on ECG including certain medications, fever, and metabolic conditions such as diabetic ketoacidosis. However, previous reports have shown that not all patients with documented Brugada pattern under severe metabolic derangement are able to demonstrate it spontaneously or with provocation testing [4]. There is currently no consensus about the management of patients with an incidentally noted Brugada pattern in the setting of a severe metabolic disturbance. The diagnostic criteria for Brugada syndrome include either a spontaneous pattern or one that is unmasked with pharmacologic provocation testing (specifically Class I anti-arrhythmics). We plan to treat this patient the same way we treat our other patient with Brugada syndrome.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
