
Research Article | DOI: https://doi.org/10.31579/2767-7370/100
1Pharma collage of Health Science.
2Tula General Hospital, Hawassa City Administration.
3Sidama Regional Health Bureau.
*Corresponding Author: Derese Desalegn Buta, 1Pharma collage of Health Science, Sidama Regional Health Bureau.
Citation: Kalkidan B. Bekele, Derese D. Buta, (2024), Tuberculosis treatment success rate and associated factors among tuberculosis patients attending health centers found in Hawassa city, Sidama Ethiopia: A facility based cross sectional study 2023, J New Medical Innovations and Research, 5(4); DOI:10.31579/2767-7370/100
Copyright: © 2024, Derese Desalegn Buta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2024 | Accepted: 22 April 2024 | Published: 03 May 2024
Keywords: factors; Ethiopia; sidama regional state; treatment success rate
Background: Tuberculosis continued to be as serious public health problem global. It has been registered as the primary cause of illness, the third reason for admission and the second cause of death and that has been as challenging disease in Ethiopia.
Objective: The study was designed to determine tuberculosis treatment success and associated factors among TB patients in health centers of Hawassa city, Sidama Ethiopia.
Methods: Facility based cross-sectional study was conducted September 20 to 26/2023 by reviewing all available medical records of TB patients those enrolled on anti-TB treatment between September 2021 and June 2023. Data were collected by using structured check list and entered in to Epi data version 7.2 and analyzed using SPSS version 22. The binary and multiple logistic regressions were used to assess possible associations. The statistical significance between variables were measured using adjusted odds ratios and P value <0.05 with 95% confidence interval.
Result: A total of 445 patients with a median age of 25(IQR: 20-35 years) were included. The overall rate of treatment success in current study was 95.7 % (CI 95%: 93%, 97%). The odds of successful treatment outcome were higher among patients in age group 15-24years (AOR=5.4, 95% CI: 1.14-26.0), having pre-treatment weight of 40-54.9kg (AOR=2.4, 95% CI: 0.2-24.583), and >/=55kg (AOR=2.02, 95% CI: 0.59-6.93) and being new TB patient (AOR=2.01, 95%CI: 0.35-9.90).
Conclusion and Recommendation: Rate of successful TB treatment outcome was obtained as an acceptable and should be maintained and further improved by designing appropriate monitoring and evaluation strategies.
Background: Tuberculosis is a infectious disease that caused by Mycobacterium tuberculosis causative agent and mostly affects the lung and can result in pulmonary tuberculosis or extra pulmonary tuberculosis within other organs. It is one among the top 10 most common causes of mortality worldwide, making it a serious public health concern. If left untreated, the illness, most frequently affects the lungs, can be fatal [1, 2].
Tuberculosis is transmitted from person to person through the air. People who have lung TB spread the germs into the air when they cough, sneeze, or spit. It just takes a few of these germs to infect a person by inhalation. It is believed that approximately 25% of the world's population carries a TB infection; however, the majority of individuals do not progress to acquire TB disease and a small percentage may be able to overcome the infection. It cannot be spread by those who are infected but not (yet) ill with the disease. The lifetime chance of developing tuberculosis is 5–10% for those with TB infection. Individuals with weakened immune systems, including those with HIV, diabetes, malnutrition, or tobacco use, are more susceptible to illness. The symptoms (cough, fever, sweats at night, or weight loss) of active tuberculosis may not show up for several months. This can cause a delay in seeking medical attention and spread the infection to other people. Within a year of coming into close contact, a person with active TB can infect five to fifteen more persons. Nearly all HIV-positive TB patients will die without treatment, and the average percentage of HIV-negative TB patients who die is 45% [3, 4] .
According to a 2017 WHO estimate, 1.6 million people died from tuberculosis and approximately 10 million people were sick. The regions with the highest fatality rates, South East Asia and the Western Pacific, accounted for about 56% of the cases, while Africa accounted for 29% [5]. Ethiopia has an estimated TB incidence of 164 per 100,000 people, making it one of the 30 nations with the highest burden of TB and Multi Drug Resistance Tuberculosis (MDR TB). Among patients who had previously received treatment, the nationwide frequency of MDR-TB climbed from 1.6% in 2005 to 17.8% in 2014 [6].
Statement of problem
10.4 million Incident cases worldwide were expected to have occurred in 2015, of which 6.1 million were notified and 1.4 million resulted in deaths. Consequently, the most recent strategy, "End TB," was created with the Sustainable Development Goals (SDG) in mind. By 2025, 90% of cases would be detected and treated successfully, according to the plan. As per the 2020 worldwide benchmarks of the "End TB Strategy," a 4-5% annual decrease in the prevalence of tuberculosis is expected. Ethiopia's TB case detection rate is extremely low in comparison to the World Health Organization's (WHO) goal of identifying all infectious TB cases. Despite all efforts, Ethiopia still being one of the 30 nations with the highest TB burden. Numerous studies have demonstrated that Ethiopia's tuberculosis treatment success rate is below the threshold of 90%. For instance, a 12-year meta-analysis on the success rate of tuberculosis treatment and related factors conducted in 2018 found that Ethiopia's overall pooled TB treatment success rate was 86%. But the results also were differ in each regions; Addis Ababa (93%), Oromia (84%), Amhara (86%), Southern Nations and Nationalities (83%), Tigray (85%), and Afar (86%), were the regions with the highest success rates for tuberculosis treatment. Retreatment cases, advanced age, HIV co-infection, and living in a remote area were the most often found risk factors for poor TB treatment outcomes [7,8].
Significance of the study
In order to identify tuberculosis treatment success rates and associated factors that reinforce better treatment outcomes and for further resource planning, prioritization and distribution. The findings of the current study will be the availed evidence to health centers, regional health bureaus, policy makers and non-governmental organizations (NGOs).
Objectives
Study area: The study was conducted in Hawassa city, the capital city of Sidama region, with population of 436,992 according to projections of the central statistics of Ethiopia in 2020 G.C, and with annual growth rate of 4.8%. The City is divided in to eight sub cities and thirty two kebele/the smallest administrative unit. It has four governmental hospitals and thirteen health centers, all the facilities provide TB treatment services according to Sidama regional health bureau report. The study was conducted on three health centers (Alamura, Millennium and Adare health centers) those were chosen by lotterymethod.
Study design and period: Facility based cross-sectional study was conducted from September 20-26, 2023 by reviewing all the available data on health center medical records of TB patients.
Source population: The source population were patients registered for treatment of TB in health centers of Hawassa city from September, 2021 – June, 2023.
Study population: The study population were all TB patients treated for TB in selected health centers in Hawassa, from September, 2021- June, 2023.
Inclusion criteria: All TB patients whose records were complete and age 15 years and above.
Exclusion criteria: Transfer out cases and TB patients whose records not complete were excluded.
Sample size determination
Single population proportion formula was utilized to calculate the sample size for the first objective.

n=384
Adding 10% contingency sample size becomes 422.
Where; n=sample size
Z=standard normal deviation
d=desired degree of accuracy
p= (50%)
Sample size for the second objective was calculated by using double population proportion using with Epi Info version7.2 (See Table 1).
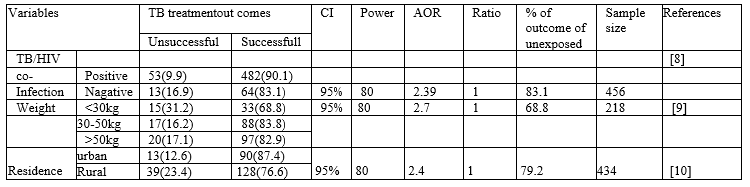
Table 1: Sample size determination considering factors associated with TB treatment success, Hawassa City 2023
From the calculated sample sizes done by using different variables, 456 is the largest value and was taken as the final sample size.
Sampling technique and procedure
Systematic random sampling technique was used to select study participants from the register within the health centers. From the total 13 health centers in the city 3 were selected by lottery method then sampling interval (k) was determined by dividing the expected number of cases in a three year period of the previous year to the total sample size which is 3 (See Figure 1).
Study variables
Dependent variable:
Independent variables:
Operational definition
Treatment outcomes
The treatment outcome was divided into seven categories according to NTLCP guideline. These categories were as follows:
Cured: Is defined as a patient initially bacteriologically confirmed and completed the treatment without the evidence of treatment failure and three or more consecutive cultures taken at least 30 days apart are negative after the intensive phase.
Completed treatment: Refers to finishing treatment but without bacteriology result at the end of treatment.
Failure: Remaining smear positive at first months despite correct intake of medications.
Defaulted treatment: Patients who interrupted their treatment for two consecutive months or more after registration.
Died: Who died from any cause during the course of treatment
Transfer out: Patients whose treatment results are unknown due to transfer to another health facility.
Successfully treated: A patient who completed treatment plus cured.
Unsuccessful treatment: The sum of lost to follow up, death, defaulted.
Smear Positive Pulmonary TB
It refers to the following: a patient with at least two sputum specimens which were positive for acid-fast bacilli (AFB) by microscopy or a patient with only one sputum specimen which was positive for AFB by microscopy, as well as chest radiographic abnormalities consistent with active pulmonary TB.
Smear Negative Pulmonary TB
It refers to the following: a patient with symptoms suggestive of TB with at least two sputum specimens which were negative for AFB by microscopy and with chest radiographic abnormalities consistent with active pulmonary TB (including interstitial or miliary abnormal images) or a patient with two sets of at least two sputum specimens taken at least two weeks apart and which were negative for AFB by microscopy and radiographic abnormalities consistent with pulmonary TB and lack of clinical response to one week of broad spectrum antibiotic therapy.
Extra pulmonary TB (EPTB)
This included tuberculosis of organs other than the lungs, such as lymph nodes, abdomen, genitourinary tract, skin, joints and bones, and meninges. Diagnosis of EPTB was based on fine needle aspiration cytology or biochemical analyses of cerebrospinal fluid or histopathological examination or strong clinical evidence consistent with active extra pulmonary tuberculosis, followed by a decision of a clinician to treat with a full course of anti-tuberculosis chemotherapy. A case of TB is a patient in whom tuberculosis has been confirmed bacteriologically or diagnosed by a clinician. The following are case definitions:
New case (N): Refers to a patient who never had treatment for TB or has been on previous anti-TB treatment for less than four weeks.
Relapse (R): Refers to a patient declared cured or whose treatment was completed of any form of TB in the past who reports back to the health service and is now found to be AFB smear positive or culture positive.
Treatment failure (F): Refers to a patient who, while on treatment, is smear positive at the end of the fifth month or later, after commencing. It also includes a patient who was initially sputum smear negative but who becomes smear positive during treatment.
Return after default (D): Refers to a patient previously recorded as defaulted from treatment and returns to the facility with smear positive sputum.
Transfer-out (T): A patient who started treatment in one treatment unit and is transferred to another treatment unit to continue treatment.
Chronic (C): A TB patient who remains smear positive after completing re treatment regimen.
Others (O): A patient who does not fit in any of the above mentioned categories.
Data collection tools and procedures
Medical records were reviewed by using a structured data collection questionnaires prepared in English. A treatment outcome was evaluated in accordance with the National Tuberculosis and Leprosy Control Program (NTLCP) adopted from the WHO. Data were collected by health officers and nurses by using questionnaires those include patient information like socio- demographic characteristics and clinical variables were obtained from TB medical records and the registration book. Body mass index was measured by using patient weight (kg) and height (M), then dividing weight by height square.
Data quality assurance
Check list was prepared after reviewing different literatures to record the necessary information from the patient cards and registration book. Prior to the start of data collection one day training was given for the data collectors about study objectives and how to fill the check list. During data collection close super vision was carried out by supervisor and principal investigator. Before receiving the filled checklist from each data collector the Supervisor checked to identify incomplete checklist.
Data processing and analysis
Data were checked for completeness, edited, cleaned and entered in to Epi data version 7.2, and exported to SPSS version 22 for analysis. Appropriate descriptive statistics such as mean with standard deviation (SD), median with inter quartile range (IQR) and frequencies with percentages were used to describe the study population in relation to relevant variables. Bivariate and multivariate analysis with 95% confidence interval were employed to infer associations between the independent and dependent variables. Binary logistic regression was used to calculate the crude odds ratio (COR) with 95% confidence interval. Each variable was entered into a logistic regression model so as to determine the presence of statistical significant association with the outcome variable. Multicollinearity was checked through variance inflation factor (VIF). All the explanatory variables with a p-value <0>
Socio-demographic characteristics of study participants
The documents of 444 TB patients were reviewed. More than half of these TB patients 265(59.7%) were male. The median age of study participants was 25(IQR: 20-35years). About 191(43%) of the participants were in the age range between 25-44years and 188(42.3%) were in the age range between15-24. The weight of TB patents ranged from 15-98kg with mean (±SD) weight of 50.8(±11.5) kg.
Clinical characteristics
Most of the attendants (94%) were new TB cases. 151(34%) of the patients were smear positive PTB Patients, 32 (7.2%) found to be HIV positive of whom 21(61.8%) and 22(64.7%) were on Cotrimoxazole preventive therapy (CPT) and ART respectively.
Among smear positive PTB patients at the beginning of the treatment 145(96.0%), 131(86.8), 145(96%) were smear negative at second, fifth and seventh months of treatment respectively. Majority of patients, 233(52.5%) had BMI less than or equal to 18 at the time they started treatment.
Treatment outcome of patients on anti-TB therapy
Among the TB patients included with the current study, 146(32.9%) were cured, 279(62.8%) had completed their treatment, 11(2.5%) were died, 4(0.9%) were defaulted and 4(0.9%) were lost to follow up (See Figure 2).
Factors associated with TB treatment success
The overall rate of treatment success (cure and treatment complete) in this study was 95.7%. The rate of treatment success was higher among males (95.8%) than females (95.6%) and there was also more positive outcome whose patients from urban setting (95.8%) than patients from rural setting (94.1%). The treatment success rate were 98.0%, 97.1%, 93.2% among PTB+, PTB-, EPTB patients, respectively (See Figure 3).
In the bivariate analysis, variables with p-value of <0 AOR=5.4,>/= 45 years. New TB patients had twice higher odds of (AOR= 2.01, 95%CI: 0.359-9.907) having treatment success than their counter parts. Similarly, the odds of treatment success were 2.4 (AOR=2.407, 95% CI: 0.236-24.583) times higher among patients with pre-treatment weight range of 40-54.9kg than >/= 55kg (See Table 2).
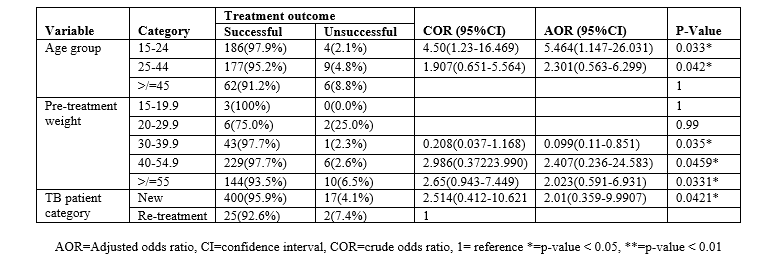
Table 2: Multivariate analysis of treatment outcome with socio-demographic and clinical characteristics of TB patients attending health centers found in Hawassa city, Sidama, Ethiopia 2023.
From the current study, the overall rate of treatment success of the TB patients was found to be 95.7 %( 95%CI: 93%, 97%) which is consistent with the findings reported from Harar town (92.5%), Infraz (95%), Turkey (92.6%), Addis Ababa (94.6) and the WHO 2030 international target of >90% [6, 11-14].
However, it is higher than national report of Ethiopia (85%) and other previous studies conducted in Ethiopia those reported with treatment success ranging from 43.3% in Hosanna to 81% in Afar [9, 15-20] . This high treatment success rate in current study might be due to good implementation of DOTs strategy and due to the exclusion of transfer out patients. Another possible explanation could be since the study was conducted in health centers which are situated in the nearby catchment of the patients there was rare probability of treatment default (n=4) and failure (n=4) rate. Similarly the reason might be that the current study was conducted among urban dweller compared to others where more rural community with lack of knowledge about TB, inappropriate health seeking behavior and stigma towards TB also[21]. This study also revealed default, death and lost to follow up rate of 0.9%, 2.5%, and 0.9% respectively. This constituted an overall unsuccessful TB treatment outcome rate of 4.7% which was lower than 5.4% ,10.8%, and 14.8% unsuccessful treatment outcome reported from Addis Ababa, Tigray region and Southern Ethiopia[6, 22, 23] that could be due to difference in duration of study period, sample size and study setting. Poor adherence to anti-TB treatment due to treatment failure, lost to follow up and irregular treatment might lead to more severe illness, treatment failure, relapse, drug resistance and even death. Defaulting and irregular anti-TB drug intake presented problem and worry for both the patient and the community and needed to be addressed appropriately. The finding showed that there is significant association between age and successful treatment outcome; patients with age category 25-44 are 5.4 times more likely to have successful treatment outcomes than patients whose age was greater than 45 year old. This finding was align with the result obtained from the studies done in Northern Ethiopia prisons, Tigray region and Arbaminch, Southern Ethiopia [28, 34, 36]. This might be due to the reason older patients may have the concomitant disease and psychological deterioration. The other significantly associated factor in this study was pre-treatment weight of 40-54kg and >/= 55kg both are 2 times more likely to have successful treatment outcome than their counterparts. This finding is supported by studies done in Harar town, India and Uganda [12, 37, 38]. Study in Addis Ababa revealed that body weight at initiation of anti-TB treatment (<35kg)was significant risk factor for death during anti-TB treatment period [39]. The reason might be that patients with good weight may tolerate the drug side effects and that can support them to have good treatment outcome. Similarly, the likelihood of TB treatment success among new TB patients was twice as likely as their counter parts to have successful treatment outcome. This finding was coinciding with studies conducted in Arsi zone, Somalia, Nigeria, and Turky [13, 32, 40, 41]. The possible reason might be that those newly diagnosed and enrolled patients may have low probability of drug resistance and a good probability of completing the required treatment.
Strength and limitation of the study
The strengths are there was a good chance that obtaining all patient information regarding anti-TB therapy, barring cases of transfer out. As a result, the results can accurately reflect how well TB patients responded to treatment.
The fact that this study relied on secondary data from patient registrations and medical records was one of its limitations. Thus, it's possible that crucial socio-demographic and economic variables like monthly income, style of care, educational attainment, employment status, and elements connected to the health system won't be evaluated to ascertain how they link to the success of therapy. As the study is institution based it is difficult to generalize for the whole community.
Strength and limitation of the study
The strengths are there was a good chance that obtaining all patient information regarding anti-TB therapy, barring cases of transfer out. As a result, the results can accurately reflect how well TB patients responded to treatment.
The fact that this study relied on secondary data from patient registrations and medical records was one of its limitations. Thus, it's possible that crucial socio-demographic and economic variables like monthly income, style of care, educational attainment, employment status, and elements connected to the health system won't be evaluated to ascertain how they link to the success of therapy. As the study is institution based it is difficult to generalize for the whole community.
The treatment outcome of TB patients at the study area was satisfactory compared to other studies and align with WHO and national TB and leprosy control program standard. The treatment outcome was significantly associated with age, pretreatment weight and type of TB patient.
Frequent supportive supervision of health centers should be done to maintain the obtained treatment success rate and achieve even better. Appropriate health education programs for patients with high risk of unsuccessful treatment outcome should be carried out. Further prospective studies are needed to identify other potential socio-demographic and behavioral factors that could affect the treatment outcome of TB patients.
TB Tuberculosis
MDR-TB Multi drug resistant tuberculosis
AFB Acid fast bacilli
HIV Human immunodeficiency virus
AIDS Acquired Immunodeficiency Syndrome
WHO World health organization
SDG sustainable development goal
DOTS Directly observed treatment short course
NTCP national tuberculosis and leprosy control program
PLHIV people living with human immunodeficiency virus
COPD Chronic obstructive pulmonary disease
PTB pulmonary tuberculosis
EPTB Extra pulmonary tuberculosis
BC-PTB Bacteriologically confirmed pulmonary tuberculosis
CI confidence interval
OR Odds ratio
AOR Adjusted odds ratio
Ethical clearance
Ethical clearance was obtained from Institutional Review Board (IRB) of Pharma College of Public health and permission was granted from Sidama Regional Health Bureau, Hawassa City Administration Health department and sample health centers after discussing and clarifying the objectives of the study and its contributions towards improving tuberculosis program.
Conflict of Interest:
Both researchers have done each step of current study with in agreement and do not have any conflict of interest regarding it.
Above all, we thank the Almighty God for all. We also would like to acknowledge Pharma College, department of public health, for giving us the opportunity to do this thesis work. We would also like to extend our deepest gratitude to chief executive officers of the health centers and tuberculosis clinic heads for their collaboration and giving all information to data collectors. Our sincere gratitude goes to data collectors and supervisors of the data collection.
Authors’ details and contribution for the current study
KBB: Kalkidan Birhanu Bekele (BSc, MPH), staff at Tula General Hospital, Sidama Regional Health Bureau, post graduate student at Pharma College of Health Science
Idea generating, developing research proposal and data collection tool, train data collectors and supervisors, supervise data collection steps, did data cleaning, entry, analysis, result writing and finalizing the document. Prepare manuscript.
DDB: Dr Derese Desalegn Buta (MPH, MBA, PhD)
Sidama Regional Health Bureau, Health Extension Program and Primary Health Care Unit advisor, Senior Public Specialist and health consultant, Researcher, student research advisor and lecturer, Phama College of Health Science:
Supervises each and every step of proposal development, advice and test data collection tool, data collection step, analysis and result writing part. Comment and finalize manuscript development.
Availability of data and materials
The datasets produced and/or analyzed throughout the current study are not openly accessible due to institutional regulation but would be obtainable from the authors for reasonable request.
Funding
There was no financial support for the current study obtained from anywhere and the researchers tried to cover it accordingly.
Supplementary files:
Supplementary files attached separately those addresses the following areas
Supplementary file 1: Participant information sheet and informed consent form
Supplementary file 2: Data collection tool of current study
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
