
Research Article | DOI: https://doi.org/10.31579/2692-9759/140
1Division of Kidney and Hypertension, Lenox Hill Hospital-Northwell Health/Zucker School of Medicine, New York, NY 10075, USA
2Department of Obstetrics and Gynecology, Lenox Hill Hospital-Northwell Health/Zucker School of Medicine, New York, NY 10075, USA
3Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Lenox Hill Hospital-Northwell Health/Zucker School of Medicine, New York, NY 10075, USA
*Corresponding Author: Maria V. Devita, Division of Kidney and Hypertension, Lenox Hill Hospital-Northwell Health/Zucker School of Medicine, New York, NY 10075, USA.
Citation: Valerie Barta, Nimesh Shah, Stephanie Baum, Christina Zottolla, Maria V. DeVita, et al, (2024), Trends in Peripartum NT-ProBNP levels in Patients with Hypertensive Gestational Syndromes: A Prospective Cohort Study, Cardiology Research and Reports, 6(5); DOI:10.31579/2692-9759/140
Copyright: © 2024, Maria V. DeVita. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 August 2024 | Accepted: 13 August 2024 | Published: 22 August 2024
Keywords: hypertensive gestational syndromes; brain natriuretic; nephrology literature
Hypertensive gestational syndromes (HGS) are increasingly prevalent as more women are delaying pregnancy. The typical high sodium, fat and carbohydrate Western diet has resulted in earlier development of obesity, diabetes, hypertension in premenopausal women. These co-morbidities further increase the number of pregnancies complicated by disorders of hypertension. The importance of screening patients for HGS is well known and treatment guidelines have been established, however there remains a paucity of data on clinical predictive and diagnostic indicators of HGS, particularly in nephrology literature. There is a need to deepen our understanding of the underlying pathophysiology in these patients. Through this understanding we can direct our focus on improving predictive and diagnostic methods of HGS in order to better serve our evolving patient population.
Hypertensive gestational syndromes (HGS) are increasingly prevalent as more women are delaying pregnancy. The typical high sodium, fat and carbohydrate Western diet has resulted in earlier development of obesity, diabetes, hypertension in premenopausal women. These co-morbidities further increase the number of pregnancies complicated by disorders of hypertension. The importance of screening patients for HGS is well known and treatment guidelines have been established, however there remains a paucity of data on clinical predictive and diagnostic indicators of HGS, particularly in nephrology literature. There is a need to deepen our understanding of the underlying pathophysiology in these patients. Through this understanding we can direct our focus on improving predictive and diagnostic methods of HGS in order to better serve our evolving patient population.
Serum N-terminal brain natriuretic peptide (NT-proBNP) levels rise in response to cardiac ventricular myocyte stretch. NT-proBNP is used in clinical practice to evaluate cardiac strain of various etiologies. Pregnancy is characterized by complex physiological changes of the cardiovascular system including a 40-50% increase in blood volume which increases left ventricular mass, left ventricular end diastolic pressure and cardiac output.1 Interstitial water and sodium are increasingly retained towards the end of pregnancy and there is a 14
We assessed the significance of NT-proBNP elevations as related to ascending degrees of cardiac strain induced by cHTN, GH and PEC in the immediate peripartum period. We sampled peripartum serum NT-proBNP levels, drawn once within 24hrs antepartum and again within 24hrs postpartum, of healthy control patients, compared to those of patients with cHTN, GH and PEC. We hypothesized that patients with hypertensive disorders of pregnancy will have higher peripartum NT-proBNP levels as compared to normal controls, due to hemodynamic stressors of labor, particularly in preeclamptics as this vasoconstrictive pro-inflammatory state confers significantly higher degrees of cardiac strain. With this information we can better risk stratify our peripartum patients with HGS, helping differentiate evolving PEC from other more benign conditions such as exacerbation of cHTN, GH or white-coat HTN.
This is a prospective observational cohort study conducted from April 2018 to February 2019 at Lenox Hill Hospital Northwell Health, New York, NY. Informed consent was obtained from patients for two separate blood draws of serum NT-pro BNP levels during their hospitalization for delivery. Patient data including age, race, parity, Body Mass Index (BMI), gestational age at delivery, family or personal history of preeclampsia, route of delivery, pre pregnancy weight, serum creatinine, aspartate and alanine transaminases (AST, ALT), hemoglobin, platelet count, uric acid, lactate dehydrogenase, urine analysis, urine protein to creatinine ratio were collected from electronic medical records. All patient data was processed in the HIPPA compliant REDCAP data storage system.
Inclusion criteria were all pregnant individuals between the ages of 18 to 55 admitted at LHH for their delivery at term as defined as gestational week 32 to 42 as normal control and/or with pregnancy related hypertensive disorders PEC, GH and CH. Patients with known heart failure, heart disease or prior cardiac surgery were excluded, as were patients with COPD, history of pulmonary embolism, diabetes mellitus, severe autoimmune disease, anti-phospholipid syndrome and those with cognitive impairment or otherwise unable to provide informed consent. Patients who delivered pre-term, or with intrauterine fetal death not associated with hypertensive disorder of pregnancy were also excluded.
Chronic hypertension was defined as requiring antihypertensive medications prior to conception, or systolic blood pressure (SBP) >140 mmHg or diastolic blood pressure (DBP) >90 mmHg known to predate conception or detected before 20 weeks gestation. Gestational hypertension was defined as SBP >140 mmHg or DBP >90 mmHg on two or more measurements at least four hours apart, occurring after 20 weeks of gestation, without concomitant proteinuria. Preeclampsia was defined as the new onset of hypertension (SBP ≥140mmHg and/or diastolic blood pressure ≥90 mmHg on two measurements at least 4 hours apart) plus proteinuria (24hr urine protein =/> 300mg, urine protein to creatinine ratio =/> 0.3 or 2+ proteinuria on urine dipstick if former measurements unavailable, without a concomitant urinary tract infection or with signs of severe PEC including thrombocytopenia, renal impairment, elevated liver enzymes, pulmonary edema, unexplained headache not relieved by medication or visual disturbances.16
Antepartum blood samples of 5-10 ml were obtained using standard sampling tubes within 24hrs prior to delivery, postpartum blood samples were drawn within 24hrs after delivery. Serum NT-proBNP analyzed by an electro chemiluminescence immunoassay “ECLIA” at our institute’s inpatient laboratory. When used with the recommended cut-offs the Elecsys proBNP II STAT assay used yields negative predictive values ranging from 97.8 to 100
A total of ninety-seven patients were enrolled. Thirty-five normotensive controls, fourteen in the cHTN group, twenty-nine in the GH group and nineteen in the PEC group. Four patients in each of the cHTN and GH group, and six in the normotensive group developed peripartum superimposed PEC. These patients were therefore analyzed in the PEC group, resulting in twenty-nine normotensive controls, ten patients with cHTN, twenty-five with GH and thirty-three in the PEC group. The mean gestational age of patients was 38.6 weeks. Serum creatinine (SCr) ranged from 0.37-1.10, mean 0.63 mg/dl. The mean time from ante-partum serum blood draw to delivery was 9.28 hours (SD +/- 6.8), mean time from delivery to postpartum draw was 12.9 hours (SD +/- 6.5). A minority of patients were already receiving at least one antihypertensive prior to admission; 3/10 chronic hypertensives (30%), 1/25 GH patients (4%), 7/33 preeclamptics (21%), this latter group includes eight patients with superimposed PEC on either cHTN or GH, and six normotensives who developed PEC. Oral antihypertensive requirements (labetalol, nifedipine ER, nifedipine IR) during hospitalization included 3/10 (30%) chronic hypertensives, 4/25 (16%) in GH group and 16/33 (48.5%) of preeclamptics. 9/33 (27.3%) preeclamptics required IV antihypertensives (IV labetalol, IV hydralazine) for severe range blood pressures. Vaginal delivery was the most common delivery mode in each group except for the normotensive group in which 18/29 (62%) of patients had caesarian sections. Ten of our thirty-three preeclamptic patients (33%) exhibited severe features (Table 1)
| Normotensive | Chronic hypertension | Gestational Hypertension | Preeclampsia | Total | |
|---|---|---|---|---|---|
| C-Section | 18 | 2 | 10 | 13 | 43 |
| NSVD | 11 | 8 | 15 | 20 | 54 |
| Total | 29 | 10 | 25 | 33 | 97 |
Table 1: Mode of Delivery in each Study Group
The mean antepartum NT-proBNP level in the normotensive control group was 65.4pg/dL, 82.1pg/dL in cHTN group, 64.8pg/dL in the GH group and 133.3pg/dL in the PEC group. Although there was a trend towards higher antepartum NT-proBNP levels in patients with cHTN and PEC as compared to control or GH groups, it was not statistically significant. The mean postpartum NT-proBNP level in the control group was 209.2pg/dL, 207.7pg/dL in cHTN group, 259.5pg/dL in the GH group and 198.8pg/dL in the PEC group. We found no significant differences in antepartum (p=0.47) or postpartum (p=0.32) NT-proBNP levels between patients in the normotensive control group, cHTN group, GH group or the PEC group. (Table 2)
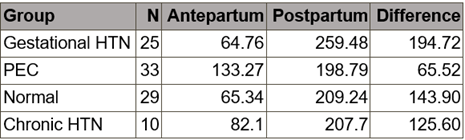
Table 2:Mean NT-ProBNP (pg/dL)
The mean antepartum NT-proBNP levels for all groups combined was 90pg/dL (5-988pg/dL). The mean postpartum NT-proBNP was significantly more elevated at 218.5pg/dl (11-1151pg/dL). The change in NT-ProBNP level from antepartum to postpartum (i.e. postpartum – antepartum level) did differ significantly across groups (p=0.01). The increase in NT-ProBNP was significantly larger in the gestational HTN group compared to the PEC group
(194.7pg/dL vs 65.5pg/dL respectively; p=0.004). A statistically significantly increase in postpartum NT-proBNP was also noted in normotensive controls compared to preeclamptics (mean rise 143.9pg/dL vs. 65.5pg/dL respectively; p=0.0081). There was not enough evidence to conclude that the increase in NT-ProBNP level differed between any other two groups. (Table 3)

*A result was considered statistically significant if p-value less than 0.05
Table 3: Differences in Mean Postpartum vs Antepartum NT-ProBNP (pg/dL)
ProBNP is secreted by cardiac myocytes then cleaved into the active form BNP and the inert N-terminal fragment NT-proBNP which is preferred for measurements as is not enzymatically degraded by neprilysin. Its action is to induce natriuresis in the setting of volume expansion and pressure overload. Serum NT-proBNP is a measurable surrogate for left ventricular cardiac strain in a variety of clinical settings, including hypertensive gestational disorders.
Several studies of NT-proBNP levels in uncomplicated pregnancy and in those with HGS have been previously published mainly in obstetric and cardiology literature. While the data is often conflicting, the consensus is that NT-proBNP levels tend to be mildly higher in pregnancy compared to non-pregnancy even in normotensive pregnant patients.15 This is attributed to increased blood volume, cardiac output and left ventricular end diastolic pressures generating subclinical cardiac strain, with clinical hemodynamic compensation and adequate pressure-natriuresis. In a study of 101 healthy pregnant women, mean NT-proBNP levels at 18-24 weeks gestation were 60pg/ml, the in-labor antepartum mean was 73.5pg/ml. The highest levels were seen within 48hrs postpartum, 157.98pg/nl, coinciding with an immediate postpartum peak in left ventricular volume.17 The trend of most prior studies is that these elevated NT-proBNP levels stay relatively stable throughout uncomplicated pregnancy up until the immediate peripartum period, where they rise maximally within 24-48hrs postpartum and up to one week postpartum.7
The literature on NT-proBNP levels as they correlate to gestational disorders of pregnancy is more variable. Our goal was to evaluate whether immediate antepartum and postpartum mean NT-proBNP differed significantly between groups of HGS based on the expected cardiac strain conferred by their particular hypertensive disorder. Based on prior studies showing maximal hemodynamic strain in pregnancy occurs in the immediate postpartum period, we measured NT-proBNP levels during labor up to 24hrs prior to delivery, and again within 24hrs of delivery. This allowed us to examine the degree of rise in NT-proBNP levels between each HGS group and controls in response to the cardiovascular demands of delivery, shedding light on potential differences in cardiovascular reserve or adaptability in these patients.
The mean postpartum NT-proBNP levels in all study groups were significantly higher than their antepartum levels. There was a 2-3 fold rise in NT-proBNP within 24hrs of delivery, consistent with literature that delivery confers a measurable degree of maternal cardiac strain even in pregnancies not complicated by hypertension.17 Interestingly, we found a statistically significant rise in peripartum NT-proBNP levels between study groups during the 24 hours pre-delivery to the 24hrs post-delivery as well. This difference was most significant in the patients with gestational hypertension and preeclampsia as compared to normal controls and chronic hypertensives. A study by Giannubilo et al in 201418 found that while NT-proBNP levels were higher in pregnant chronic hypertensives around 16 weeks gestation compared to normotensive pregnancies, their levels plateaued and remained stable throughout the rest of pregnancy. This early elevation and then plateau of NT-proBNP mirrors that seen in studies of uncomplicated pregnancies versus non-pregnancy. The steady NT-proBNP levels even towards term suggests that chronic hypertensives may have an increased ability to adapt to the increased intravascular volume later on in pregnancy without a significant increase in left ventricular end-diastolic pressure or stress, perhaps conferred by the adaptation to chronic pressure overload. It is possible that GH and PEC, both fairly acute processes compared to cHTN, result in a more rapid increase in cardiovascular strain, impairing adaptation. Similarly, Verlohhren et al25 in 2017 noted significantly elevated NT-proBNP levels at 35 weeks gestation in patients with GH and PEC as compared to normotensive pregnancy. We found no significant difference in ante or postpartum NT-proBNP levels between normotensive patients, chronic hypertensives, gestational hypertensives or preeclamptics. The PEC
group had the highest antepartum mean NT-proBNP, trending towards but not reaching statistical significance. Coupled with the fact that the PEC group had the least rise in postpartum NT-proBNP levels, one may consider the higher antepartum levels as a possible signal of impending cardiovascular decompensation in the setting of the vasoconstriction conferred by preeclampsia.
Given that our study was a small population, some of our findings, in particular the trend towards higher mean postpartum NT-proBNP levels in our PEC cohort may not have reached statistical significance due to sampling error and other confounding factors. Another important note is that 62% of our normotensive controls underwent elective cesarean sections, compared to 20% in the cHTN group, 40% in GH and 39.4% in the PEC group. We prioritized minimizing interventions in this sensitive study population and as such, we enrolled more normotensive patients with planned C-sections because per hospital protocol they already required at least one blood draw. Higher peripartum NT-BNP levels in the normotensive groups may have been related to intra-op cardiovascular stress, anesthesia, intravenous fluids and blood products.
While using NT-proBNP is a validated marker for cardiac strain, it can be affected by other factors that need to be considered, particularly in pregnancy. Obesity, infection and intrauterine growth restriction can increase NT-proBNP levels.15,17,18 Lev-Sagie et al26 reported an increase in NT-proBNP in women receiving epidural pain relief versus not. A study from 2007 by Tintonin et al27 published in AJOG found higher levels of NT-proBNP in patients with preeclampsia who were treated with antihypertensives versus not. It is unclear whether these factors cause an independent rise in NT-proBNP regardless of the patient’s hemodynamic status or whether the cardiovascular strain conferred by some of these conditions is what drives the rise in NT-proBNP. In those patients with severe PEC and kidney impairment, the reduced clearance of NT-proBNP may lead to exaggerated elevations in peripartum levels.
Gestational hypertensive disorders are increasingly prevalent in the United States due to increases in co-morbidities, maternal age and infertility interventions. Underlying conditions known to confer higher risk of hypertensive complications during pregnancy include obesity, chronic hypertension, diabetes, cardiovascular and kidney disease including proteinuria, and often these patients have several compounding risk factors. As obstetricians, nephrologists and cardiologists treating this high-risk population, we must be aware of the increasing incidence of GHD and work towards a better understanding of the underlying pathophysiology as well as predictors of GHD especially preeclampsia. This is the first study to prospectively assess the NT-proBNP levels of pregnant normotensives, chronic hypertensives, gestational hypertensives and preeclamptics pre- and post-delivery during the period of maximal pregnancy-related cardiovascular strain. Our data show all groups had higher antepartum NT-proBNP levels compared to non-pregnancy. There was a trend towards higher antepartum NT-proBNP in those with chronic hypertension which we think may be secondary to adaptations to longstanding elevated blood volume and pressure. Those with preeclampsia showed an even larger trend towards higher antepartum NT-proBNP which may be an indicator of impending preeclampsia. Mean NT-proBNP rose two-three times antepartum levels immediately postpartum in all groups, however the degree of rise was significantly larger in gestational hypertensives and normotensive controls compared to those with chronic hypertension and even more so in preeclampsia, likely due to the latter two group’s already higher antepartum levels. More research is needed to elucidate whether there is a negative predictive value NT-proBNP cut off in immediate antepartum NT-proBNP level or degree of rise in postpartum NT-proBNP that we can use to aid in the often-difficult diagnosis of exacerbation of chronic or gestational hypertension versus developing preeclampsia.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
