
Research Article | DOI: https://doi.org/10.31579/2639-4162/219
1 Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
2 MSc BSc RMN Lecturer in Mental Health Nursing with Dementia Specialty. University of Cumbria, Bowerham Road, Lancaster, LA1 3JD England.
*Corresponding Author: Jan van de Rakt, Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
Citation: Jan Van de Rakt, Steve McCarthy-Grunwald, (2024), Treatment of the severe rigidity in the morning by Parkinson, J. General Medicine and Clinical Practice, 7(16); DOI:10.31579/2639-4162/219
Copyright: © 2024, Jan van de Rakt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 August 2024 | Accepted: 05 September 2024 | Published: 13 September 2024
Keywords: rigidity; Parkinson; last phase of parkinson disease; tone treatment through push-away orthosis
Background/ Aim.
Treatment of people with Parkinson will be continued through the whole life of this person. All away until the last phase often in a Nursing home and often is he/she dependent of an wheelchair /bed. The part of the disease in the beginning is well documented and the number of treatments are enormous and of an great high degree, but this degenerative disease will change the possibilities dramatic and then is treatment an lot more difficult and thus also the results are often minimal. This phase asked for our attention, intervention and measurements to develop a treatment with an evident base.
Design.
The approach done by people with dementia that are in the Foetal attitude was the start that our attention also goes to people with Parkinson in the last phase. Because the amount of stiffness was so height that the resemblance was great with paratonia. Paratonia is an pathological neurological tone increase that can lead to an attitude that is hardly to change and people where often cognitive total absent. Elements of this “picture’ say we also by people with the last phase of Parkinson and often in morning and measurements of the tone give us the clarity that also there was an high pathological neurological tone.
Result.
The intervention though pressure on the feet by hard pillows and/or orthosis gave an reaction of “pushing away” and that is an movement. Movements does not possible when the tone was so high especially in the morning. Then this tone was around Mas-P = 4 but through this “stimulation” movements, this tone decreases almost 2 levels to Mas-P= 2. This tone decrease makes the whole morning ADL with the transfers and eating better possible and give the quality of live an positive kick.
Discussion and conclusion
The treatment possibilities for people at the end of the disease of Parkinson are limited but there are possibilities. This article about the reaction of hard pillows and/or orthosis with the investigation of the reaction though tone measurements should be an start for further good research how we can hold the quality of life as high as possible.
Parkinson ‘disease is a degenerative disease that is increasing in the world through all kinds of reason but also through pesticides [1] and that asked for ban on it, but also for a network to treat and go along with this people the whole way of this disease. In the Netherlands is the Parkinson Net start with this network that is also going international [2,3,4]. The result is that more understanding is now for this disease and that people will be see earlier and therefore will a longer and especially an higher quality of life, be possible. But still, it is a neurological disease that will go over many years but the symptoms will be bigger and that asked for treatment that has an answer for everyone to make live as well as possible.
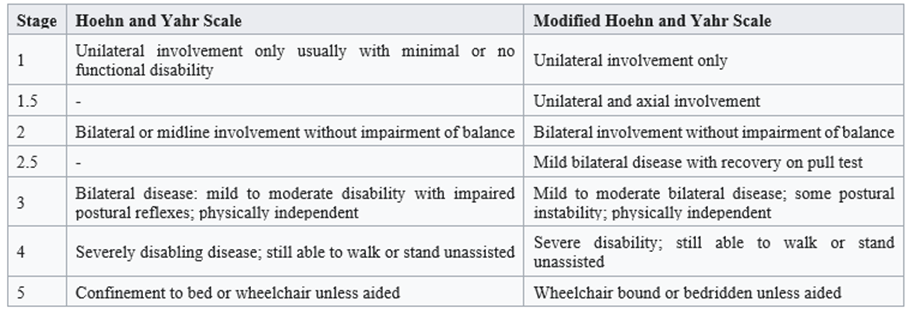
Table 1 [5]
The development of this disease is evident and it also obvious that at the end this people are dependent of assistance in all domains of movement and ADL. Further, the possibilities to speak, eat and swallowing at the end always a problem that need extra attention. Treatment with medications will help for a long period and also but regrettable lesser at the end and then is it important that the caregivers around the person has possibilities to increase the quality of live. So will the Pisa attitude have an influence on the swallowing capacity of this person and can this be decrease for moments through the day so that eating, swallowing get better. [7,8]
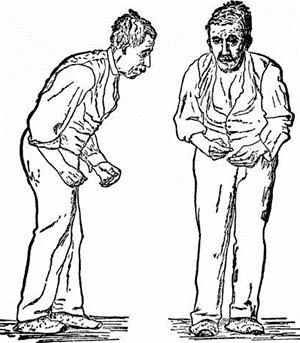
Picture 1: The picture that for long time has THE association with the Parkinson disease. This isn’t the picture that many people have, thanks to the increase of the treatment but regrettable will the attitude, the symptoms as stiffness, freezing, balance loss etc. be so clear that for all is assistance needed to get out the bed, in the clothes etc. In all books in literature this stiffness is a great problem and therefore must we search, what the cause of this stiffness is and or we can change/decrease it for moments through the day as by the Pisa syndrome.
In many literatures this stiffness is described as follow;
Stage 5 [6] “This is the most advanced and debilitating stage. Stiffness in the legs make it impossible to stand and walk. The person is bedridden or confined to a wheelchair unless aided. Around the-clock care is required for all activities.
Rigidity
This stiffness has a direct association with the tone in the muscles-pattern and with the neural possibilities that the damaged brain has.
Quote [10]; Objective rigidity' in PD correlates with velocity-dependent abnormal neuronal activity. The observations overall (i.e. the velocity-dependent feature of biomechanical and neurophysiological measures of objective rigidity) would point to a putative subcortical network responsible for 'objective rigidity' in PD, which requires further investigation.[9]
Quote [11]: People with PD exhibit higher values in terms of objective muscle stiffness than healthy controls. Rigidity depends on the angular velocity and articular amplitude of the mobilization applied. There are objective, valid, and reliable methods that can be used to quantitatively assess rigidity in people with PD. [10,11]
This higher tone and loss of selectivity, dexterity is the adaptation that the damaged brain must do, to get, with his lowering possibilities, the optimal control over “mind” and body and that will at the end give this enormous stiffness – rigidity but when we help the brain with information than is it possible, on moments through the day create less rigidity and possibility to move etc. Cools [13,14] et al. use the circles according Fowles to make clear what the alternatives are when a system in the brain lost their function. This has led to treatment with all kinds of cues [12] etc. and give us possibilities so seek for alternative route to decrease the rigidity for certain moments. This element that the treatment will never have a great affect through the whole day, has to do with the capacity of the damaged brain and his capacity to react on information and also on the level of this information -input- because not all input and certainly in stage 5 will enter the brain and has the same effect.
According to Cools et al. must this a stimulus on extero- /proprioceptive level and dynamic. This dynamic is so important because than will the extinction [15] be low but it has also an aspect that this group of people has a low cardio/pulmonal system, thus are they not capable to react long on this dynamic extero-/proprioceptive stimuli.
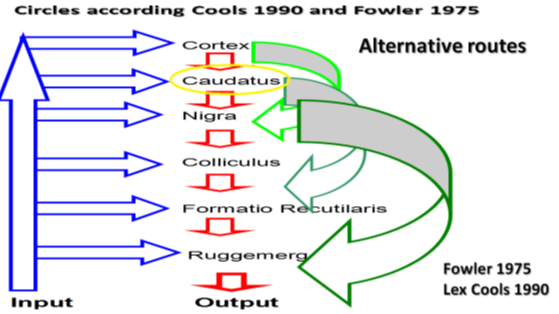
Figure 1: This figure gives a picture what the damaged brain does to decrease the effect of an bad functioning of the area around the caudates by searching for other ways. See the upper circle through the cortex, this cost more time but the control on tone, selectivity is than still possible. But when the disease progressed is this circle not possible anymore and are there only circles on a lower level possible and that has as consequences.
The consequences when the brain must use lower levels is;
Scientific evidence.
Scientific evidence is collected in the work of “The New Cognitive Neurosciences “under chief editor Cazzaniga [21c], the present of the projection in the brain and the greatness of it, determinate selectivity, dexterity, differentiation and height of tone. Damage og the somatosensory cortex forced the damaged brain to use lower situated projections, with restricted possibilities.
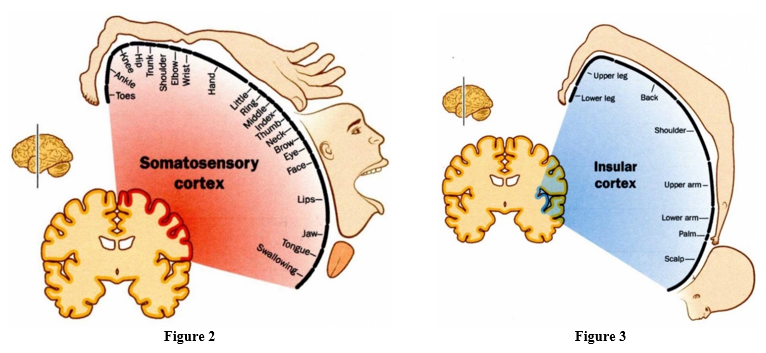
Figure 2 and 3: The projections on the somatosensory cortex figure 2 let us see much room for selectivity and thus movements variations but when we these projections see on the insular cortex than is that room almost gone and lies the focus on the base of the trunk and will the system must use, a system with limited movements possibilities. This will be achieved through the use of pathological synergies with a high tone and the highest tone will be used to create no movements at all.
This adaptation will create another way of moving and/or holding an attitude, thus must we search for another intervention.
This will give the follow picture!
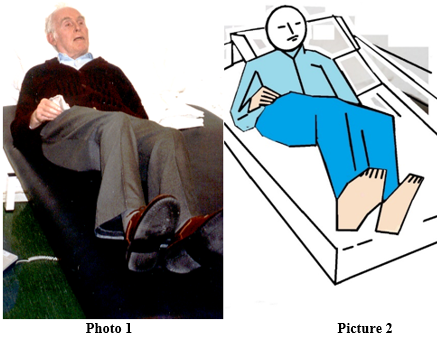
Photo 1 and Picture 2: The photo and the picture are the same person but through the picture is the attitude of the arms and legs clearer and see we the dominancy of the back diagonals and thus the dominancy of the flexion synergy (arms) and extension synergy (legs). Always lies by many people the focus on the feet and hand but by degenerative neurological disease will often early in the developmental of the disease the greatest tone increases and the necessary to use the synergy, lies in the trunk and the great joint as shoulder and hip and that because they are necessary to hold the balance etc. On the photo is the position of the elbow therefore on the bench, he is trying to move and push.
Look at his right hand, he holds handkerchief there is selectivity but, in this situation, will this handkerchief be very difficult to get to his mouth as his elbow stay on the bench. The fact that his head (extension and see the stretch tension on his throat) that this upper trunk stand in extension and lower trunk stand also in extension. Extension? we see a kyphosis but look at picture 1 this kyphosis is an eccentric extension and on photo 1 en picture 2 is the amount of concentric much higher and is his ability to move very restricted through that high tone and every attempt will this tone raise. In bed is this person in phase 4-5 thus more disable as when he stands or sit. Every attempt to move asked for an action of the front diagonals and that will be inhibit through the dominancy of the back diagonals [22]. It is important to realize that lying in a bed and move in that bed, asked for a movements strategy that is for someone with this dominancy of the back diagonal heavier than sit or stand or simple make movement in that attitude. Of course, will the transition from sit to stand be also very heavy.
Long lying in one attitude.
The difficulty of changing the lying attitude and often the long period that people are lying in the same position will change often the tone dramatically and in the morning this person has often a tone that is at his maximum [23,24,25,26]. This rigidity can be so high that no movement can occur, certainly not on his own and caregivers must try to get the arms and legs in motion and that asked often, much effort. The transfers in and out bed together with the washing and dressing make this a hell of a job for both. Though the danger of pressure scores is this person often on an bed with an anti -decubitus matrass that is capable to divide the pressure and decrease that risk. But out the research from people with paratonia through dementia [27,28] we known, that this can be an instable base that will increase the tone and create an attitude with a tone of Mas-P 4 and create an attitude known as the Foetal attitude. This tone increase will give much more pressure and an increase on pressure scores. This extreme high tone allows no movement and that same we see by people in the phase 5 often in the morning after a long period of lying. We therefore use the approach that we use for people in the Foetal attitude, by people with a high rigidity especially in the morning.
First, we make the bed stable through fill the anti-decubitus with air and create so a stable matrass, some people, in previous phase, where now better capable to start with some movements on their “own” and this movements create a tone decrease what we want to get the transfers and the ADL on a better level for both parties and decrease the decubitus (pressure score) risk. But the group in the phase 5 with the rigidity that is extreme, was this not enough. Still the base is important because the other inventions were lesser effective, without this stable base and this reaction on this stable base asked for an amount of time. The idea that:” make the matrass hard` and the movements start is wrong idea, this will often cost some time before this information enter the brain and the first reaction will occur. Thus, start with this a half hour before you start with the ADL and transfers with creating a stable and hard base because that give a reaction [29] by many people with neurological disorders. Therefore, the group in phase 5 need certainly this base and certainly for a half hour before we go to stimulated this person to push!
Push/away orthosis.
The principle is to stimulated the person to move. In this case we try to give a proprioceptive and exteroceptive stimulus that enter the brain and stimulate this person to move. That means that the stimulation must be so that it enters the brain, this damaged brain must “feel” this stimulation, only than is a reaction possible. In the Fetal attitude treatment, we could with this intervention decrease the tone about 2 levels (from Mas-P 4 “no movement at all” to Mas-P 2” movement with a clear resistance”) [25] and often the cognition improves but the restriction was always that this was only when the person lies stable and it works only for one hour, sometimes more. And this intervention has need for a preparation from minimal a half hour on a stable bed and after that, could be start with the push-away orthosis. By people with Parkinson could an orthosis be necessary but sometimes was a stable – hard- bed with some hard pillow under the feet enough to get the effect of push-away. This because (see photo 1) the legs are often still in extension and then could a padding of the area be possible but important is that there must be a tension in the situation that the “brain” must feel because than will there be a reaction.
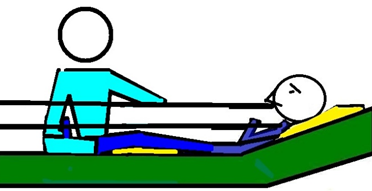
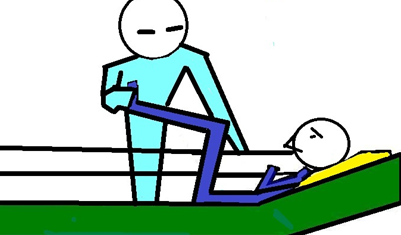
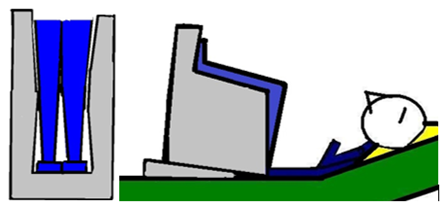
Picture 3: A situation in which the therapist test what the amount of pressure against the feet sole will give the push-away reaction. In this case no clear loss of mobility in the joint thus when the reaction is there, will this be on call with some hard pillow – picture 4

Picture 4: Now the space between the feet and the back of the bed is full with hard pillow and the dorsal flexion is maximal, this all to stimulated the brain to push away. Often people find this not fine and that means that the stimulus has enter the brain. Important detail the head rest stand up and that is important by all neurological diseases because flat lying can increase the extension tone starting in the neck and that makes a reaction more difficult (Tonic Labyrinth Reaction [17]).
Thus, a stable bed and after a reaction on it, the push-away pillows. Thus, this starts about an hour before the caregivers start with the ADL and transfers. Of course, asked every individual for an own approach and also the timing but a good multidisciplinary team will find this fast. When the mobility in the joints is restricted through so-called “contractures” [20] than is the stability much more difficult and is beside a stable bed, a head rests up also an orthosis necessary to create that stability. Thus, first increase stability and then must we determinate how we can change this orthosis in a push -away orthosis.
That means 3 elements and every time test the tone after that intervention;
Picture 5: Test to determinate in which position this person push the hand away, that stand against the foot soles.
But again, this push-away orthosis will be useful in a restricted amount of time and thus on 2 or 3 occasion through the day with an effect of an hour mostly! However, when this effect can increase through a harder matrass, head rest position and an orthosis that stabilized the legs and can give an elongation of this effect. This orthosis must give stability, that stability must enter the brain and to controlled that is only measurement of the tone the right option and not the picture that we see. Often the comment is that the person lies relaxed but when the tone was measured the opposite was true. The tone was so high that movement wasn’t possible.
There are the criteria for such an orthosis;
And always measure the tone when there is a reaction and measure also after hour. We know that measurements can increase the tone but it is so important to know what the interventions do!
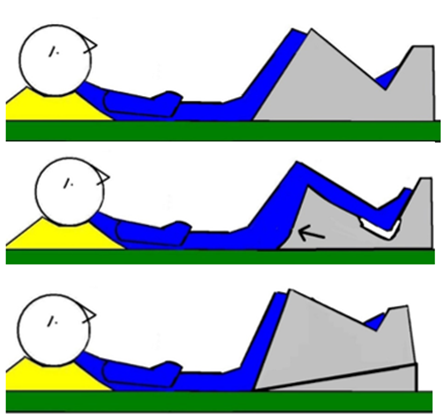
Picture 6, 7 and 8: How the orthosis is built up with a clear support area for the feet and still with a protection “gap” for the heel to prevent pressure scores (picture 7). Picture 7 let us see how an orthosis looks like when the side part is “removed”. Picture 8 give an impression when we place an extra part under the orthosis to create a push away orthosis.
Picture 9 and 10: The first picture let us see how the legs are placed in the orthosis and make clear how this gives information but also stability not only by the feet but also along the side and back of the legs. Picture 10 give an impression when the position of the legs is extreme than must the orthosis be so that placing can be easy and again with an extra piece can change in an push-away orthosis.
The last stage of the disease of Parkinson gives often a tone that is extreme and make people so stiff that movement starting is almost impossible Especially in the morning is this often a great problem for both parties. There is a solution with its restriction qua time and can help the start and other moments through the day. The morning makes transfers and ADL easier but often also the possibilities to eat/swallow and there is often also a cognitive improvement. Through wise chooses through the day can these moments give a better quality of life, but it asked for measurements of the tone and. a multidisciplinary team. This measurement of the tone is so important because than will be clear or this intervention works and when not, it should inspire us to search further. The effect of the treatment of the Pisa -syndrome [7] through higher pressure with the reaction of pushing away, has never be found as the tone measurements not be the base for this investigation and treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
