
Research Article | DOI: https://doi.org/10.31579/2694-0248/052
* Clinic for Trauma, Orthopaedics and Sports Medicine, Hospital Barmherzige Brüder, Prüfeninger Str. 86, 93049 Regensburg, Germany.
*Corresponding Author: Franz Müller, Clinic for Trauma, Orthopaedics and Sports Medicine, Hospital Barmherzige Brüder, Prüfeninger Str. 86, 93049 Regensburg, Germany.
Citation: Ramzi Yosef, Christian Wulbrand, Bernd Füchtmeier and Franz Müller, (2022). Treatment of Geriatric Subtrochanteric Femoral Fractures with Nailing. Is Operation on Duty Associated with Inferior Outcome? J Clinical Orthopaedics and Trauma Care, 4(5); DOI:10.31579/2694-0248/052
Copyright: © 2022, Franz Müller. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 December 2022 | Accepted: 06 December 2022 | Published: 20 December 2022
Keywords: subtrochanteric femoral fracture; time of operation; revision; mortality; outcome; HRQoL; ASA
Background: Subtrochanteric femoral fractures are often require open reduction and internal fixation. Data regarding the time of operation are missing; therefore, we conducted this retrospective and monocentric study.
Material and Methods: Between 2006 and 2020, a total of 115 patients with subtrochanteric fractures were enrolled. Treatment was performed with long nailing. We performed two groups: operations started within regular working hours (8:00 am – 16:00 pm; n = 41); and operations started on duty (n = 74). Based on our database, 24 variables were assessed. The primary outcomes were revision, infection, general complications, and survival. The secondary outcomes were the EuroQol five-dimension scale (EQ-5D-5L) health state, the EQ Visual Analogue Scale (EQ-VAS) and the Parker mobility score.
Results: The mean age of the patients was 81.8 years (range 65–97). With one exception (time to operation), the variables were balanced between the two groups. The revision rate was 11.3% (n = 13), with a nonsignificantly higher rate for treatment on duty (n = 11/74 vs. 2/41; p = 0.134). All infections (n = 5) occurred after treatment on duty, but this was nonsignificant. The Kaplan–Meier survival rate was also nonsignificant between the groups (log rank = 0.282), with a total one-year mortality rate of 25.2%. After a mean follow-up of 5.5 years (1.1–14.2), outcome measures were similarly reduced in the two groups.
Conclusions: Based on our study, we recommend operation within 24 hours after admission and regardless of time. Further studies with a higher number of cases are provide general recommendations.
In contrast to proximal or femoral neck fractures in geriatric patients, subtrochanteric fractures are less common. The recently published Swedish Fracture Register reported a rate of at least 22% within 10,548 consecutive hip fractures [1], and an observational study with 2,000 proximal femoral fractures assessed a prevalence rate of 7% [2]. General accepted definition of subtrochanteric fracture is a main fracture line from the distal border of the lesser trochanteric and up to 5 cm distally. However, clear definition of subtrochanteric fracture is unequally, based on different classification systems [3]. Therefore, variable rates are reported, but a number of < 10>
Nonetheless, subtrochanteric fractures should be treated with operation, and intramedullary nailing is generally used and recommended for geriatric patients [4-6]. Extramedullary fixations, e.g.; with dynamic hip screw, are more unusual based on study results comparing intra- versus extramedullary fixations [7, 8]. Operative treatment is very challenging, and open reduction with one or more cables or wires of the proximal femoral shaft is often necessary for better results [9-11].
At least, the outcome of subtrochanteric fracturesis accompanied by higher morbidity and mortality, and functional decline in comparison to pertrochanteric fractures [12]. Within one year after operation, the level of social depencey and walking ability is still decreased in comparison to the pre-injury status [13].
To reduce morbidity and mortality, national guidelines recommendoperation within 24 or 48 hours after admission [14-16], based also on register data with a very high number of cases [17-18]. Therefore, operations are often performed on duty, especially to decrease the time to operation and to reduce the selling of electively planned operations. However, to the best of our knowledge, no study has investigated the timing of operation with regard to regular workingtime (8:00 am – 16:00 pm) versus on-duty operations, and with respect to outcome. Therefore, we conducted the current study to close this gap.
This monocentric study was conducted in our academic centre as a retrospective review according to the principles of the World Medical Association Declaration of Helsinki. Data were retrieved from our electronic database, and verbal informed consent was obtained from all patients or relatives who participated in follow-up with telephone interviews.
The electronic database included proximal femoral fractures, including subtrochanteric fractures operatively treated since 2006 with baseline characteristics and peri- and postoperative variables, including complications and mortality with a minimum of one year after operation. Time to operation and time of incision were accurately assessed for all patients.
For this study, we included subtrochanteric femoral fractures with an age of ≥ 65 years, a low impact injury, and operative treatment with nailing between 2006 and 2020. A subtrochanteric fracture was defined as a proximal femoral shaft fracture with the primary fracture line within 5 cm distal of the lesser trochanter [19]. Additional fracture lines vertically into the greater trochanter were included. For classification, we used the most frequently reported system introduced by Seinsheimer in 1978 [19]. Classification was carried out by the first and senior authors, and the last author has implemented and upgraded our database for 10 years. We excluded subtrochanteric fractures with an age < 65>
Baseline characteristics included age, gender, affected side, and body mass index (BMI; kg/m2). Comorbidities were assessed according to the American Society of Anaesthesiology (ASA), and individual reported comorbidities are given in Table 1.
| Variable | Total sample size n = 115 | Working on duty n = 74 | Regular working hours n = 41 | p value |
| Age (years) | 81.8 (7.78) | 81.4 (7.74) | 82.4 (7.91) | 0.465 |
| Female sex (n) | 79 | 51 | 28 | 1.000 |
| Body mass index (kg/m2) | 27.2 (5.34) | 27.5 (5.29) | 26.7 (5.43) | 0.103 |
| Left side (n) | 63 | 39 | 24 | 0.564 |
| Seinsheimer Classification (n) |
0.559 | |||
| IIA | 3 | 0 | 3 | |
| IIB | 19 | 8 | 11 | |
| IIC | 19 | 6 | 13 | |
| IIIA | 44 | 15 | 29 | |
| IIIB | 5 | 3 | 2 | |
| IV | 18 | 8 | 10 | |
| V | 7 | 1 | 6 | |
| Treatment (n) | 0.448 | |||
| Closed | 12 | 10 | 2 | |
| Open with 1 Cerclage/wire | 25 | 17 | 8 | |
| Open with 2 Cerclage/wire | 49 | 30 | 19 | |
| Open with 3 Cerclage/wire | 29 | 17 | 12 | |
| Time to surgery (hours) | 13.6 (12.39) | 12.1 (13.39) | 16.5 (9.87) | 0.001 |
| Duration of operation (minutes) | 123.3 (39.38) | 119.8 (36.45) | 129.5 (43.98) | 0.467 |
| Intraoperative blood loss(ml) | 685,8 (458.25) | 724.1 (477.96) | 627.2 (425.93) | 0.263 |
| Perioperative transfusion/Units | 2.3 (1.89) | 2.5 (2.06) | 1.9 (1.5) | 0.272 |
| ASA Classification (n) | 0.355 | |||
| II | 28 | 17 | 11 | |
| III | 79 | 50 | 29 | |
| IV | 8 | 7 | 1 | |
| Creatinine value(mg/dl) | 1.3 (0.91) | 1.3 (1.08) | 1.1 (0.43) | 0.284 |
| C-reactive protein value (mg/l) | 14.0 (29.9) | 15.2 (32.89) | 11.9 (23.81) | 0.600 |
| Haemoglobin value (g/dl) | 12.2 (1.96) | 12.2 (2.14) | 12.2 (1.62) | 0.755 |
| Hypertension (n) | 87 | 54 | 33 | 0.497 |
| Heart failure (n) | 40 | 26 | 14 | 1.000 |
| Diabetes (n) | 33 | 21 | 12 | 1.000 |
| Atrial fibrillation (n) | 36 | 22 | 14 | 0.677 |
| Dementia (n) | 28 | 17 | 11 | 0.656 |
| Chronic obstructive lung disease (n) | 10 | 4 | 6 | 0.163 |
| Parkinson disease (n) | 4 | 3 | 1 | 1.000 |
| Marcumar or NOACs(n) | 27 | 17 | 10 | 1.000 |
| Insulin therapy (n) | 6 | 4 | 2 | 1.000 |
| Hospital stay (days) | 15.3 (6.11) | 15.4 (6.67) | 15.3 (5.02) | 0.544 |
Unless otherwise noted, values are given as the mean, with the standard deviation (± SD) in parentheses. ASA= American Society of Anaesthesiology
Table 1. Variables
Further perioperative data included time to surgery (from arrival in the emergency department to incision in minutes), exact time of incision, preoperative blood values, duration of operation in minutes, estimated intraoperative blood loss in ml, perioperative total blood transfusion per unit, and hospital stay (including the day of admission and discharge), resulting in 24 assessed variables.
For this study, we performed two groups: one group underwent operations within the regular working time (7:00 am – 16:00 pm), and the other group underwent operations on duty (16:01 pm – 6:59 am). The primary outcome was any revision, infection, and survival. Infection was defined according to the criteria of the Working Group of the Musculoskeletal Infection [20]. The secondary outcome was health-related quality of life (HRQoL), assessed by the EQ-5D-5L® (EuroQol Research Foundation 2019, 3068 AV Rotterdam, Netherlands). This instrument comprises five dimensions, which each having five options to assess severity: no problems and slight, moderate, severe, or extreme problems. The calculated index values range from 1.000 (best health) to − 0.205 (worst health status) for our country. The Visual Analogue Scale (EQ-VAS) ranges from the best (100 points) to the worst (0 points) current health state that the interviewed patient can imagine [21, 22]. Mobility was assessed with the Parker mobility score [23]. A minimum of zero points represents bedridden, and a maximum score of 9 points is given for walking ability for shopping without assistive devices.
Outcome measures were assessed by telephone after a minimum of one year after the operation. For patients with abnormal mental status (dementia), we assessed only the Parker mobility score reported by their relatives. The hypothesis was that there would be no difference in outcome between the two groups.
Operative technique
All operations were performed under general anaesthesia in the supine position on a radiolucent traction table with an X-ray converter. Preoperative single-shot antibiotics were given to every patient. All operations were performed by senior trauma surgeons (residents) or under their supervision with antegrade nailing using a cannulated proximal femoral nail. Other types of nails were not used. The lengths of the nails are between 300 and 480 mm with a diameter of 10 mm. When closed reduction failed, prior to nailing open reduction and fixation with cables or wires were performed. Reaming of the diaphysis was not used routinely. All nails were distally locked with two screws. Postoperatively, patients were mobilised with full-weight bearing as tolerated.
Kolmogorov–Smirnov tests were used to determine the distribution of the variables. The variables in this study were normally distributed except for age, BMI, and time to surgery. Mann–Whitney U tests were used to compare to independent samples, and Fisher’s exact tests were used for unadjusted comparison of proportions, whereas Pearson’s chi-squared tests were used for unadjusted comparison of ordinal variables. Data are presented as the mean values with standard deviations (SD) or as percentages (%). Kaplan–Meier survival analyses were used to determine the association between death and the time of operation (regular working hours vs. on duty). Log-rank tests were used to compare survival probabilities. All statistical tests were two-sided, and p values less than 0.05 were considered to indicate statistical significance. SPSS software for Windows. version 24.0 (SPSS, Chicago, Illinois), was used for all analyses.
From January 2006 through December 2020, a total of 3,394 patients aged ≥ 65 years underwent operation for proximal femoral fractures. Of these patients,3,273 were excluded – 1,578 femoral neck fractures, 1,687 trochanteric fractures, and 8 subtrochanteric femoral fractures not treated with nailing (4 dynamic hip screws, 4 primary hip replacements), which left 115 patients with 115 subtrochanteric femoral fractures for analysis. Therefore, the incidence of subtrochanteric fracture within the sample≥ 65 years was 3.6%.For the binary analysis, 41 patients were treated within the working hours, and 74 patients on duty. The mean age was 81.8 years (range65–97) at the time of operation, and women (n = 79) were more affected than men (n = 36). The baseline characteristics (age, sex, BMI, side, ASA, comorbidities) were well balanced between the two groups (Table1).
Time to operation was decreased when treatment was performed on duty, and this was the only one variable with significance between the groups (p = 0.001).For the total sample, 84.3% of the patients (n = 97) received treatment within 24 hours after admission. Further perioperative variables, including classification system, the use of cables/wires, duration of operation, and hospital stay were also non-significantly distributed (Table 1).
The total revision rate was 11.3% (n = 13). The reasons for revision were infection (n = 5), nonunion (n = 3), haematoma (n = 2), and screw cutout, iatrogenic peri-implant fracture, and fracture dislocation (each of them n = 1). Eleven revisions, including all five cases of infection, were associated with operations performed on duty, but this was not significant (Table 2).
| Outcome measure | Total sample size | Working on duty | Regular working hours | p value |
| Operative revision (n) | 13 | 11 | 2 | 0.134 |
| Infection (n) † | 5 | 5 | 0 | 0.159 |
| General complication (n) | 7 | 5 | 2 | 1.000 |
EQ-5D-5L* |
0.76 (0.29) |
0.73 (0.29) |
0.79 (0.29) |
0.738 |
| Visual analogue scale* | 78.4 (23.57) | 76.5 (26.88) | 81.1 (19.00) | 0.812 |
| Parker mobility score** | 5.4 (3.01) | 4.9 (3.22) | 6.23 (2.52) | 0.286 |
| Kaplan–Meier Survival (months) | 61.27 (5.57) | 65.4 (7.0) | 49.0 (6.65) | 0.282 |
Unless otherwise noted, values are given as the mean, with the standard deviation (± SD) in parentheses. ASA= American Society of Anaesthesiology
†Infection (n = 5) is a subgroup analysis of operative revision
* EQ-5D-5Land visual analogue scale assessed for 22 living patients without dementia
** Parker mobility score assessed for all 35 living patients
Table 2. Outcome measures
Additional surgical-related complications without reoperations (e.g.; broken nails; or refused operations) were not observed. General complications, including thrombosis (n = 3), pneumonia with acute renal failure (n = 2), pulmonary embolism (n =1) and postoperative delirium (n = 1), were also non-significantly distributed.
The one-year mortality rate for the sample size was 25.2% (25/115 patients), and the estimated mean Kaplan–Meier survival for the total sample size was 5.5 years (95% confidence interval (CI) 4.2–6.0 years), without differences between the groups (log-rank 0.282; Table 2; Figure 1).
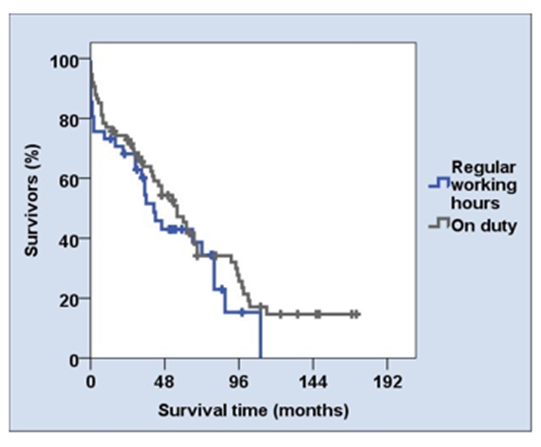
Figure 1. Kaplan–Meier survival analysis. The difference between the two groups was not significant (log rank 0.282)
Follow-up for livingpatients was assessedafter a mean follow-up of 5.5 years (1.1–14.2), and all living patients or their relatives were reached by telephone. The EQ-5D-5L and the EQ-VAS were assessed for 22 patients without dementia and for the sample with dementia (n = 35) the Parker mobility score were used. The outcome measuresshowed no significant differences between the two groups (Table 2).
The key element of our study was the use of a binary analysis to examine time of operation. For that we performed one group that underwent operations within the regular working hours and another group that underwent operations on duty. This type of analysis is considerably novel in the literature.
An epidemiological fracture register study with trochanteric and subtrochanteric fractures (n = 10,548) found no relation between the timing of operation (regular working hours: 8:00 am – 22:00 pm) and mortality, but further data, e.g., complications or HRQoL measures, are lacking [1]. Similar results were reported for hip fractures by Switzeret al., but follow-up was already completed 30 days after the operation [24]. Contrary to these two studies, Forssten et al. found that operation for hip fracture was associated with a 5% increase in the 30-day and 90-day mortality rates for patients who received arthroplasty between 17:00 pm and 8:00 am, but not for internal fixation [25]. In summary, outcome data according to geriatric subtrochanteric fractures and the timing of operation are lacking.
Additionally, the time to operation is also important. In our study with minute-based registrations, more than 80% of the patients received treatment within24 hours after admission. This is in accordance with the recommendations of national guidelines, to treat proximal femoral fractures within 24 hours after admission [14]. Therefore, both the time to operation and the timing of operation should be considered in the analysis of surgical timing.
The background for this study was, that working on duty decreases the quality of life and disturbs surgeons’ human biorhythmus [26]. Therefore, our hypothesis was that operation on duty will result in inferior outcomes compared to operation performed during regular working hours. Again, subtrochanteric femoral fractures are very demanding operations. However, and interestingly, treatment on duty did not lead to inferior outcomes in our study – although the revision rate and infection rate were higher – but nonsignificant. Therefore, further studies with a higher number of patients are recommended.
We exclusively assessed geriatric patients; therefore, our mean age was in accordance with studies using similar protocols [7, 10, 13, 27]; but older than those most reported in the past [9, 11]. It should be kept in mind, that subtrochanteric fractures occur with bimodal age distribution. First, fractures occur by high-impact injuries, e.g., motorbike accidents in young patients often associated with multiple injuries or polytrauma. Second, fractures occur particularly in geriatric women after a fall on level ground, as reported for pertrochanteric fractures or hip fractures [9]. The latter presents our sample size. From our point of view, the analysis of both young and elderly patients should take care to avoid heterogeneity and misleading results.
The incidence rate of subtrochanteric fractures in our study was approximately 3% using the Seinsheimer classification, and this rate was considerably lower than expected. A recently published multi centre study reported 909 subtrochanteric fractures within3,154 intertrochanteric fractures, which resulted in an incidence rate of about 29%, but the classification was based only on surgical codes and not on classification or radiological study review [28]. From the authors’ point of view, this record is far away from a valid number. In contrast, a further hip fracture registry obtained a rate of 12.5% among 13,939 patients with extracapsular hip fractures [12], and the clinical study of Arshad et al. [27] reported a rate of only 4.8% among 1,808 femoral neck fractures. In summary, a major difference exists for incidence rates based also on a lack of consensus in fracture classification. Loizou et al. [3] identified 15 different classification systems with 2 to 15 subgroups. Although one study reported a low degree of interobserver variation for the Seinsheimer classification [29], this is still the most frequently used classification method [3].
Within the study period, we used routine intramedullary nailing for the treatment of subtrochanteric femoral fractures. It is the recommended device for the treatment of all types of subtrochanteric femoral fractures [11, 13], based on lower complications, especially for nonunion rates previously reported in studies comparing extra and intramedullary devices [7, 8]. A recent analysis of insurance routine data related the current treatment situation reported that nailing is the most frequently used device for subtrochanteric fractures, with a rate of 89% [4]. A meta-analysis including 8 randomised and 3 cohort studies also recommended nailing as the treatment of choice based on shorter operation times, less intraoperative blood loss, lower rate of fixation failure, and better functional outcome[6]. For the latter, however, outcomes were not recorded for patients aged ≥ 60 years.
Most fractures in this study, especially types III to V according to the Seinsheimer classification, were treated using open reduction and additional application of cabels/wires for fragment reduction [6]. A retrospective study including a finite element analysis by Huang et. al. [30] showed the efficacy of nailing in combination with cable/ wires in the treatment of subtrochanteric femoral fractures: within 52 patients, only one non union and no infection were reported [30]. A previously published study also advocated open reduction and cerclage wiring for subtrochanteric fractures [10, 11], resulting in better HRQoL outcome [10].
The total revision rate in our study was approximately 11%; herein, there were five infections, resulting in an infection rate of 4.3%. Miedel et al. [31] reported the same revision rate (11%), but infections were not noted. With the endpoint one year after operation, Robinson et al. [13] assessed a fracture or implant related complication rate of 23.2%, but most of them were managed non-operatively. Moreover, rate of screw cutout was in this study considerably higher in comparison to our result (4.0%; n = 12/302 vs. 0.9%; n = 1/115). At least, deep and superficial infection rate was 13.9% [31]. In contrast to this study, we did not differentiate deep or superficial infection, and in signs of infection we performed always revision with antibiotic therapy additionally. Arshad et al. [27] reported a revision rate of 9.5% andhere in two infections within 75 subtrochanteric fractures treated with intramedullary nailing. Viberg et al. [28] reported only 6 deep infections within 601 long intramedullary nails for the treatment of subtrochanteric fractures. Again, this low number is probably not valid because it is based only on transmitted code procedures. In summary, our revison and infection rate was in line or better than reported in the past.
According to the HRQoL measures, we were able to contact all 35 living patients, including 13 patients with dementia. Therefore, we had no loss to follow-up but few patient numbers. Anyway, there is a lack of HRQoL data for patients with subtrochanteric fractures. To our best, only three studies have reported outcomes with HRQoL up to date [7, 10, 31]. In one study, the authors compared HRQoL for 90 patients treated with nailing, open reduction and cerclage (n = 30) versus nailing with closed reduction (n = 60) [10]. The reported mean EQ- D-5L was 0.78 for open treatment versus 0.66 for closed treatment12 months after operation. Interestingly, in this study with a treatment period of three years, the first author performed all open procedures using four different implant types, which may be one reason, that the mean time to operation was delayed between 4 and 5 days [10]. A multicentric study published by Eckström et al. [7] evaluated 87 elderly patients with subtrochanteric fractures and treated by nailing. The authors reported a mean preoperative EQ-5D score of 0.73, and a mean EQ-5D score of 0.52 at 24 months after the operation. Approximately the same results were reported by Miedel et al. [31] 12 months after operation using long Gamma nails. Therefore, our results are in line with or even better than the reported outcome. Visual analogue scales were not reported in these three studies [7, 10, 31].
The mean Parker mobility score in our study was 5.4 for 35 patients, including those with dementia. To our best, we found no study reporting Parker mobility scores after subtrochanteric fracture treatment.
In summary, geriatric patients sustaining subtrochanteric femoral fracture showed reduced HRQoL outcomes not only in the short term [12, 7, 31], but also in the mid- to-long term, as we assessed.
We reported a one-year mortality rate of 25.2%. The rate is considerably lower than that reported by Viberg et al. [28]. In this multicentric cohort with similar descriptive data, including patients≥ 65 years, the one-year mortality rate was 32%. On the other hand, our rate is in line with the studies published by Robinson et al. [13], Arshad et al. [27] or Eckström et al. [7]. Müller-Mai et al. [4] reported a rate of 26% at one year after the operation. In contrast, and despite similar baseline characteristics, Codesido et al. [10] reported a one-year mortality rate of only10%. Explanations might be that many patients (20%) were lost to follow-up, and patients with dementia were excluded. The key message is that the one-year mortality rate in geriatric patients with subtrochanteric femoral fractures is similar to that reported for geriatric hip fractures or trochanteric fractures [12].
This study presents geriatric patients, including patients with dementiatreated for subtrochanteric femoral fracture with a long intramedullary nail. Therefore, our sample represents the clinical setting. To our best, and apart from register data or multicentric studies, we reported a very high number of geriatric patients. Furthermore, this study was the first to compare outcome measures of these often difficult-to-treat fractures within working hours versus on duty. Finally, a strength of our study is the high completeness (no loss of follow-up for living patients) and data quality with outcome measures for all living patients in the mid- to long term.
This study has limitations. First, it is a comparative retrospective study without a case–control group, resulting in a lower level of evidence without generalized results. Second, the number of patients treated on duty was much lower than that in the regular working hours group. Third, the prevalence of adverse events, e.g., infection, was low, resultingin a lack of statistical power. Fourth, despite long-term follow-up, some patients were assessed with short-term follow-up, and further complications are possible in the future. Fifth, the results cannot be generalized to other devices because we always used the same cannulated long nail device. Without a doubt, a short nail would also be appropriate for Seinsheimer type II A-C fractures. Sixth, the number of used cables/wires are based on fracture types, the degree of dislocation, and the surgeon’s personal experiences. Therefore, a bias cannot be excluded. The results of the HRQoL reflect the morbidity and fragility of the geriatric patients rather than the outcome of subtrochanteric femoral fractures. HRQoL data were available for a all living patients, but the number was low based on the high mortality rate. Further, pre-injury HRQoL were not recorded in the database. Finally, follow-up was performed with telephone calls rather than by recentradiological or clinical evaluations.
The outcome of subtrochanteric femoral fractures in geriatric patients and treated by nailing on duty was non-inferior compared to treatment on regular working hours. However, the rate of adverse events was higher but non-significantly. Therefore, we recommend operation within 24 hours after admission and regardless of timing. Further studies with a higher number of cases are necessary to provide general recommendations.
Ethical Approval
Approval was obtained by the Ethics Committee.
Consent to Participate
All patients or their next relatives gave constent to participate in this study.
Consent to Publish
Not applicable
Funding
The research did not receive any specific grant from funding agencies in the public, commercial or non-profit sectors.
Competing interests
The authors declare that they have no conflict of interest.
Availability of data and material
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
