
Research Article | DOI: https://doi.org/10.31579/2692-9759/136
Universidad Autónoma de la Ciudad de México
*Corresponding Author: Cruz García-Lirios, Universidad Autónoma de la Ciudad de México.
Citation: Quiroz-Campas CY, Javier C. Guillén, Hernández-Gracia TJ, Arturo S. Sánchez, Francisco E. Morales, (2024), Treatment adherence of Covid-19 in students from central Mexico: Contrast of a structural equation model, Cardiology Research and Reports, 6(4); DOI:10.31579/2692-9759/136
Copyright: © 2024, Cruz García-Lirios. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 July 2024 | Accepted: 08 July 2024 | Published: 16 July 2024
Keywords: covid-9; respiratory diseases; self-care; treatment adherence
Treatment adherence is a central axis in the health agenda. In the framework of the SARS CoV-2 pandemic, it is necessary to predict this phenomenon. The objective of the present work was to contrast a model of structural equations. A confirmatory, psychometric and cross-sectional work was carried out with a selection of 100 students, considering their participation in the social service and professional practices in public hospitals in central Mexico. A factorial structure was found that explained 62% of the total variance, suggesting the contrast of the model in other scenarios.
Until March 2021 100 million have been infected and three million have died worldwide from the SARS CoV-2 pandemic and Covid-19 disease so far (WHO, 2021). In Mexico, even when under-records are recognized by the health authority, 170.000 people have died (PAHO, 2021).
The vaccination policy followed the United Nations Covaxx mechanism (SSA, 2021). It is a multilateral agreement where governments contribute a fund that is distributed according to criteria established by the World Health Organization. It involves the purchase of drugs to immunize 10% to 50% of the population, following a logic of availability, production and equitable distribution among the 34 signatory countries. In addition, Mexico has negotiated directly with multinationals and governments of Russia and China for the management of vaccines. 75 million were purchased from the Oxford company, 20 million from Covaxx, 15 million from Pfizer and 30 million from Cansino, although it has made agreements with others based on compliance with the agreement, availability and supply of the vaccines. The Ministry of Health has established medical personnel as a priority for immunization until February 2021, followed by the elderly sector until April, people between 50 and 59 years old until May, 40 to 49 years old until June and the rest until March 2022.
However, information that discredits the government has propagated the association between vaccines and deaths without documenting studies, reducing the data to a coincidence and without considering the risks of exposure to immunization with comorbidities (Garcia et al., 2020: p. 51). Therefore, the empirical test of a model that allows studying the effect of unscientific information on treatment adherence decisions is essential to observe institutional health responses.
Psychological studies of adherence to treatment show that beliefs and attitudes toward self-care are determinants of adherence to treatment. In the case of respiratory diseases, this process is tempered by the perception of risk that the present study was proposed to elucidate.
Attitudinal health studies have shown that these are one-dimensional that allude to favorable or unfavorable evaluations of objects (Javiedes, 2004). This dimension explains the reasons that lead people to accept or reject attitudinal objects (Laca, 2005). In this sense, in the case of respiratory diseases, attitudinal studies suggest that epidemics are evaluated as unfavorable by the groups to which patients in intensive care belong (Montmollin, 1984).
However, other studies indicate that evaluations may be favorable when it comes to illnesses that do not warrant a long stay. People tend to evaluate positively those cyclical diseases that activate disease prevention and treatment mechanisms (Pallí & Martínez, 2004). Said favorable evaluation of acute diseases is part of a positive self-concept in which health care is a factor that increases the positive image of oneself (Peiró, Morales & Fernández, 2004).
Positive or negative evaluations of illness can be complemented by decisions about self-care, family, partner, and other groups. Intentions are another attitudinal dimension that has not been explored, described, or even explained. The state of knowledge indicates that there are two theories in charge of intentions.
The Theory of Reasoned Action (Ajzen & Fishbein, 1974) and later, the Theory of Planned Behavior (Ajzen, 1991); both refer to intentions as intermediate factors between beliefs and behaviors (Ajzen, 2001). These are future, feasible and measurable decisions that convey the effects of past beliefs on future behaviors (Ajzen, 2002). Even the theory postulates specific intentions as the main determinant of delimited behaviors. These are decisions focused on expectations of costs and benefits that activate actions limited to minimizing costs and maximizing benefits.
Experimental studies (control and manipulation of variables) have shown that the uncertainty of the risks favors the search for low costs and high benefits, compared to the certainty of risks that favors the search for low costs and high benefits. That is, when diseases are uncertain, people risk obtaining costly solutions.
Quasi-experimental studies (control of variables) have only shown that risk expectations are triggers of beliefs and intentions around a disease. In this sense, the present study explains the attitudes towards uncertain respiratory diseases in relation to groups in which individuals are immersed.
The study's contribution to the state of the art lies in the contrast of a model that studies the determinants of adherence to treatment. Consequently, the modeling and contrasting of the relationship between the variables integrates the findings of other investigations. Therefore, the aim of the research is to show the prevalence of psychosocial determinants of public health focused on respiratory illnesses in four main lines of knowledge concerning regulation, policies, advocacy and research.
Are there significant differences between the dimensions of adherence to treatment reviewed in the literature as effects of non-scientific information with respect to the contrast of the model proposed in the present work?
The premise that guides the present work indicates that adherence to treatment had been considered as part of a structure of social, work and family support in rehabilitation, but it was not considered as an effect of the non-scientific information disseminated in the media and electronic networks such as Facebook, Youtube, Twtter and WhatsApp (Nouira, 2021: p. 220). In this sense, the diversification of factors that make up the adhesion process implies the convergence of media spheres with personal, family, work and institutional spheres (Dwajani et al., 2018: p. 69). In this way, the adherence structure will include dimensions related to each area, as well as allusion to their hybrid combinations such as vaccines, their percentage of effectiveness and attribution to the government that people associate with the quality of immunization (Batool et al., 2020: p. 1917).
Design
Given that the pandemic led to a strategy of confinement and prolonged social distancing, a cross-sectional design was chosen. In addition, a psychometric study was carried out in order to establish the cognitive and behavioral variables associated with the rejection or acceptance of immunization.
Sample
A non-probabilistic selection was made of 100 students (56% women and 44% men, M = 21.2 SD = 1.23 of age and M = 9,872.12 USD SD = 234.35 USD monthly income) from a public university. The selection criterion was to belong to the system of practices and social service in organizations and institutions with and without profit aims of the municipality of Chimalhuacán, State of Mexico.
Instrument
The Scale of Adherence to the Treatment of Chronic Degenerative Diseases was used, which includes 40 assertions (items) around norms ("The treatment of Covid-19 is effective in traditional people"), values ("A person who follows the recommendations of Covid-9 experts"), beliefs ("Covid-19 affects morbid people"), perceptions ("The Sputnik V vaccine has more risks than benefits"), knowledge ("Covid-19 affects decisions"), skills ("Covid-19 can be controlled with a balanced diet"), attitudes ("Sputnik V vaccine affects older adults"), decisions ("I will get vaccinated against Covid-19"), intentions ("I would choose the Sputnik V vaccine to prevent Covid-19") and behaviors ("I got vaccinated against Covid-19").
Procedure
Opinion mining was carried out, using the Delphi method, as well as the symptom technique for the analysis of evaluations by expert judges. In three rounds the content of the items was evaluated; a) phase of review of the instrument and qualification of the reagents, b) phase of comparison of the qualifications of experts and c) phase of reconsideration or reaffirmation of the qualification.
The participants were interviewed and surveyed in the university facilities. The access to the respondents was made from the database of the degree in medicine, considering the system of professional practices and social service of the university and the collaborating institutions. They were informed that the results of the investigation would neither positively nor negatively affect their school situation. They were asked to answer the questions and statements honestly. They were invited to consult the results in the final report of the research group. The data were processed in the Statistical Package for Social Sciences (SPSS) and the Structural Moment Analysis Software (AMOS) in versions 10 and 6.0.
The instrument was validated with 100 students from the same institution. After establishing the internal consistency that reached a value higher than the essential minimum (alpha of .805) and the ten factors, its factorial structure was confirmed with 100 practitioners and professional servants.
Analysis
The parameters of kurtosis, Cronbach's alpha, KMO coefficients, Bartlett's test, factorial weights, Pearson correlations, “phi” covariances, “beta” and “range” weights, as well as adjustment indices and, residuals were used in order to contrast the model of specified relationships with the observed data.
The kurtosis value close to the unit was assumed as evidence of the normal distribution of the responses of respondents with respect to the statements that measure the study variables in an instrument with response options and interval measurement levels.
KMO coefficients are greater than 0.600 and the Bartlett test with a significance level less than 0.050 were assumed as evidence of product-moment correlations that facilitated the exploratory factor analysis of principal axes with pro max rotation. Subsequently, factorial weights greater than 0.300 were considered as evidence of the maximization of variance in terms of the factors derived from the exploratory analysis. Percentages of explained variance greater than 0.20 were assumed as evidence of acceptance of the null hypothesis.
Cronbach's alpha value greater than 0.60 was assumed to be enough to demonstrate the internal consistency of the indicators with respect to the general scale and the subscales. The product-moment correlation higher than 0.90 was considered as evidence of collinearity and multicollinearity, which means that the items are similar in terms of their contents.
Pearson's r values close to unity and zero were discarded from subsequent analyzes as they signify collinear or spurious relationships. On the other hand, those values higher than 0.30 and lower than 0.90 were assumed as evidence of dependency relationships.
The "phi" values between 0.30 and 0.90 were identified as evidence of dependency relationships in the case of categorical variables or in combination with continuous variables.
The “beta” values between exogenous and endogenous variables between 0.30 and 0.90 were assumed as evidence of dependency relationships. Similarly, “gamma” values between endogenous variables close to zero or to unity were discarded from subsequent analyzes.
The Goodness of Fit Index (GFI for its acronym in English) close to unity was assumed as evidence of fit and acceptance of the null hypothesis. On the contrary, values lower than 0.975 were considered as evidence of rejection of the null hypothesis and acceptance of the alternative hypothesis.
Values close to zero were assumed as evidence of fit between the specified relationships and the data obtained, therefore, the null hypothesis of fit between both models was accepted. In contrast, values greater than 0.007 were considered as evidence of rejection of the null hypothesis.
The values that indicate the reliability and validity of the instrument that measures treatment adherence reached values higher than the essential minimums of .60 and .300 respectively. Table 1 shows the reliability and validity values essential for the analysis of the consistency of the instrument and its measurement from the convergence of responses to the items. The results indicate that the instrument is consistent in its measurement of the dimensions established in the state of the art, as well as consistent in recording responses to items. That is, the reliability and validity values suggest that the instrument meets the requirements prior to more detailed and specific analyzes such as sphericity and suitability of the subscales to the study sample.
| R | M | SD | A | F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 |
| r1 | 4,1 | 1,9 | ,71 | ,32 | |||||||||
| r2 | 4,3 | 1,3 | ,78 | ,38 | |||||||||
| r3 | 4,1 | 1,8 | ,70 | ,51 | |||||||||
| r4 | 4,0 | 1,1 | ,73 | ,67 | |||||||||
| r5 | 4,8 | 1,9 | ,71 | ,52 | |||||||||
| r6 | 4,3 | 1,6 | ,72 | ,42 | |||||||||
| r7 | 4,6 | 1,0 | ,78 | ,49 | |||||||||
| r8 | 4,8 | 1,3 | ,74 | ,39 | |||||||||
| r9 | 4,0 | 1,4 | ,70 | ,60 | |||||||||
| r10 | 4,5 | 1,6 | ,77 | ,61 | |||||||||
| r11 | 4,4 | 1,5 | ,79 | ,62 | |||||||||
| r12 | 4,3 | 1,8 | ,75 | ,67 | |||||||||
| r13 | 4,2 | 1,9 | ,73 | ,52 | |||||||||
| r14 | 4,1 | 1,0 | ,75 | ,59 | |||||||||
| r15 | 4,4 | 1,1 | ,79 | ,53 | |||||||||
| r16 | 4,6 | 1,2 | ,73 | ,58 | |||||||||
| r17 | 4,3 | 1,4 | ,75 | ,49 | |||||||||
| r18 | 4,2 | 1,3 | ,72 | ,48 | |||||||||
| r19 | 4,1 | 1,2 | ,71 | ,57 | |||||||||
| r20 | 4,0 | 1,1 | ,70 | ,59 | |||||||||
| r21 | 4,2 | 1,0 | ,73 | ,40 | |||||||||
| r22 | 4,7 | 1,4 | ,77 | ,42 | |||||||||
| r23 | 4,9 | 1,8 | ,76 | ,38 | |||||||||
| r24 | 4,0 | 1,3 | ,74 | ,56 | |||||||||
| r25 | 4,1 | 1,2 | ,73 | ,64 | |||||||||
| r26 | 4,2 | 1,4 | ,78 | ,67 | |||||||||
| r27 | 4,3 | 1,7 | ,79 | ,68 | |||||||||
| r28 | 4,7 | 1,8 | ,77 | ,57 | |||||||||
| r29 | 4,8 | 1,3 | ,74 | ,57 | |||||||||
| r30 | 4,3 | 1,2 | ,75 | ,45 | |||||||||
| r31 | 4,2 | 1,6 | ,73 | ,63 | |||||||||
| r32 | 4,1 | 1,9 | ,75 | ,50 | |||||||||
| r33 | 4,3 | 1,0 | ,74 | ,64 | |||||||||
| r34 | 4,9 | 1,2 | ,73 | ,32 | |||||||||
| r35 | 4,7 | 1,3 | ,72 | ,61 | |||||||||
| r36 | 4,3 | 1,5 | ,75 | ,46 | |||||||||
| r37 | 4,6 | 1,7 | ,71 | ,57 | |||||||||
| r38 | 4,0 | 1,8 | ,72 | ,58 | |||||||||
| r39 | 4,7 | 1,9 | ,73 | ,46 | |||||||||
| r40 | 4,9 | 1,0 | ,70 | ,62 |
Table 1: Description of the instrument that measures treatment adherence
Source: Elaborated with data study; R = Reactive, M = Mean, SD = Standard Deviation, A = Alpha excluded value item. Adequation and Sphericity ⌠X2 = 435.12 (245 gl) p = 0.000; KMO = 0.567⌡Method: principal axes, Rotation: Promax. F1 = Norms (16% total variance explained and alpha = 0.724), F2 = Values (13% total variance explained and alpha = 0.789), F3 = Beliefs (10% total variance explained and alpha = 0.761), F4 = Perceptions (7% total variance explained and alpha = 0.829), F5 = Knowledge (5% total variance explained and alpha = 0.895), F6 = Skills (4% total variance explained and alpha = 0.886), F7 = Attitudes (3% total variance explained and alpha = 0.856), F8 = Decisions (2% total variance explained and alpha = 0.719), F9 = Intentions (1% total variance explained and alpha 0.725) F10 = Behaviors (1% total variance explained and alpha 0.826).
The ten factors explained 62% of the variance of the structure. Ten factors prevail in adherence to treatment. That is, the orthogonality of the structure suggests that it is a multiple and diverse phenomenon, not subject to a universal protocol.
Once the validity structure was established, the relationship structure was estimated considering the correlations between the factors, as well as the
covariances to observe the incidence of other factors not included in the model (Table 2). That is, the correlation and covariance values suggest that nine variables are determinants of adherence to treatment behavior. This is so because, the process of adherence to immunization through vaccines involves at least ten variables in decision making, acceptance and application of the vaccine. It is a relationship of trust between the rulers and the ruled that results in co-management.
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | |
| F1 | 1,0 | 1,8 | ,54 | ,52 | ,67 | ,69 | ,69 | ,56 | ,59 | ,46 | ,56 | |||||||||
| F2 | ,34* | 1,0 | 1,9 | ,34 | ,54 | ,57 | ,57 | ,64 | ,67 | ,30 | ,45 | |||||||||
| F3 | ,48* | ,35* | 1,0 | 1,7 | ,41 | ,47 | ,55 | ,47 | ,68 | ,51 | ,63 | |||||||||
| F4 | ,39* | ,47** | ,56* | 1,0 | 1,6 | ,37 | ,41 | ,36 | ,57 | ,58 | ,54 | |||||||||
| F5 | ,30** | ,39* | ,54* | ,30* | 1,0 | 1,8 | ,36 | ,45 | ,59 | ,63 | ,68 | |||||||||
| F6 | ,46* | ,35* | ,46** | ,38* | ,42* | 1,0 | 1,6 | ,51 | ,46 | ,47 | ,63 | |||||||||
| F7 | ,53* | ,42*** | ,36* | ,43* | ,46* | ,53* | 1,0 | 1,9 | ,53 | ,58 | ,59 | |||||||||
| F8 | ,48*** | ,41* | ,45* | ,36* | ,49** | ,45** | ,38* | 1,0 | 1,7 | ,62 | ,45 | |||||||||
| F9 | ,54* | ,45* | ,58* | ,54** | ,59* | ,58* | ,36** | ,54* | 1,0 | 1,6 | ,41 | |||||||||
| F10 | ,49* | ,38* | ,49* | ,68* | ,37** | ,47* | ,34* | ,46* | ,38* | 1,0 | 1,9 |
Table 2: Correlations and covariations between factors
Source: Elaborated with data study; F1 = Norms, F2 = Values, F3 = Beliefs, F4 = Perceptions, F5 = Knowledge, F6 = Skills, F7 = Attitudes, F8 = Decisions, F9 = Intentions, F10 = Behaviors; * pless than ,01; ** p less than ,001; *** p less than ,0001
The structure of relationships shows the emergence of a common factor that the literature identifies as treatment adherence to explain the deliberate, planned and systematic process of social and family support that sustains the decision to carry out medical recommendations. In order to establish the axes, trajectories and relationships between the variables, we proceeded to estimate the effects of the deliberate process on the decision and the action
to carry out adherence to treatment in a structural equation model (Figure 1). In other words, the structure of relationships between factors and indicators suggests that adherence to treatment is a complex phenomenon of trust between authorities and respondents. It is an immunization process that prioritizes the vaccination of students considering them strategic to mitigate the pandemic. In this administrative and institutional sequence, adherence to treatment is essential to reverse the information that vaccines are not safe.
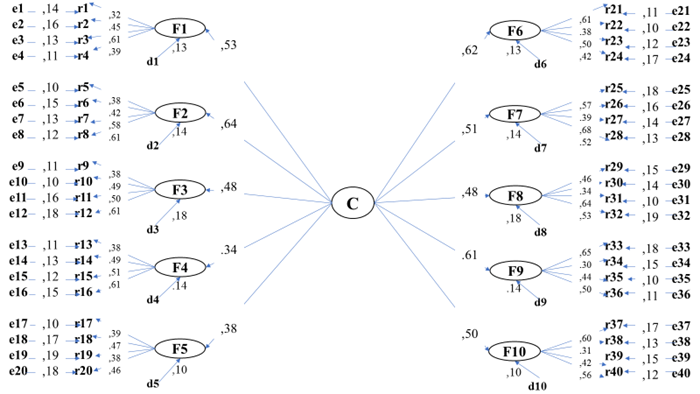
Figure 1: Structural equation modelling
Source: Elaborated with data study; C = Construct of adhesion treatment, F1 = Norms, F2 = Values, F3 = Beliefs, F4 = Perceptions, F5 = Knowledge, F6 = Skills, F7 = Attitudes, F8 = Decisions, F9 = Intentions, F10 = Behaviors, R = Indicator, d = Disturbance measurement factor, e = Error measurement indicator
The adjustment and residual parameters [χ 2 = 16.35 (17gl) p = 0.000; GFI = 0.925; CFI = 0.975; NFI = 0.975; RMSEA = 0.003; RMR = 0.002; R 2 = 0.576] suggest the non-rejection of the null hypothesis relative to the significant differences between the structure of adherence to treatment reported in the literature with respect to the structural equation model established in this work. The adjustment of the theoretical structure with respect to the proposed model suggests that the respondents are in a public health sector organized to reduce the effects of the information that refers to the inefficiency of the vaccines.
The structure of treatment adherence reported in the literature shows the importance of quality of life, socio-economic variables and reactions to medical treatment as determinants, but in the present study, it was shown that these variables are mediators of social and group norms regarding whether or not to adhere to the treatment.
Garcia et al., (2020) suggest that treatment adherence is reduced by agents external to social and family support that configure adherence to barriers. In the present work, a deliberate, planned and systematic sequence of variables related to social and family support has been established that, when interacting with cognitive variables, suppose a stable structure oftreatment adherence.
Vargas et al., (2020) found that age and adverse reactions to treatment reduce adherence and increase adherence to barriers. In the present study, a structure of 10 factors was found around which treatment adherence is reflected by a sequence that goes from norms to behavior. That is, treatment adherence involves a series of principles that guide behavior, mediated by social, family, and cognitive factors.
Casaño et al. (2020) demonstrated that treatment adherence is related to the quality of life. In the present work, it was found that adherence to treatment is reflected by a structure of social, family and cognitive resources without which the sequence of adherence to treatment would be impossible.
Research lines concerning treatment adherence as a result of the mediation of cognitive factors from social and socioeconomic dimensions will allow anticipating the barriers that inhibit it. Regarding the logical sequence of
deliberation, planning and systematization, it is necessary to point out the sociodemographic variables that accentuate the barriers or adherence to treatment.
It is suggested to carry out opinion mining, the Delphi method and the symptoms technique that allowed the construction of the instrument, as well as the content validity. If internal consistency refers to the degree of understanding of the content of each item, the three information processing phases are recommended.
Therefore, the empirical test of the model in other scenarios and samples will allow a diagnosis of the trust of users of the health service towards their health and political authorities regarding the management of the pandemic, as well as the immunization of the population, mainly the application of vaccines in order to be able to counteract the unscientific information that is disseminated in the media and electronic networks.
The contribution of this work to the state of the question lies in the contrast of a model that explained the psychological structure of adherence to treatment in a sample of practitioners and social servants from central Mexico. 62% of the total variance was explained from ten factors, with the values reflecting the sociocognitive structure analyzed.
In relation to the theoretical, conceptual and empirical frameworks related to adherence to treatment, the contribution of this study lies in the reliability and validity of an instrument that measures the evaluative, normative, perceptual, attitudinal and intentional determinants of treatment adherence.
However, the type of study and the type of sample selection limit the results to respondents and cannot be generalized to a population. A confirmatory study with a probabilistic selection is recommended to strengthen the findings of the present work.
However, the results contribute to psychological models of public health in general and studies of adherence to treatment since, unlike the model of reasoned action and the model of planned behavior, norms are determinants of beliefs and attitudes. In other words, the study sample showed cultural power in their disease-preventive lifestyles. Therefore, a study about individualism and collectivism will clarify ethnic and cultural differences.
In this sense, some studies related to multiculturalism and interculturalism show that, in migrant communities, adherence to treatment depends on learning the language and reading- writing skills more than values and norms.
Even when migrant communities manage to be represented by leaders who are in health centers, their quality of life improves through awareness of self-care and adherence to treatment.
Other studies have shown that adherence to treatment depends on parenting styles, being the most influential assertive style when establishing a rehabilitation program.
However, norms and values seem to have a greater impact on those individuals who are not heads of family and rather adjust to the customs and traditions of their community of origin. In this sense, family socialization is overcome by the sense of belonging to a community and attachment to a place of origin, including its rituals for treating illnesses that are not unrelated to mysticism protocols.
Therefore, it is necessary to deepen the incidence of self - care and public health programs in order to anticipate scenarios such as epidemics or pandemics that can further inhibit adherence to treatment and the quality of life of peri-urban communities.
The present work has demonstrated the incidence of group norms, family, friends and coworkers, on adherence to the treatment of respiratory diseases. In relation to the study by Carreón (2011) in which the norms of the labor context affected self-care and the prevention of accidents at work, mediated by the perception of risks and internal security policies, the present investigation warns that the explanatory power of group norms is significant when there is an identity related to the uses and customs of the group.
In this way, it is necessary to carry out studies that include the variable of sense of belonging and roots in a context, place or environment that allows explaining the relationship between choice and belonging of a group with respect to treatment adherence for respiratory diseases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
