
Research Article | DOI: https://doi.org/10.31579/2690-1897/125
1 Department of General Surgery, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
2 Head of Trauma Unit Charlotte Maxeke Johannesburg Academic Hospital, University of Witwatersrand, South Africa, Milpark Hospital, South Africa.
*Corresponding Author: R Pswarayi, Department of General Surgery, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Citation: R Pswarayi, MS Moeng. (2022). Trauma Patients at Risk of In-Hospital Mortality. J. Surgical Case Reports and Images 5(5); DOI: 10.31579/2690-1897/125
Copyright: © 2022, R Pswarayi, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 September 2022 | Accepted: 29 September 2022 | Published: 09 November 2022
Keywords: trauma; mortality; accidents; morbidity; resuscitation
The trauma incidence in South Africa is significantly high and forms one of the top-five causes of unnatural death. Thus, one of the higher incidences of trauma across the world. Subsequently the in-hospital mortality forms a high burden of disease on the health systems in South African health care facilities. Therefore, analysing the incidence of trauma and the various mechanisms of trauma allows for in-hospital trauma mortalities to assessed. The aim of this study was to analyse the in-hospital mortality distribution factors at a Johannesburg Trauma unit over an eight-year retrospective review from 01 January 2005 –31 December 2012 and Analysis of Trauma Bank data forms at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH). Looking at demographics, physiological parameters, mechanism of Injury, Injury Severity Score (ISS) and New Injury Severity Score (NISS). Ethics through the Wits Ethics Committee was obtained. The Statistica V8 application was used to analyse the data that was collected and a P value of <0.05 was reported as significant. A total of 18, 087 Priority 1 patients were reviewed in this study. This sample demonstrated the 21-45 years of age group was the most affected trauma group (87.3%). Penetrating injuries (Stab and gunshot wounds) had the highest incidence yet lower mortalities. However, blunt injuries (ranging from Pedestrian- and Motor- vehicle crashes, blunt assaults, falls and burns) had lower incidences and higher mortalities. The highest in-hospital mortality was due to burns patients (22.56%) followed by pedestrian vehicle crashes patients affecting the predominantly young male population. Poor probability of survival was demonstrated amongst Motor Vehicle Crashes (Ps 44%) and Motorbike Crashes (34%), and PVCs.
worldwide and over five million deaths per year [1]. This invariably may affect temporary or permanent morbidity and disability with a negative impact on the economy leading to a high burden on health care systems. In the advent of such high trauma incidence, reducing medical errors and minimizing complications is of utmost importance. This indicates the need at an institutional level that hospitals require a system where complications may be detected and surgical safety and quality can be evaluated [1]. As described by Abe T et al, Failure To Rescue (FTR) is defined as death after a surgical complication and this has a correlation with mortality [2]. FTR reflects an institution’s aptitude to rescue patients that have developed complication [2].
Despite considerably improved road safety and occupational safety strategies along with appreciable development in pre-hospital and in-hospital management of trauma patients, trauma continues to be the most common cause of death and disability worldwide, particularly in people under the age of 40 [1]. An assortment of variables affect mortality after trauma, including: age, severity of injury, site of injury, haemodynamic instability, time to definitive care, quality of care, and coagulopathy [3]. A study demonstrated that the primary causes of death in patients that arrive to a hospital are severe head injury, hypovolaemic shock, sepsis, and multi-organ-failure [3].
In the United States of America, violence kills more than 1.6 million people alone [4] and the direct and indirect costs of violence are astounding and impact national and local economies by stunting growth, increasing socio-economic inequalities, and increasing the expenditure of the health and law-enforcement departments, to name a few. This may negatively impact the health system in numerous ways – incidence, mortality, and Disability-Adjusted-Life-Years (DALYs), including disability and premature mortality [5]. The various societal/community impacts of trauma include disintegration of support networks, interruption in the provision of social services, reduced access to health and mental health treatments, decreased social capital, loss of productivity, and high societal costs [6]. According to Matzopoulos, R. et al., injury-related mortality accounted for 12% of deaths and 16% of years of life lost, mainly because of road traffic accidents and homicides [7].
The trauma incidence in South Africa is significantly high and forms one of the top-five causes of unnatural death, thus, one of the higher incidences of trauma across the world [8]. It is the leading cause of unnatural death and disability in South Africa, and accounts for approximately 50% of injury-related mortality in persons 15-44years of age [9]. Subsequently the in-hospital mortality forms a high burden of disease on the health systems in South African health care facilities [9].
Therefore, analysing the incidence of trauma and the various mechanisms of trauma with their resultant injuries, allows for in-hospital trauma mortalities to assessed. Consequently, this may permit evaluation at institutional levels and even municipal levels to reassess the quality of pre-hospital and in-hospital management, re-evaluation of surgical safety and quality, and initiation of directive preventative strategies. The main aim of this study is to classify the mechanism of injury and the in-hospital mortality rates according to the mechanism of injury.
Study Design and Methods
An eight-year retrospective review from 01 January 2005 – 31 December 2012 analysing the in-hospital mortality distribution factors at a Johannesburg Trauma unit by assessing the demographics, mechanism of injury, Injury Severity Score (ISS) and New Injury Severity Score (NISS) of patients presenting to this trauma unit thereby focusing on the variables influencing such mortalities.
Definition of terms
Analysis of Trauma Bank data forms at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) of all patients presenting to the level one trauma unit. This hospital is based in Johannesburg, South Africa. This state/government facility serves a large population of mainly low-to-middle income persons in the surrounding areas. All patients presenting to and managed in the Trauma Unit at CMJAH have a Medibank Assessment Form filled out detailing: demographics, pre-hospital management, primary survey, secondary survey, management in the trauma unit and investigations. This hospital is an academic facility and, hence, patients treated here consent to data being used anonymously for research.
The Statistica V8 application was used to analyse the data collected on the Medibank Assessment Forms filled out by the attending doctors. A p-value of <0>
Ethical and legal considerations
Ethics through the Wits Ethics Committee was obtained: Human Research Ethics Committee (HREC).
The author(s) received no financial support for this article's research, authorship, and/or publication
A total of 18, 087 patients were reviewed in this study with ages ranging from 1-92 years as this encompassed all the patients presenting to this unit and all mechanisms of injury were recorded (Figure 1).
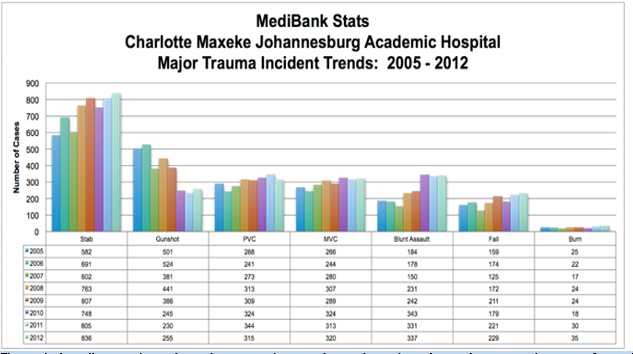
Figure 1: The graph above illustrates the incidence of various mechanisms of injury during the study period comparatively per year. It is evident that penetrating injuries have the highest occurrence, followed by blunt and burn injuries. Overall, all mechanisms of injury over the years are on an incline, except for gunshot injuries, which seem to be declining. Penetrating trauma was seen in 48.64% of cases, blunt trauma in 47.16%, and 1.06% were burns incidence.
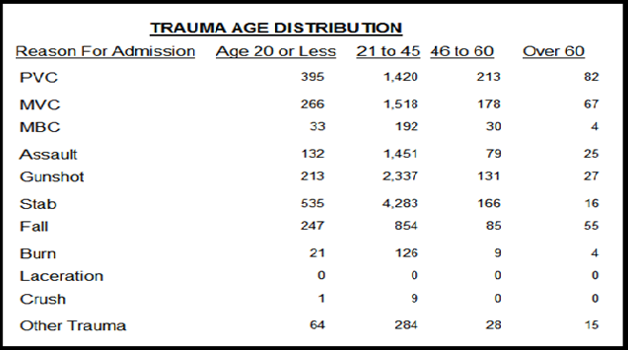
Figure 2: The table above illustrates the mechanism of injury with age distribution with the majority of injuries occurring in the 21-45year age group.
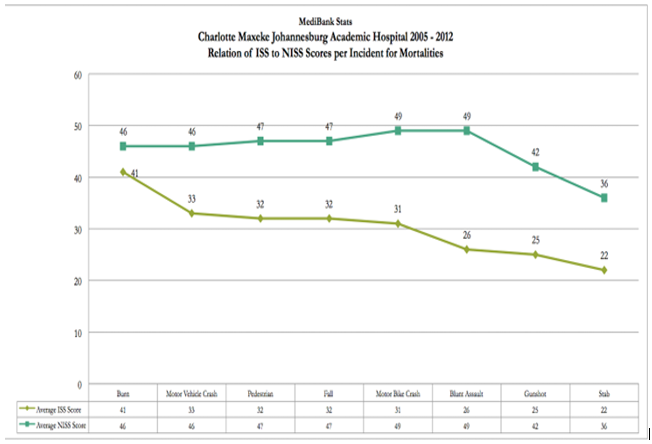
Figure 3: The graph below shows the ISS and NISS relation to mortality in accordance with various mechanisms of injury. Blunt assaults and burns have relatively high mortalities but vary according to ISS and NISS. Penetrating injuries have relatively lower mortalities than blunt injury.
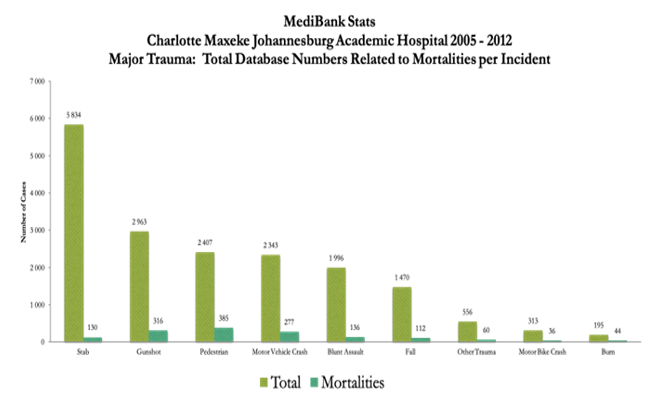
Figure 4: the graph above shows the overall mortalities over the study period according to the mechanism of injury. As can be seen, penetrating injuries have the highest incidences but with relatively low moralities. Blunt injuries including MVC, PVC, blunt assaults, fall from height have lower incidences but relatively higher mortality rates. Burns have the least incidence with a high mortality.
As demonstrated by the results, the highest incidence of trauma occurs in the 21-45year age group with penetrating injuries, particularly stabbings, presenting as the most common (almost three times that of blunt injuries) mechanism of injury followed by GSW injuries (Figure 2). PVCs and MVCs have had a steadily increasing incidence over the years, but blunt injuries initially presenting at a lower rate than the former two becomes the higher incidence rate amongst the three by the year 2012. However, overall, penetrating injuries involving stabs and GSW presented with the highest incidence throughout the years. Blunt injuries of PVC, MVC, and blunt assaults followed in incidence, but it can be noted that their occurrence was on the rise as the years went on (Figure 1). This is in keeping with a study conducted in Nigeria that showed males accounted for two-thirds of death rates and were mainly due to road traffic accident deaths [10].
In this review, when comparing the Injury Severity Score (ISS) and New Injury Severity Score (NISS) to the Probability of Survival (Ps), stab injuries have the lowest mortality, followed by blunt assault then gunshot injuries (Figure 3). However, the stabs have the highest incidence, with gunshot injuries occurring approximately at half the rate of stabs. The above results highlight where the greatest burden of disease emanates from. Firstly, penetrating injuries (Stabs and GSW) have the highest incidence yearly. This is followed by blunt injuries (PVC, MVC, blunt assault, and fall from height), and this once again is in keeping with a study conducted in San Francisco demonstrating GSW, followed by MVC and falls being the predominant mechanisms of injury [11]. Burns make up the lowest incidence of trauma compared to penetrating and blunt injuries. However, across the board, all of the above mechanisms of injury are on the increase year after year, except for gunshot injuries.
In comparison, although penetrating injuries had the highest incidence, their relative mortality is lower according to the ISS and NISS. In stark contrast, burns and blunt assaults have relatively high mortality relative to their incidence. A cross-sectional study found that central nervous system injuries were the most frequent cause of death, followed by haemorrhage and organ failure in the first 7 days of admission [11]. As expected, blunt injuries from PVCs, MVCs, MBCs, and Fall from height have relatively high mortality that is likely associated with polytrauma injuries with higher ISS and NISS scores (Figure 4). A retrospective audit done showed that the three main causes of trauma-related deaths were head injuries followed by polytrauma and chest injuries [12].
The methodology bias of the retrospective audit is a limitation of this study. As the patient physiology on presentation is not included this does not allow for accurate assessment of predicted mortality. The assessment of psychosocial influences on the various trauma patients was not taken to account, i.e.: unemployment, alcohol abuse, family relationships, and previous trauma. This could significantly attribute to the groups presenting in the trauma unit. The CMJAH Trauma Unit does not have a dedicated burns unit, this may account for the proportionately higher mortality rates seen in burns patients.
The data reviewed in this study is old and review of more recent data may be more useful to assess the burden of trauma and the mechanisms of injury with significantly high mortality rates in order to audit and assess areas of improvement in resuscitation and management.
The highest in-hospital mortality was due to burns patients even though the incidence of this mechanism was relatively low, followed by PVC patients affecting the predominantly young male population which had a high incidence of occurrence and high mortality. Poor probability of survival was demonstrated amongst Motor Vehicle Crashes and Motorbike Crashes, and PVCs. The high mortality of blunt assaults is associated with a low probability of survival even though their incidence is lower compared to the penetrating trauma. The overall in-hospital trauma mortality rate as evidenced by this study was 8.27%. This study demonstrated the high incidence of penetrating injuries, although the overall mortality of this mechanism was low, followed by blunt injuries with more than double the mortality of penetrating injuries.
The author(s) declared no potential conflicts of interest concerning this article's research, authorship, and/or publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
