
Case Report | DOI: https://doi.org/10.31579/2692-9759/157
1Chief, Pediatric and Adult Cardiology, Prakash Heart Station, Nirala Nagar, Lucknow, UP, India.
2Cardiac Technician, Prakash Heart Station, Nirala Nagar, Lucknow, UP, India.
*Corresponding Author: Akhil Mehrotra, Chief, Pediatric and Adult Cardiology, Prakash Heart Station, Nirala Nagar, Lucknow, UP, India.
Citation: Akhil Mehrotra, Faiz Illahi Siddiqui, (2025), Transthoracic Echocardiography: Dextrocardia with Situs Inversus accompanied by myriads of Congenital Cardiac Defects. A Rare Case Report, Cardiology Research and Reports, 7(3); DOI:10.31579/2692-9759/157
Copyright: © 2025, Akhil Mehrotra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 March 2025 | Accepted: 08 April 2025 | Published: 15 April 2025
Keywords: dextrocardia; situs inversus; dorv; pulmonary valvular stenosis; cavcd; hypoplastic mitral valve annulus; complete av septal defect, malposition of great arteries
Transthoracic echocardiography (TTE) for the detection of congenital heart defects (CHD), is an indispensable and first line imaging technique. A nine year old female child presented to us with breathlessness, central cyanosis and clubbing of all the fingers and toes. We performed a TTE in a structured manner by the sequential segmental approach (SSA) and were able to establish a categorical diagnosis of Dextrocardia, Situs Inversus accompanied by a conundrum of congenital cardiac defects.
Dextrocardia with situs inversus (SI) incidence is 1-2 per 20,000 normal population [1-3] and about 2% - 5% have associated congenital cardiac disease [4, 5]. Currently, TTE is the standard number one imaging technique in the diagnostic assessment of CHD [6-9] (Figure 1), due to its characteristics of versatility, non-invasiveness and probability.
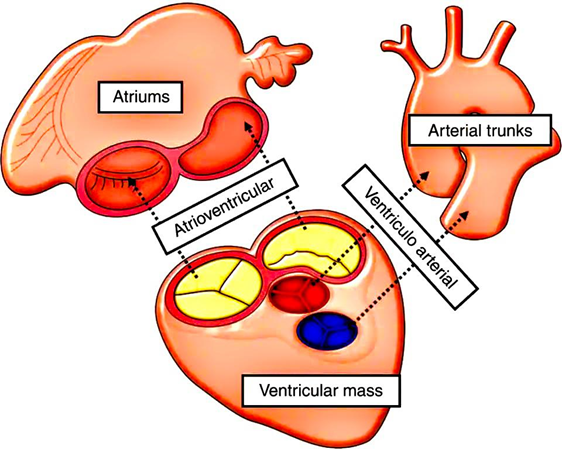
Figure 1: Sequential segmental analysis. Diagrammatic representation of segments of the heart (1. atria; 2. ventricles; 3. great arteries) and bridging components (atrio-ventricular canal and infundibulum).
The SSA comprises of numerous echocardiographic interpretative imaging steps for methodical assessment of morphology of the heart. The stepwise approach enables precise recognition of the morphological anatomy of heart, in patients of CHD [10] (Figure 2).
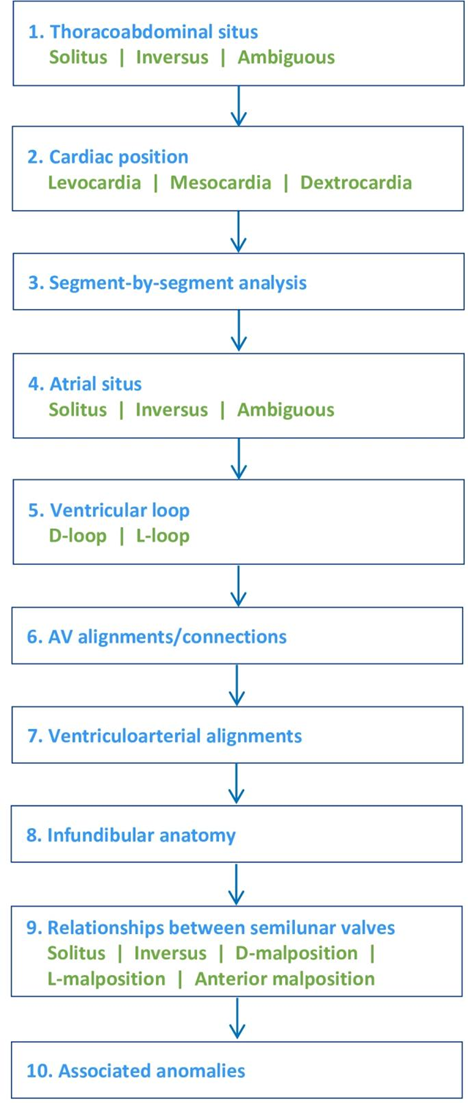
Figure 2: Stepwise approach to sequential segmental analysis (SSA). How to proceed in the SSA is elaborated in the figure 2.
Here, we are reporting a case of 9 year old cyanotic female child suffering from confirmed CHD. We performed a succinct SSA with TTE and were able to establish a detailed diagnosis of CHD encompassing myriads of anomalies: Dextrocardia, Situs inversus, Malposition of great arteries (MGA), Double outlet right ventricle (DORV), Pulmonary valvular stenosis (PS), Complete atrio-ventricular canal defect (CAVCD), Hypoplastic mitral valve annulus, left atrium (LA), left ventricle and accompanied with left aortic arch.
A private hospital referred a 9 year old female child to us for comprehensive color echocardiography and opinion regarding treatment of cyanotic CHD.
The parents provided the history of cyanosis since birth, shortness of breath and failure to thrive. On clinical examination, the child was slim and lean, very active and lively. Pectus excavatum was noticed along with prominent chest wall. Central cyanosis was obvious over her lips, fingers tips and toes. Conspicuous clubbing was also noticed over nails of fingers and toes (Figure 3).

Figure 3: Facial appearance and other clinical features in our index patient. (A) Facial appearance; (B) Chest wall abnormalities- Pectus excavatum was observed alongwith prominent chest wall; left > right; (C) Clubbing and cyanosis was detected in all the fingers; (D) Clubbing and cyanosis was noticed in all the toes.
The child’s weight was 13 kg, height was 168 cm, BP was 90/60 mmHg, HR was 105/min, respiratory rate was 20/min and SPO2 was 72% at room air. Cardiac examination revealed apical impulse in the right chest, in the 4th intercostal space, just medial to the mid-clavicular line. A grade 3/6 ejection systolic murmur was best heard in the pulmonary area of right chest. P2 component was soft. No clicks or gallop sound were heard.
Xray chest (PA) view demonstrated dextrocardia with reduced pulmonary arterial flow (Figure 4).

Figure 4: X-ray chest (PA) view- Dextrocardia is recognized. The pulmonary blood flow is decreased.
Resting ECG showed the following features (Figure 5):
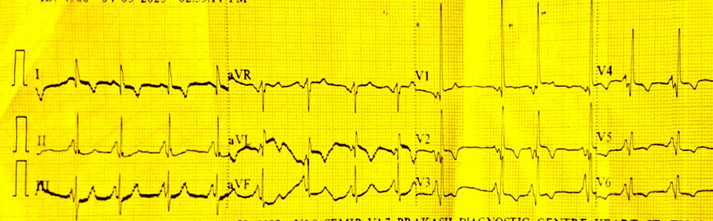
Figure 5: Resting ECG demonstrated: Ventricular rate of 96/ min with a normal sinus rhythm T wave inversion in L1, AVL, V2- V6 , Tall R waves in V1 (consistent with right ventricular hypertrophy), lack of normal R wave progression in precordial leads.
Transthoracic Echocardiography
TTE assessments according to SSA, were performed by employing My Lab X7 4D XStrain echocardiography machine, Esaote, Italy.
M-mode Echocardiography
For estimating various ventricular parameters (Table 1), M-mode echo was conducted.
| Measurements | LV | RV |
| IVS d | 6.4 | 7.2 |
| ID d | 12.1 | 21.4 |
| PW d | 4.3 | 8.3 |
| IVS s | 7.2 | 7.0 |
| ID s | 8.0 | 16.6 |
| PW s | 5.9 | 8.3 |
| EF | 67 % | 48 % |
| %FS | 33 % | 22 % |
| EDV | 3.4 ml | 15.2 ml |
| ESV | 1.1 ml | 7.9 ml |
| SV | 2.3 ml | 7.3 ml |
| Mass | 9 g | 34 g |
| IVS, interventricular septum, ID, internal dimension; PW, posterior wall; values are mentioned in millimeter. | ||
Summary of M-mode echocardiography
M-mode echocardiography depicted dilated RV with mildly reduced RVEF (48 %). On the contrary the LV was hypoplastic with normal LV systolic function LVEF (67 %).
2Dimensional-Transthoracic Echocardiography
2Dimensional transthoracic echocardiography (TTE) was conducted in explicit detail and it demonstrated the following features (Figures 6-18):
Both the great arteries are arising from the morphological right ventricle.
A subaortic conus was recognised
Aorta is anterior and to the right of PA
PA is posterior and to the left of aorta
Common AV valve (CAAV) orifice
Common AV valve with separate MV (Right AV valve) and TV (Left AV valve) orifices
MV orifice was hypoplastic and TV leaflets were large and thickened.
Size: 9.8 mm.
Ostium primum type.
Lt. to Rt. shunt.
Size 15.9 mm.
Inlet type
Lt. to Rt. shunt.
The chordae of left AV valve (Tricuspid valve) were attached to the lateral wall of RV and RV apex. MV chordae were attached to ventricular septal crest and lateral wall of LV.
On color flow mapping a mild, central tricuspid regurgitation jet was identified in RA. The jet area was 2.80 sqcm.
PV domed
Peak/mean gradient across PV = 83/64 mmHg.
Hypoplasia of PV annulus, MPA, LPA and RPA
PV annulus (D): 4.0 mm
MPA (D) : 5.3 mm
LPA (D) : 3.6 mm
RPA (D) : 3.5 mm
Morphological LV was hypoplastic
Normal LV systolic function LVEF (67 %)
Peak/mean gradient across PV = 83/64 mmHg.
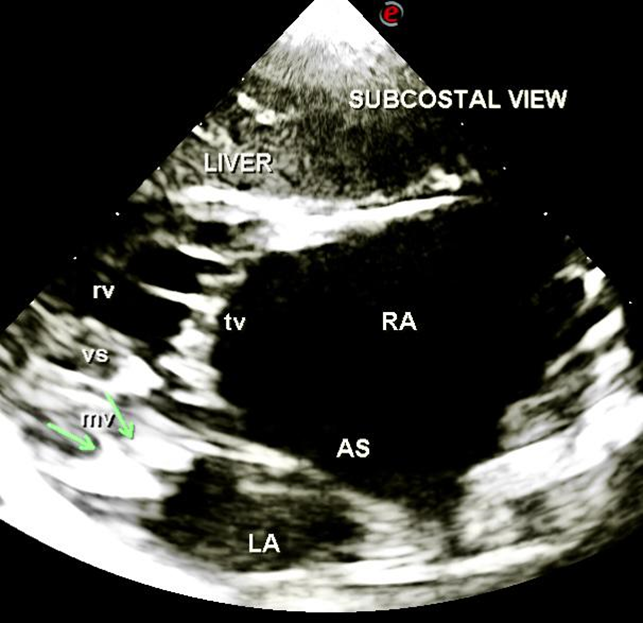
Figure 6: Dextrocardia. Subcostal view identifies dextrocardia.

Figure 7: Situs Inversus: In the subcostal view aorta is right sided and inferior vena cava (ivc) is left sided. Liver is also left sided ; ao, aorta; ivc, inferior vena cava; sp, spine.
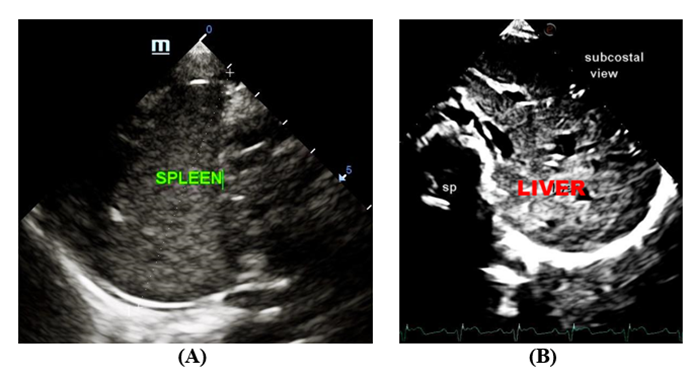
Figure 8: Situs Inversus. Ultrasound of abdomen reveals: (A) Right sided spleen; (B) Left sided Liver; sp, spine.
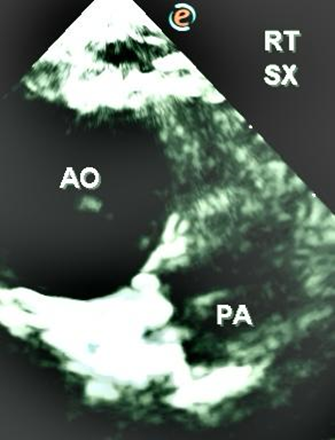
Figure 9: Malposition of great arteries. In the SX view from the right chest shows aorta is anterior and to the right of pulmonary artery and pulmonary artery is posterior and to the left of aorta.
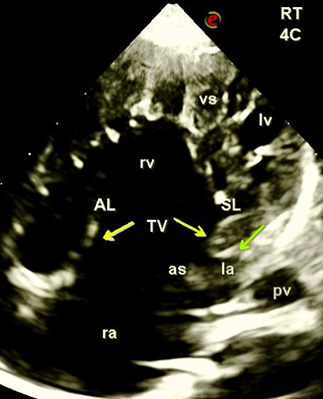
Figure 10: Apical 4C view from right chest with cursor probe placed at 9 o’clock position. Morphological right ventricle was dilated and morphological LV was hypoplastic; la, left atrium; lv, left ventricle; ra, right atrium; rv, right ventricle; vs, ventricular septum; TV, tricuspid valve; as, atrial septum; AL, anterior leaflet; SL, septal leaflet.
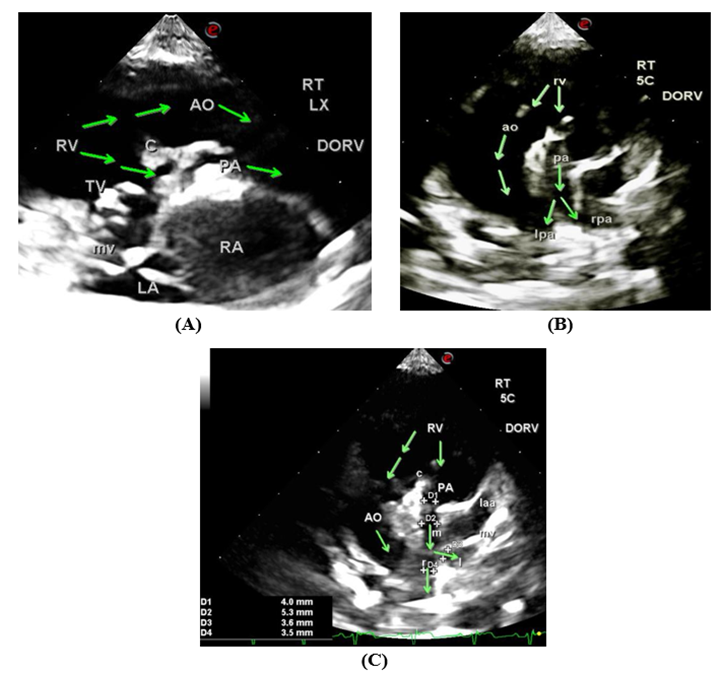
Figure 11: Double outlet right ventricle. (A) and (B) In the right LX and right apical 5C view both great arteries are arising from morphological RV. Aorta was anterior and pulmonary artery was posterior and hypoplastic. Pulmonary valve was domed. A subaortic conus was also recognized. (C) In the right apical 5C view, the diameter of hypoplasic pulmonary arteries was estimated. PV annulus, MPA, LPA and RPA diameter was 4.0 mm, 5.3 mm, 3.5 mm and 3.6 mm respectively; DORV, double outlet right ventricle, Ao, aorta, PA, pulmonary artery; C, conus; LA, left atrium; TV, tricuspid valve; RV, right ventricle; mv, mitral valve; l, left pulmonary artery, r, right pulmonary artery; vs, ventricular septum.
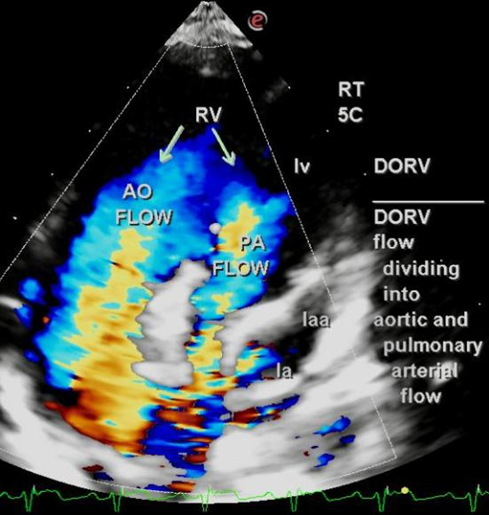
Figure 12: Color flow mapping in apical 5C view from right chest. The classical movement of blood flow in DORV is depicted. The anterior aortic flow is non turbulent and the posterior pulmonary arterial flow is highly turbulent because of severe pulmonary valvular stenosis; la, left atrium; lv ,left ventricle; laa, left atrial appendage; AO, aorta; PA, pulmonary artery.
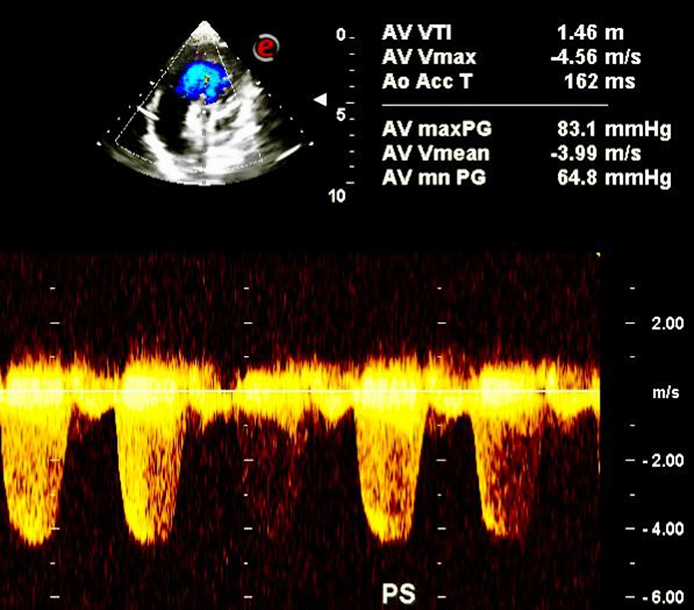
Figure 13: Color flow mapping across pulmonary valve identifies pulmonary valvular stenosis with a peak/mean gradient of 83.1/ 64.8 mmHg; PS, pulmonary stenosis.

Figure 14: Complete atrio-ventricular canal defect (CAVCD). (A) Apical 4C view from right chest portrays common AV valve with two components: large anterior and septal leaflet of TV and bileaflet MV. (B) Apical 4C view from right chest discerns the ostium primum ASD (**) CAVCD (****); mv, mitral valve; lv, left ventricle; vs, ventricular septum; mb, moderator band; rv, right ventricle; ra, right atrium; AL, anterior leaflet of TV; SL, septal leaflet of TV; as, atrial septum; TV, tricuspid valve.
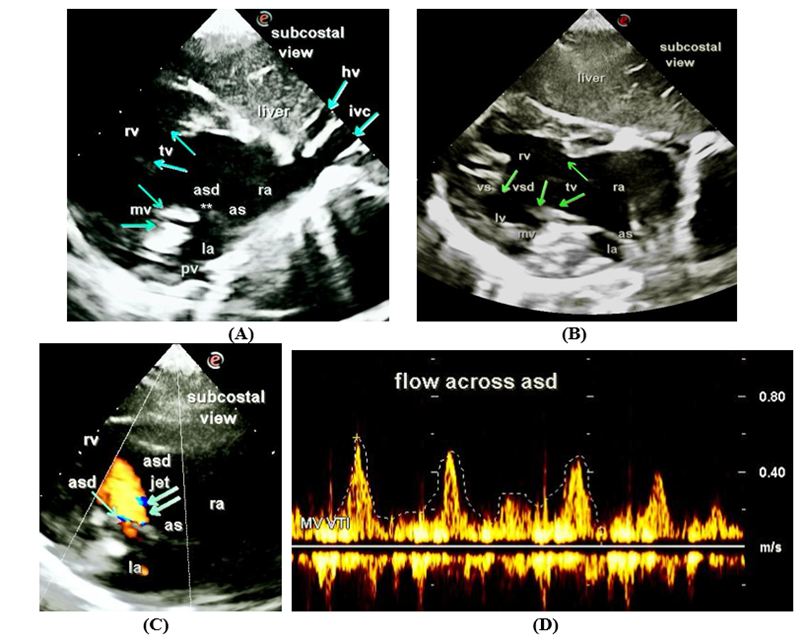
Figure 15: Complete AV canal defect in the subcostal view. (A) Large TV annulus, TV leaflets, hypoplastic MV annulus, ostium primum ASD, dilated RA and Hypoplastic LA were deciphered; (B) Large inlet VSD dilated RV and hypoplastic LV were exhibited; (C) On color flow imaging an ASD jet is displayed across ostium primum ASD; (D) Peak/mean gradient across ASD was 2.1/0.7 mmHg.
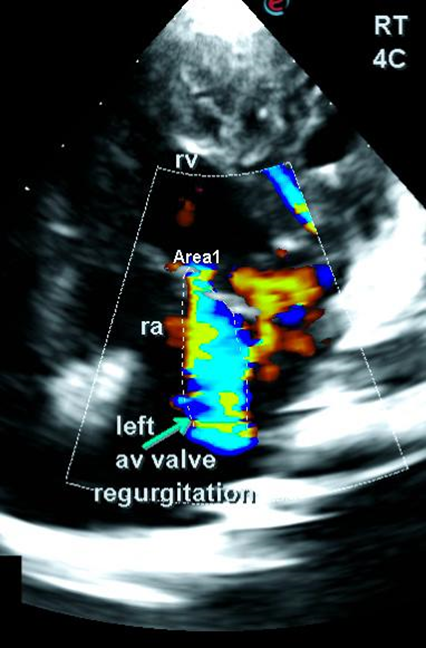
Figure 16: Left AV valve (TV) regurgitation. Apical 4C view from right chest shows mild TV regurgitation.
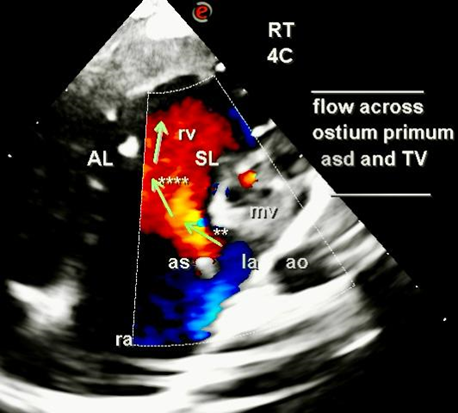
Figure 17: Direction of blood flow across ostium primum ASD and TV in the apical 4C view, imaged from right chest. Color flow mapping across ostium primum ASD is denoted as (**) and across TV is denoted as (****). Green arrows portray the direction of blood across ASD and TV; la, left atrium; ra, right atrium; rv, right ventricle; as, atrial septum; ao, aorta; mv, mitral valve; AL, anterior leaflet of tricuspid valve.
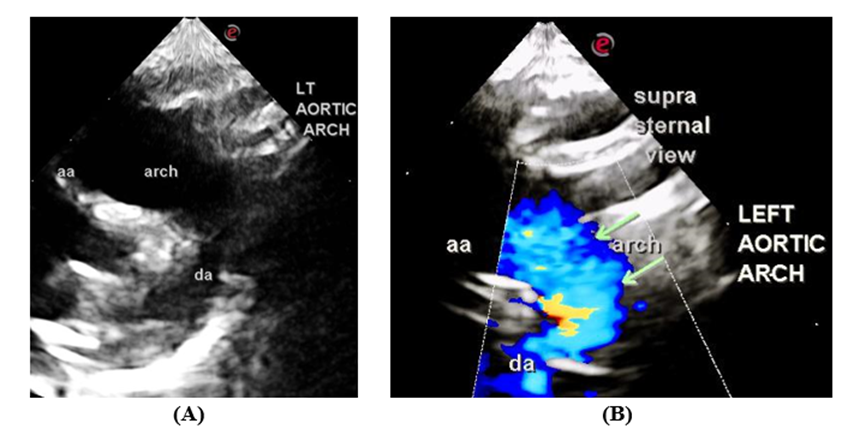
Figure 18: Suprasternal view. (A) Left aortic arch; (B) Color flow mapping demonstrating non turbulent blood flow in the left aortic arch; aa, ascending aorta; da, descending aorta.
Summary of color echocardiography
On TTE, in our index patient, we detected numerous cardiac defects: Dextrocardia, Situs inversus, Malposition of great arteries, DORV, PS, CAVCD-Rastelli Type B, Hypoplastic MV annulus, LA, and LV accompanied by left aortic arch. Due to the presence of significant breathlessness and central cyanosis, we suggested to the parents to consult a tertiary care cardiovascular institute for palliative or corrective surgery.
A “segmental approach” was advocated by Richard Van Praagh in 1972. According to this methodology the heart structure were classified into three crucial components: 1. Atria, 2.Ventricles and 3.The great arteries [11]. Nonetheless, Anderson had his exclusive version of segmental approach [10]. Undoubtedly, multiple imaging technique including, Cardiac MRI, Cardiac CT and TEE play a paramount role in the detection and confirmation of CHD. Currently, TTE , because of its non-invasive nature, free availability and adaptability, stands out as a number one imaging technique in the diagnosis of CHD [6-9].
In SIT, around 2-5% of patients have associated cardiac anomalies [4, 5]. Typically, normal life expectancy is observed in patients with situs inversus (SI) and dextrocardia (DXA) unaccompanied by other CHD. Nevertheless, in those accompanied by CHD, reduced life span is expected, determined by the seriousness of the CHD [12]. Clinical manifestation in the patient is variable depending on associated malformations [13-15].
A perplexing mystery of congenital heart defects
The salient TTE features in our index patient, were deeply puzzling and mystifying. However, with great determination and endurance, we were able to construct a complex albeit a clinching diagnosis of SI, DXA, Malposition of great arteries, DORV, Pulmonary valvular stenosis, CAVCD, hypoplastic MV annulus, LA, LV and left aortic arch. Despite these complexities our patient has survived into mid-childhood with significant symptomatology of breathlessness, cyanosis and clubbing, due to a balanced circulation.
We have considerably searched the literature and were unable to find a similar case report. Nonetheless, many authors have published rare case reports of SI, DXA with multiple and or complex CHD [16-20]. We are mentioning here three such interesting complex case reports A “Triply Reversed Heart” [17] comprising of SI, DXA and congenitally corrected TGA in 57 year old female, was published by Chang et al [17]. A noteworthy report of Nigerian infant who presented with SI, DXA with multiple cardiac anomalies (Common atrium, CAVCD, Pulmonary atresia and PDA) [20]. Importantly, Chang et al published 2 case report of complex congenital heart disease in whom cardiac transplantation was performed. One of them was afflicted with dextrocardia, situs inversus with single ventricle, D-TGA, severe valvular PS, left aortic arch and bilateral SVC.
The uniqueness of our case was concomitant existence of CAVCD, DORV, Malposition of great arteries and PS creating a complicated hemodynamics.
Our patient spotlights, the presence of Dextrocardia, situs inversus, CAVCD, DORV and malposition of great arteries accompanied by severe PS and left aortic arch, which has not been described in literature. Complex congenital cardiac defects require a considerable amount of knowledge of CHD and moreover strong determination and endurance is necessary, while performing the TTE. The procedure may consume plenty of time in a busy practice of non-invasive cardiologist. The patient being at high risk of mortality, was referred to a tertiary care Cardiovascular institute for a definitive corrective/palliative surgery.
We are deeply indebted to Faiz Illahi Siddiqui, our co-editor, who has innovated the scheme and presentation of Figure 2 of our manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
