
Review ariticle | DOI: https://doi.org/10.31579/2690-4861/630
1Department of Cardiac Surgery, University Hospital Schleswig-Holstein (UKSH), Kiel, Germany.
2DZHK (German Centre for Cardiovascular Research), Partner Site Hamburg/Kiel/Lübeck, Hamburg, Germany.
3Department of Cardiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland.
4 Centre for Cardiovascular Innovation, St Paul’s and Vancouver General Hospital, Vancouver, Canada.
5Cardiovascular Translational Laboratory, Providence Research & Centre for Heart Lung Innovation, Vancouver, Canada.
6Centre for Heart Valve Innovation, St. Paul’s Hospital, University of British Columbia, Vancouver, British Columbia, Canada.
7Department of Cardiology and Angiology, University Hospital Schleswig-Holstein (UKSH), Kiel, Germany.
8Department of Vascular Surgery, University Hospital Schleswig-Holstein (UKSH), Kiel, Germany (R.B.).
*Corresponding Author: Georg Lutter, Department of Cardiac Surgery, University Hospital Schleswig-Holstein (UKSH), Kiel, Germany.
Citation: Zhang Xiling, Nina Sophie Pommert, David Meier, Stephanie L. Sellers, Hatim Seoudy, et al, (2025), Transcatheter Tricuspid Valve Replacement: will it take over? Review Article, International Journal of Clinical Case Reports and Reviews, 22(4); DOI:10.31579/2690-4861/630
Copyright: © 2025, Georg Lutter. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 November 2024 | Accepted: 17 December 2024 | Published: 22 January 2025
Keywords: tricuspid regurgitation; heart valve replacement; transcatheter; stents; clini-cal outcomes
Severe tricuspid regurgitation (TR) is a prevalent and challenging condition associated with poor survival outcomes and significant morbidtiy. Medical therapy alone often fails to provide adequate symptom relief, and standalone surgical intervention is liked to high mortality rates, making it a less favorable option unless combined with left-sided valve surgery.
The advent of transcatheter tricuspid interventions has provided new therapeutic possi-bilities, particularly for high-risk patients who are ineligible for conventional surgery. However, many patients remain unsuitable for transcatheter tricuspid repair, or achieve only limited benefits from such procedures. In this context, Transcatheter tricuspid valve replacement (TTVR) has rapidly emerged as a promising alternative, offering the po-tential for more effective treatment outcomes. This review explores the latest advance-ments in TTVR devices, highlights key clinical experiences, and discusses the chal-lenges and limitations of this evolving strategy. Additionally, we address patient selec-tion criteria, procedural outcomes, and future directions in the field, emphasizing the potential of TTVR to transform the management of severe TR.
Tricuspid regurgitation (TR) is a prevalent form of valvular heart disease with extensive research establishing its severity as an independent predictor of mortality[1]. The European Society of Cardiology / European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines recommend tricuspid valve repair or replacement for patients with moderate to severe primary or secondary TR, especially when performed in conjunction with left-sided heart surgery, as a Class I indication[2]. However, managing isolated TR, particularly when accompanied by right ventricular dysfunction, remains challenging, with perioperative mortality rates reaching up to 10%[2].
Transcatheter tricuspid valve intervention (TTVI) offers an innovative therapeutic approach aimed at mitigating the risks associated with conventional surgical procedures. Moreover, compared to treatment with oral medications alone, TTVI may be associated with higher survival rates and lower rates of heart failure rehospitalization[3]. Recent advancements have introduced various TTVI techniques, providing minimally invasive alternatives that have shown promising initial results. The spectrum of TTVI includes both transcatheter tricuspid valve repair (TTVr) and replacement (TTVR), each tailored to specific patient needs. While TTVr has demonstrated commendable safety and efficacy, anatomical considerations such as unfavorable tricuspid valve morphology, or excessive annular dilatation with large coaptation gap may preclude the use of edge-to-edge repair. For these individuals, TTVR sometimes represents the only potential alternative[4].
This review will comprehensively examine the different types of valves currently available and their respective statuses in clinical trials. Furthermore, it will analyze the ongoing challenges and developmental trends in the field of TTVR, emphasizing its potential to significantly advance the therapeutic landscape for TR.
Transcatheter Tricuspid Valve Replacement-Current Landscape
Since the first-in-human implantation, TTVR has advanced rapidly[5]. Early devices were temporarily set aside due to technical limitations and the complex anatomy of the tricuspid valve, which posed challenges in initial design and clinical application. However, with advancements in imaging navigation, catheter technology, and materials science, TTVR techniques have gradually improved, now encompassing two primary approaches: orthotopic and heterotopic replacement. Orthotopic replacement involves directly implanting a new valve at the tricuspid valve site, while heterotopic replacement positions the valve stent within the vena cava[6]. Multiple new devices are currently entering clinical trials, with some demonstrating significant efficacy in high-risk patients, thereby promoting the standardization and diversification of TTVR techniques. Table 1 shows the orthotopic and heterotopic tricuspid valve replacement devices currently under development and tested.
| Device | Manufacturer | Access | Anchoring | Trials |
| Orthotopic | ||||
| VDyne | VDyne | Transfemoral | Septal anchor | NCT05797519 |
| Cardiovalve | Venus MedTech | Transfemoral | TV leaflets | NCT04100720 |
LuX-Valve Lux-Valve Plus | Jenscare Biotechnology | Transatrial Transjugular | Septal anchor and anterior leaflet grasp | NCT05436028 NCT05436028 |
| EVOQUE* | Edwards Lifescience | Transfemoral | TV leaflets/ annulus | NCT04221490 NCT04482062 |
| Intrepid | Medtronic | Transfemoral | Perimeter oversizing | NCT04433065 |
| Trisol | Trisol Medical | Transjugular | Tricuspid annulus | NCT04905017 |
| TRiCares | TRiCares | Transfemoral | Tricuspid annulus | NCT05126030 |
| NaviGate | NaviGate Cardiac Structures | Transatrial | TV leaflets/ annulus | N/A |
| Heterotopic | ||||
| Sapien XT | Edwards Lifescience | Transfemoral | Preceding stent implantation | NCT02339974 |
| TricValve | P+F Products + Features | Transfemoral | N/A | NCT04141137 |
| Tricento | MEDIRA | Transfemoral | N/A | N/A |
Table 1: Orthotopic and heterotopic tricuspid valve replacement devices currently under development and tested. The Evoque valved stent received CE mark*. The scaffolds of these valved stents are made of nitinol. TV: tricuspid valve
Orthotopic Transcatheter Tricuspid Valve Replacement
VDyne
The VDyne valve (VDyne, Inc., Maple Grove, MN, USA, Fig. 1A) consists of a dual-frame nitinol prosthesis, housing a 30 mm porcine tri-leaflet valve. The outer frame is asymmetrically designed (like an oyster, pear-like) with five different fixation mechanisms: a tab at the right ventricular outflow tract, small tabs at the lateral or free wall of the right ventricle (RV), a small tab at the postero-septal wall, and a large tab beyond the posterior annulus. This design aims to anatomically conform to the native annulus while allowing for minor oversizing (larger atrial and ventricular hub). The valve is available in five sizes, suitable for any tricuspid annulus with a circumference of up to 180 mm. Additional sizes under development. The valve is deployed using a single 28Fr catheter and features a unique side-loading delivery system in which the prosthesis is crimped vertically rather than radially. Even after full expansion and positioning it can be fully recaptured[7].
The initial thirteen patients receiving the 3rd generation of human implants were all successfully treated[7]. Early feasibility trials are currently underway in multiple regions globally (VISTA, NCT05797519), and the device has been designated as a breakthrough device by the U.S. Food and Drug Administration (FDA).
Cardiovalve
The Cardiovalve (Venus MedTech, Hangzhou, China, Fig. 1B) device comprises a self-expanding nitinol stent and bovine pericardial leaflets. It
features an atrial flange to assist with anchoring and incorporates leaflet capture technology to prevent valve migration. The valve is delivered via a low-profile 28F delivery system through the femoral vein. The Cardiovalve is suitable for patients with an annulus diameter ranging from 36 to 55 mm and a right ventricular length exceeding 45 mm[8].
Currently, an early feasibility study of Cardio valve is being conducted in the United States (NCT04100720), enrolling 15 patients. The primary endpoints include the absence of device- or procedure-related adverse events within 30 days post-procedure. However, this study has been intermittently interrupted due to technical issues. The new TARGET trial has commenced (NCT05486832), aiming to enroll 100 patients to evaluate the safety and performance of the Cardio valve system.
LuX-Valve
The LuX-Valve (Jenscare Biotechnology, Ningbo, China, Fig. 1C) is a self-expanding bovine pericardial valve also mounted on a nitinol stent. It stands out from traditional stent devices with its unique anchoring mechanism, which secures placement through anterior leaflet clamps and a ventricular anchor, significantly reducing stress on the cardiac walls and minimizing the risk of complications.
This innovative bioprosthesis is available in four sizes, ranging from 30 to 55 mm, and includes eight skirted atrial disc options, making it suitable for native tricuspid annulus diameters from 25 to 50 mm. Implantation is facilitated by a flexible 32Fr delivery system via a transatrial approach, enhancing procedural adaptability and patient recovery[9].
In clinical evaluations, Lu et al.[9] documented the first deployment of the LuX-Valve for transcatheter tricuspid valve replacement in patients at high risk for tricuspid regurgitation. The procedure was successful in all 12 patients, with 90.9% exhibiting no residual tricuspid regurgitation at the 30-day postoperative follow-up.
Additionally, Sun et al.[10] observed a significant reduction in tricuspid regurgitation severity over a 12-month period in a similar patient cohort, although one patient succumbed to right heart failure within three months post-operation.
The second-generation LuX-Valve is transitioning to a transjugular approach. The first-in-human study of the LuX-Valve Plus demonstrated significant results, with all patients successfully receiving the implant and achieving none/trace TR within 30 days[11]. Results from 76 patients under early compassionate use showed that at 1 month, 95.0% of patients had TR of ≤2+, and 86.8% had TR of ≤1+[12].
Currently, multiple studies (NCT06568003, NCT05436028) are evaluating the safety and efficacy of transjugular tricuspid valve replacement using the LuX-Valve Plus system.
Evoque
The EVOQUE tricuspid valve replacement system (Edwards Lifescience, Irvine, CA, USA, Fig. 1D) features a self-expanding nitinol stent, bovine pericardial leaflets, an intra-annular sealing skirt, and anchoring devices. This system is available in three sizes: In 44 mm, 48 mm, and in 52 mm. It utilizes a low-profile, multi-plane 28Fr delivery system designed for femoral artery implantation, making it adaptable to a wide range of anatomical structures.
The TRISCEND trial (NCT04221490) evaluated the safety and performance of the EVOQUE system in patients with symptomatic TR of at least moderate severity, despite receiving medical therapy. At 1 year, 97.6% of implanted patients had TR of mild or less, with 69.0% exhibiting none or only trace TR[13].
none or only trace TR[13].
The TRISCEND II trial (NCT04482062) aims to assess the safety and efficacy of the EVOQUE system compared to optimal medical therapy (OMT) for patients with at least severe TR. Initial six-month follow-up results from the first 150 patients demonstrated that the EVOQUE system effectively eliminated TR in approximately 78% of participants, with nearly 99?hieving a TR severity of moderate or less, and about 94% reaching a severity of mild or less[14]. Results from the second-phase TRISCEND II trial, involving 400 patients, indicated that at 1 year, 72.6% of patients had no residual tricuspid regurgitation, 22.6% had mild regurgitation, 3.8% had moderate regurgitation, and 0.9% had severe regurgitation. Although most patients experience a significant reduction in regurgitation severity, the incidence of important safety outcomes also warrants attention, including 30-day all-cause mortality (3.5%), major bleeding within 30 days (10.4%), and new pacemaker implantation within 1 year (17.8%)[15]. The EVOQUE tricuspid valve replacement system has received Conformité Européene (CE) mark from the European Union (2023) and approval from the U.S. FDA (2024).
Intrepid
The Intrepid valve (Medtronic Plc, Minneapolis, MN, USA, Fig. 1E), employs a sophisticated dual-structure design and was primarily used in the mitral position. This includes a 29 mm tri-leaflet bovine pericardial valve and is offered in three sizes: 43 mm, 46 mm, and 50 mm. The device is currently deployed via a 35Fr delivery system accessed through the femoral vein, with further enhancements in a 29Fr system underway.
The Intrepid valve is specifically designed for patients with mitral regurgitation (MR) and now also for tricuspid regurgitation. Following transcatheter mitral valve replacement using the transapical Intrepid valve, 99.5% (n=200) of patients had mild or less MR within 30 days, and all surviving patients (n=122) had mild or less MR at the 2-year follow-up[16]. A pre-market trial is currently underway (NCT03242642). Moreover, successful cases of compassionate use have been documented[17]. Presently, the early feasibility trial of the Intrepid TTVR (NCT04433065) is actively enrolling participants. This ongoing trial aims to evaluate the valve's safety and efficacy in clinical settings.
Trisol Valve
The Trisol valve (Trisol Medical, Yokneam, Israel, Fig. 1F) is constructed from a self-expanding conical nitinol alloy and features a single-leaflet circular bovine pericardial valve leaflet. This innovative design maximizes blood flow when the valve is open and minimizing resistance and turbulence, it enhances hemodynamic performance. Additionally, the valve employs a unique high closing volume design that can mitigate the impact of increased right ventricular afterload[18]. The valve’s stability is ensured by the application of axial force at the ventricular end and a polyester atrial skirt. Delivered via the transjugular route using a 30Fr system. The Trisol valve has already been successfully implanted in ten human patients[19].
Currently, an early feasibility study of the Trisol system (NCT04905017) is actively recruiting participants to further evaluate its clinical efficacy and safety.
TRiCares Topaz system
The TRiCares Topaz TTVR system (TRiCares SAS, Paris, France, Fig. 1G) utilizes a sophisticated self-expanding dual-stent design made from nitinol. The outer stent ensures robust sealing and anchorage while protecting the inner stent from deformations caused by RV contractions. This inner stent houses an independent porcine pericardial trileaflet valve, ensuring the valve’s integrity despite the external stent’s movements. The device is delivered through a 29Fr system accessed via the femoral vein.
The inaugural human implantation of the TRiCares Topaz system was conducted under compassionate use for treating TR, successfully implanted in two patients. During the three-month follow-up period, there were no reported mortalities or complications. However, a decline in RV function was observed three months post-implantation[20]. Currently, a pioneering clinical trial of the TRiCares Topaz trans-femoral tricuspid heart valve replacement system (TRICURE, NCT05126030) is active, focusing on evaluating its preliminary safety and efficacy parameters.
NaviGate
The NaviGate valve (NaviGate Cardiac Structures Inc., Lake Forest, CA, USA, Fig. 1H) features a self-expanding, tapered nitinol stent with tri-leaflet bovine pericardial leaflets. It secures the tricuspid valve using 12 anchoring screws and stabilizes with 12 atrial flaps. Available in six sizes ranging from 36 to 54 millimeters, the delivery system uses a 42Fr catheter sheath for transatrial or transjugular implantation. However, the transjugular approach has been abandoned due to the sheath size and complications such as difficulty in achieving coaxial alignment with the relatively simple delivery system[8].
Navia et al[5]. reported the first use of the NaviGate valve in two patients with TR, demonstrating its safety and feasibility. In a report on 32 patients treated with NaviGate under compassionate use, the implant success rate was 100%, with all patients achieving TR severity of grade 2 or less. The 30-day mortality rate was 12.5%[21]. In an early multicenter experience involving 30 patients, 26 (87%) had successful procedures, with 4 cases of device dislocation and 2 patients (5%) requiring conversion to open-heart surgery. Out of 24 patients, 18 (76%) had mild or less TR at discharge. The in-hospital mortality rate was 10%, and 4 patients (13%) died during follow-up, with an average follow-up duration of 127 ± 82 days[22]. Currently, the development of the NaviGate valve has been paused.
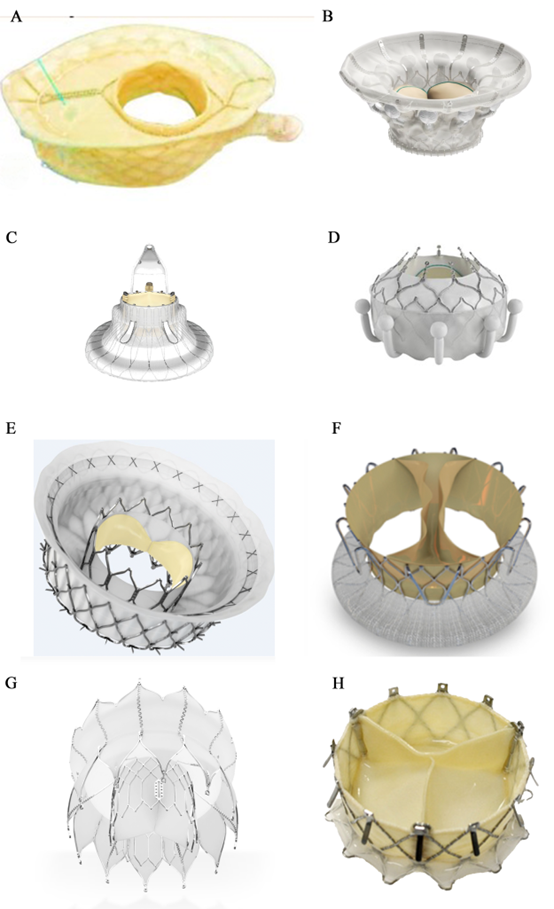
Figure 1. Orthotopic transcatheter valved stents: (A) The VDyne valve (VDyne, Inc., Maple Grove, MN, USA); (B) The Cardiovalve (Venus MedTech, Hangzhou, China); (C) The LuX-Valve (Jenscare Biotechnology, Ningbo, China); (D) The EVOQUE (Edwards Lifescience, Irvine, CA, USA); (E) The Intrepid valve (Medtronic Plc, Minneapolis, MN, USA); (F) The Trisol valve (Trisol Medical, Yokneam, Israel); (G) The TRiCares Topaz valve ((TRiCares SAS, Paris, France); (H) The NaviGate valve(NaviGate Cardiac Structures Inc., Lake Forest, CA, USA).
Heterotopic or caval tricuspid valve implantation
In some cases, transcatheter therapy is not feasible for certain patients. Although this method was abandoned in the past due to low efficacy and high mortality caused by technical limitations, innovations in recent years have led to the development of heterotpic or caval tricuspid valve implantation (CAVI) as a palliative alternative. This technique reduces venous reflux and improves right heart pressure through implantation in the inferior vena cava (IVC) or superior vena cava (SVC)[23, 24]. However, due to the risks of embolization, thrombosis, and hepatic vein obstruction, heterotopic implantation is more challenging than orthotopic implantation. Although CAVI does not significantly improve hemodynamics, it leads to notable improvements in quality of life and symptom relief[25]. Recent reports have indicated right heart remodeling after CAVI, suggesting its potential prognostic value[26].
Saien
The balloon-expandable Sapien valve series (Edwards Lifescience, Irvine, CA, USA) is widely used in aortic valve replacement. However, for the largest 29 mm Sapien XT valve, the diameter of the IVC remains too large, necessitating anchoring within a previously placed stent in the IVC.
The first human trial was conducted in 2013 and achieved acceptable results[27]. The TRICAVAL trial showed improvements in NYHA classification and quality of life post-procedure. However, the high rate of valve dislocation led to some patients requiring open-heart surgery[28]. Currently, there is no available data on the safety and efficacy of the Sapien valve for treating severe, refractory TR.
TricValve
The TricValve transcatheter bicaval valve system (P+F Products + Features, Vienna, Austria) consists of two self-expanding nitinol stent with bovine pericardial valves. The SVC valve is available in 25 mm and 29 mm sizes with a long skirt design to prevent paravalvular leakage (Fig. 2A). The IVC valve, sized at 31 mm and 35 mm, has a short skirt design to prevent hepatic vein embolization (Figure. 2B). The device is delivered via a 24Fr transfemoral delivery system and has received CE mark.
The first in-human implantation of the TricValve system was successful, with an 8-week follow-up showing improvements in venous congestion and symptoms related to right heart failure[6]. At 12 months post-implantation, the patient remained in NYHA class II with no symptoms of right heart failure[29]. Six-month results from the TRICUS EURO study (NCT04141137) in Europe showed that 79.4% of patients were in NYHA class I or II. Prosthesis dislocation occurred in 3% of patients but did not lead to serious consequences. Major bleeding was the primary serious complication, affecting 17.1% of patients.
TRICENTO
The TRICENTO (MEDIRA, Balingen, Germany, Fig. 2C) is a transcatheter bicaval valved stent currently in development, consisting of a self-expanding nitinol frame and porcine pericardial valves. The stent is custom-made based on pre-procedural imaging of the patient and delivered via a 24Fr delivery system. It is anchored within the IVC and SVC, aligning the stent valve with the native tricuspid valve. This design aims to prevent systolic blood backflow and ensure forward blood flow during diastole.
Early results from a multicenter study indicated that all stents were successfully implanted; however, three cases (14%) of asymptomatic stent fracture were observed during follow-up. At a median follow-up of 61 days, 65% of patients were in NYHA class I/II. Heart failure rehospitalization occurred in 19% of patients, and the one-year survival rate was 76%[30].
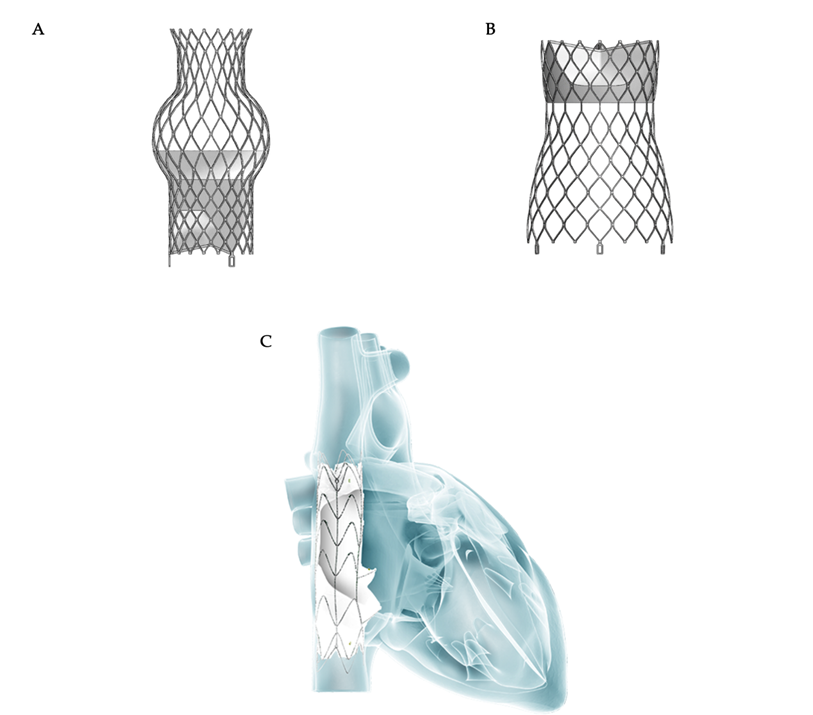
Figure 2. Heterotopic valve stent: (A, B) The TricValve transcatheter bicaval valve system (P+F Products + Features, Vienna, Austria); (C) The TRICENTO valved stent (MEDIRA, Balingen, Germany, Fig. 2C).
Timing of Intervention
For intervention in TR, currently only the ESC/ EACTS guidelines provide a Class I indication, which is for severe symptomatic TR. Wang et al[31]. compared the characteristics and outcomes of patients with Class I indications for severe symptomatic TR to those without such indications who underwent early surgery. The results showed significantly better short- and long-term outcomes in the early surgery group. Although the patients in Class I were older, with more pronounced symptoms and higher NYHA classifications, resulting in notable differences in baseline characteristics, the small sample size may also have influenced these findings. Nevertheless, this raises a new consideration: should we wait until Class I indications are met before intervening? In fact, the longer the wait for Class I indications, the greater the likelihood of developing risk factors such as right ventricular dysfunction, atrial fibrillation, and renal impairment, which in turn increase both surgical and long-term risks. With the emergence and advancement of new TTVI devices, a lower-risk surgical alternative is now available, potentially offering a new therapeutic strategy for early intervention in TR.
Patient selection
Clinically, secondary TR accounts for 90% of all TR cases[32]. In the early stages of the disease[33], where right ventricular dilation is not yet severe and tricuspid annular dilation occurs without significant leaflet tethering, transcatheter annuloplasty systems like the Cardioband. Tricuspid Valve Repair System are effective in repairing TR[34]. As the disease progresses to the second stage, further dilation of the RV and tricuspid annulus compromises leaflet coaptation, resulting in progressive leaflet tethering. At this juncture, the likelihood of achieving successful repair with an annuloplasty ring alone diminishes, necessitating a combination of edge-to-edge repair and annuloplasty[35, 36]. Notably, performing TTVR at this stage may completely resolve TR. Compared to transcatheter edge-to-edge repair, TTVR can attain a mild or lesser degree of residual TR in almost all patients within 30 days and 1-year (Figure 3)[9, 10, 37-41]. This resolution of TR can be maintained for up to one year, showcasing favorable functional outcomes that may positively influence long-term survival and functional status. In the third stage, as leaflet tethering further deteriorates, TR escalates to massive or torrential levels, rendering repair efforts potentially futile[42].
For patients with preserved or mildly to moderately impaired right ventricular function, TTVR should be considered the treatment of choice. In patients with end-stage heart failure who are on pharmacological treatment, employing TTVR or CAVI as a compassionate therapy is viable, but requires meticulous assessment of the patient’s condition[43].
Apart from survival rates, improvements in quality of life are also an important consideration. In both the TRILUMINATE pivotal trial[44] and the TRISCEND II pivotal trial[45], significant quality of life benefits were observed compared to OMT alone, and these benefits were associated with the degree of TR reduction. In the TRILUMINATE trial, improvements in Kansas City Cardiomyopathy Questionnaire Overall Summary Score scores were similar across groups, regardless of baseline TR severity. In contrast, in the TRISCEND II trial, the extent of quality of life improvement was directly related to baseline TR severity, with patients with more severe baseline TR experiencing greater health status benefits[45]. In addition, there were differences in the timeline of health status improvement between the two trials. In the TRILUMINATE Pivotal trial, the majority of patients showed significant improvement by 30 days post–transcatheter edge-to-edge repair. In contrast, in the TRISCEND II Pivotal trial, only moderate improvement was observed at 30 days, with continued improvement over the following six months[45]. This may be due to a transient increase in right ventricular afterload associated with TTVR.
Based on experience with mitral valve surgery, valve repair is generally prioritized over valve replacement, as conventional valve replacement surgery requires resection of subvalvular structures. This disruption to the subvalvular apparatus can damage the normal ventricular architecture, gradually leading to ventricular ‘sphericalization’ and impairing ventricular function[46, 47]. TTVR does not directly affect the papillary muscles and chordae tendineae; however, the implanted prosthetic valve stent may exert a mild mechanical effect on adjacent tissues. In certain cases, the position of the implant may slightly alter the geometry of the right ventricle, indirectly impacting the position and tension of the papillary muscles. Nevertheless, this effect is typically minimal and, in the vast majority of cases, does not lead to functional abnormalities.
CAVI is specifically engineered to alleviate congestion in patients with severe torrential TR who are either ineligible for surgery or present a high surgical risk. The fundamental mechanism of CAVI involves deploying a valved stent at the junction between the inferior vena cava and the right atrium to mitigate regurgitation. This intervention significantly reduces hepatic congestion, which subsequently improves hepatic and renal function, leading to decreased symptoms only of ascites and peripheral edema[48]. Moreover, CAVI has the potential to enhance right ventricular output, thereby augmenting cardiac output. Nonetheless, it is important to note that this approach is unlikely to ameliorate right ventricular function or influence the process of right ventricular reshape remodeling, thus categorizing it as a palliative procedure.
From the perspectives of safety and efficacy, the technology underpinning CAVI continues to necessitate rigorous validation through ongoing clinical trials. Furthermore, its effectiveness must be evaluated against optimal medical therapy within the framework of randomized controlled trials to establish a robust base of evidence.
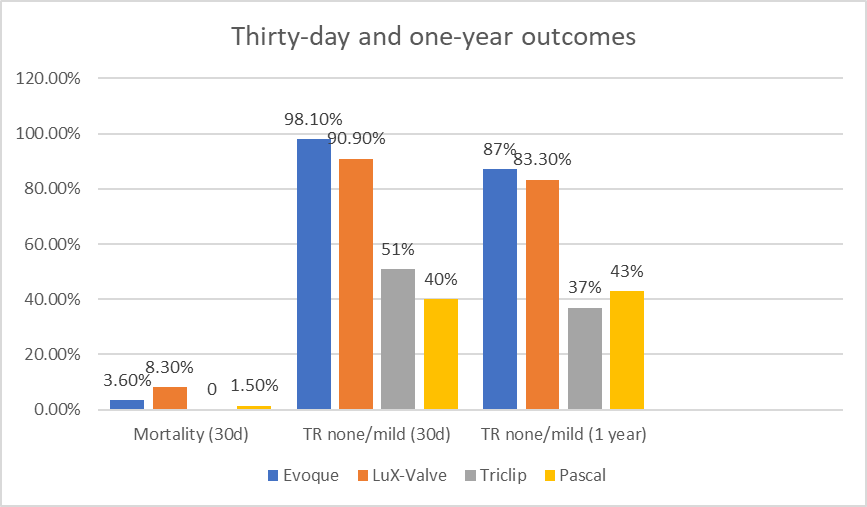
Figure 3: Thirty-day and one-year outcomes of transcatheter tricuspid valve intervention[9, 10, 37-41]
Valve durability and anticoagulation
Similar to transcatheter aortic or mitral valves, an inevitable issue with transcatheter tricuspid valves is their durability. Based on past experiences, the durability of bioprosthetic valves typically ranges from 10 to 15 years[49, 50]. However, the durability of right-sided cardiac transcatheter bioprosthetic valved stents remains unclear. The location of the tricuspid valve makes it more susceptible to the complex hemodynamic effects within the heart, particularly in the low-pressure regions. Although the pressure in this area is relatively low, factors such as regurgitation and turbulent flow contribute to increased risks of calcification and wear. Consequently, the durability of the tricuspid valve is generally lower compared to other heart valves. Tissue-engineered bioabsorbable heart valves may offer a strategic approach. Currently, tissue-engineered heart valves have achieved encouraging results in the pulmonary valve domain[51]. Nevertheless, further research is required in the tricuspid valve area.
Currently, there is a lack of evidence-based guidelines for antithrombotic therapy in patients undergoing transcatheter tricuspid valve interventions[52]. Drawing from the experience with surgical bioprosthetic valves, in the absence of an indication for long-term oral anticoagulation (OAC), it is considered reasonable to administer vitamin K antagonists for 6 months following TTVR[53]. Notably, due to the relatively lower blood flow in the right heart chambers, the risk of thrombosis in right-sided prosthetic valves is higher than in left-sided valves[54]. Therefore, an extended duration of OAC may be recommended. After TTVr, single antiplatelet therapy may be considered. However, since most patients already require anticoagulation due to pre-existing atrial fibrillation, they are typically maintained on long-term OAC[55]. Major bleeding is the most common serious complication following TTVI, highlighting the need for further research to determine the optimal duration of anticoagulation after transcatheter tricuspid valve intervention.
Right ventricular dysfunction
Although transcatheter TTVR can effectively eliminate TR, a subsequent complication is the decline in RV function. Right ventricular systolic dysfunction persists 30 days post-operation, which may indicate that the mechanical function of the RV had already been impaired under chronic severe TR but was masked by the reduced afterload[56]. Following TTVR, the significant reduction in TR leads to a sharp increase in afterload, thereby negatively affecting RV function.
Sugimoto et al[57]. proposed a novel load-independent method for measuring RV contractility and found that RV dysfunction in patients with severe TR at baseline did not change after tricuspid valve surgery. While postoperative RV function can predict the outcomes of tricuspid valve surgery, the results of transcatheter devices warrant further investigation. For instance, the single-leaflet design of the Trisol valve, with its high closing volume, can mitigate the sharp increase in afterload that follows the reduction of TR.
In conclusion, while TTVR shows promise in addressing TR, careful consideration of RV function and ongoing research into device-specific impacts on afterload are essential to optimize patient outcomes.
Transvenous leads and transcatheter tricuspid valve devices
The incidence of TR increases exponentially in patients with implanted cardiac electronic devices[58]. This increase is significantly attributed to the leads passing through the tricuspid valve, which can directly interfere with the normal movement of the leaflets, preventing them from closing completely[59]. Prolonged lead friction may also cause structural degeneration or damage to the tricuspid valve[60]. Additionally, long-term interactions can lead to an inflammatory response, resulting in local fibrosis or scar formation, which further impairs leaflet function[61].
Endocardial leads can become trapped between the valve stent and the endocardium, resulting in transvenous lead entrapment.
In the TRISCEND trial, all nine patients with pre-existing pacemakers had their right ventricular leads trapped by the Evoque valve[37]. If a trans-tricuspid lead becomes trapped, it cannot be fully removed in the event of device infection, necessitating alternative surgical extraction and prolonged antibiotic therapy, both of which carry significant mortality risks. In cases of device infection, prolonged suppressive antibiotic therapy has been associated with a 25% mortality rate at one month post-hospitalization and a 90% mortality rate at five years, with an estimated median survival of 1.43 years. Additionally, 18% of patients experience recurrence within one year[62]. The need for surgical extraction also poses serious morbidity risks, particularly in the population undergoing TTVR due to high surgical risk.
In appropriate patients, percutaneous transvenous lead extraction (TLE) may be considered prior to the TTVR procedure[63]. It is important to consider that in patients with TR, the lead may have been embedded or formed scar tissue due to prolonged presence. Removing the lead may further damage the tricuspid valve, leading to more severe regurgitation or acute valve dysfunction. In the ELECTRa registry, out of 3,555 patients who underwent TLE, 0.02-0.59% experienced worsening of tricuspid valve function post-TLE[64]. Polewczyk A et al. reported that in a study of 2,631 patients, 2.5?veloped severe dysfunction following TLE. Therefore, when the risk of TLE is relatively low, performing TLE before TTVR is worth considering[65].
For patients requiring ventricular pacing, leadless pacemakers are a good option[66]. However, it is advisable to implant the pacemaker before TTVR, as the delivery sheath size for devices such as Micra or Aveir is relatively large and may increase the difficulty of the procedure[67]. Utilizing a coronary sinus-based pacing system is also an option. Although studies suggest that placing transvenous leads on a bioprosthetic valve may be safe and not affect valve function, the lack of long-term follow-up necessitates caution with this approach[68]. Epicardial pacing leads do not involve the valve but come with increased invasiveness[69].
In summary, choosing a rhythm management method requires comprehensive consideration of the patient’s specific circumstances.
TR is no longer overlooked, as it significantly contributes to cardiac morbidity and mortality. With the rapid advancement of TTVR therapies, tricuspid regurgitation can now be effectively corrected, avoiding the adverse risks associated with traditional surgery.
TTVR devices offer clear advantages over surgical tricuspid valve replacement and transcatheter repair, reducing mortality and complication rates while effectively treating TR. Additionally, TTVR devices are less dependent on anatomical factors and the underlying TR etiology. Although some devices have received clinical approval, research on TTVR remains limited. Further studies with larger populations, longer follow-ups, and standardized management strategies are needed to advance this field.
Early feasibility studies show promising results and ongoing research continues to explore TTVR’s potential. For patients with severe TR who lack other treatment options, TTVR offers significant hope for the future.
Abbreviations
CAVI :Caval valve implantation
CE :Conformité Européene
ESC :European Society of Cardiology
EACTS :European Association for Cardio-Thoracic Surgery
FDA :Food and Drug Administration
MR :Mitral regurgitation
OAC :Oral anticoagulation
RA :Right atrium
RV :Right ventricle
TLE :Transvenous lead extraction
TR :Tricuspid regurgitation
TTVI :Transcatheter tricuspid valve intervention
TTVr :Transcatheter tricuspid valve repair
TTVR :Transcatheter tricuspid valve replacement
TV :Tricuspid valve
Conceptualization, X.Z. and G.L.; methodology, G.L.; data curation, D.M., S.L.S.; writing—original draft preparation, Z.X., G.L. and N.S.P; writing—review and editing, T.P., D.M., S.L.S., D.F., G.W., O.J.M., H.S., T.A. and R.B.; visualization, D.F. and H.S.; supervision, G.L.; project administration, G.L.; funding acquisition, G.L. All authors have read and agreed to the published version of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
