
case report | DOI: https://doi.org/10.31579/2690-4861/438
1Department of Cardiothoracic Vascular Surgery, The Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, China.
2The Affiliated Nanhua Hospital, Department of Gastroenterology, Hengyang, Hunan, China.
3Youjiang Medical University for Nationalities, Baise, China.
4Department of Cardiothoracic Vascular Surgery, The Affiliated Nanhua Hospital of University of South China.
*Corresponding Author: Yi Zhang, MD, PhD, Department of Cardiothoracic Vascular Surgery, The Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, China.
Citation: Fengqing Liao, Jialong Huang, BoHao Yang, Yang Hu, XiaFei Li, et al, (2024), Tracheal Reconstruction in a Patient with Tracheal Stenosis Following Acute Pancreatitis Supported by VV ECMO: a Case Report and Literature Review, International Journal of Clinical Case Reports and Reviews, 18(3); DOI:10.31579/2690-4861/438
Copyright: © 2024, Yi Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 April 2024 | Accepted: 25 June 2024 | Published: 08 July 2024
Keywords: tracheal stenosis; acute pancreatitis; ecmo; tracheotomy; airway management
This case report presents a case of tracheal obstruction following severe pancreatitis and describes the condition and airway management of an adult patient from the emergency department to the intensive care unit (ICU), from airway management to pre-operative ECMO implantation to intraoperative ECMO Weaning. Transselective venovenous extracorporeal membrane oxygenation (VV ECMO) effectively mitigates the risks associated with tracheotomy, thereby creating a safe setting for tracheal reconstruction surgery. This case report delves into the mechanisms, characteristics, diagnosis, and treatment of tracheal stenosis. Additionally, a potential association between tracheal stenosis and pancreatitis is explored. Tracheotomy supported by VV ECMO to ensure ventilation, emerges as a viable alternative.
AP is an acute inflammatory condition characterized by the self-digestion of pancreatic tissue, leading to a systemic inflammatory response.1-3 TS is an obstructive upper airway disease that can be life-threatening.4 Severe cases of TS are rare and typically present as respiratory dysfunction.5 Currently, the main cause of TS is believed to be the result of repeated injury and repair of the tracheal mucosa and abnormal wound healing such as granulation tissue proliferation.4,6 ECMO is mainly used to provide continuous extracorporeal respiratory and circulatory support to maintain life in patients with respiratory and/or cardiovascular failure, and is usually used in patients with severe acute respiratory distress syndrome (ARDS).7,8
In this article, we present a case study of a patient who developed severe tracheal stenosis two months after surgery for severe pancreatitis. The patient underwent a successful tracheal reconstruction with ECMO support. It is important to note that tracheal stenosis following pancreatitis is an extremely rare occurrence. Our focus was on exploring the relationship between tracheal stenosis and pancreatitis, discussing the selection of surgical methods, managing the patient’s airway, and highlighting the application of ECMO.
A 31-year-old male was admitted to our hospital's emergency department in May 2023 with dyspnea and confusion. The patient’s family complained of shortness of breath for 7 days after activities, which was significantly aggravated in the past 3 days, accompanied by a cough and difficulty in coughing up phlegm. Upon admission, physical examination revealed the presence of three obvious concave signs, profuse sweating throughout the body, and wheezing rales in both lungs. Additionally, a 10 cm surgical scar and peri-pancreatic drainage tube were observed in the left abdominal region. On arrival, his oxygen saturation in room air, was 90%, and his heart rate (HR) was 121 bpm. The initial blood pressure (BP) readings were 226/113 mmHg. Immediate management of the patient included high-flow non-invasive oxygen therapy and urapidil infusion, which resulted in immediate improvement in breathing, an increase in SpO2 to 100%, and a decrease in blood pressure to 182/99 mmHg.
The patient was admitted to our hospital at the end of January 2023 with acute pancreatitis, complicated by pulmonary infection and respiratory failure. Following pancreatic puncture drainage, anti-infection treatment, blood transfusions, and six days of tracheal intubation, the patient’s condition improved. However, the fever recurred later, and the condition gradually deteriorated. In early March, surgical intervention was performed to remove necrotic pancreatic tissue and drain the peri-pancreatic abscess. On the second postoperative day, the patient developed acute peritonitis, sepsis, and multiple organ failure. Laparoscopic exploration, removal of pancreatic necrotic tissue, abscess incision and drainage, and jejunostomy surgery are all performed in an emergency. After six days of mechanical ventilation via tracheal intubation, the patient was successfully weaned and showed gradual improvement. He was discharged in mid-April but still had a peripancreatic drainage tube in place. The patient was in good health prior to admission.
Immediate chest CT and three-dimensional reconstruction of the trachea revealed significant tracheal stenosis (below the cricoid cartilage), with no apparent abnormalities in the rest of the trachea(Figure2 a). Abdominal CT showed resolution of exudative lesions in the abdominal cavity, decreased ascites, and improvement in mesenteric edema. The patient was transferred to the ICU because of confusion consciousness gradually improved, and oxygen saturation increased following sputum aspiration, high-flow noninvasive mechanical ventilation, and oxygen therapy.
A multidisciplinary team comprising critical care physicians, respiratory physicians, cardiothoracic surgeons, anesthesia teams, and ENT surgeons, consulted at the bedside in the ICU, with special focus on airway management. Given the patient’s short neck, severe stenosis below the cricoid cartilage, and the potential inability of our smallest tracheal tube to pass through the narrowed lumen, our primary concern was the risk of rapid respiratory failure in the event of failed intubation leading to airway bleeding. Tracheotomy, although initially considered, was deemed excessively risky because of its high potential for bleeding and asphyxia. Bronchoscopic balloon dilatation was also considered but was deemed highly likely to fail because of the severity of the stenosis, potentially causing treatment delays. Therefore we needed a new method to ensure adequate ventilation. Hence, we reached out internal ECMO team and proposed an individualized approach after extensive deliberation. This approach involved a predetermined VV ECMO cycle under local anesthesia, followed by transfer to the operating room for the induction of general anesthesia with ECMO support. The patient then underwent the classical procedure of tracheal resection and end-to-end anastomosis, and specimens were collected for pathological evaluation. After the procedure, the patient received further treatment in the ICU. The patient’s family provided informed consent for the proposed plan, acknowledging its associated risks and benefits.
After administering sedation, the patient was positioned supine with the head tilted to the left side and the right lower limb abducted and externally rotated. The right internal jugular vein and right femoral vein were used as catheters. Following local anesthesia with 2% lidocaine, ECMO catheters were placed under ultrasound guidance and heparin saline was injected. The flow rate was gradually adjusted from 0.5 L/min. When the flow rate reached 3.45 L/min, ECMO functioned effectively, achieving a blood oxygen saturation of 100%, and the catheter was secured in place.
An unexpected occurred upon admission to the operating room. Blood oxygen saturation decreased from 100 percent to 78 percent, while vital signs remained stable. Suspecting inadequate blood volume or recirculation as potential causes, 2.0 u of suspended red blood cells without white blood cells and 1,000 ml of sodium lactate Ringer solution were given to replenish the blood volume. Additionally, we adjusted the blood flow rate to 3.6 L/min, resulting in a gradual increase in the blood oxygen saturation to 96 percent. With the patient’s blood oxygen restored, the procedure commenced with the patient in the supine position. Tracheotomy was performed under local anesthesia, followed by intubation and mechanical ventilation to maintain a blood oxygen saturation above 95 percent. Minor intraoperative bleeding was also observed. The patient was weaned from ECMO as soon as possible to prevent ECMO-related complications and alleviate the financial burden on the patient’s family. The ECMO blood flow rate was reduced to 1.5 L/min, then turned off completely, while the patient’s oxygen saturation remained stable at 98 percent. After a total operative time of 1.5 hours, successful weaning from ECMO was achieved. Following satisfactory general anesthesia, a vertical incision of approximately 6 cm in length was made in the neck, up to the thyroid cartilage down to the suprasternal fossa, and the trachea was incised upwards along the endotracheal tube. The thickened tracheal wall was approximately 2 cm in long. The stenotic trachea was resected and the posterior and lateral walls of the trachea were anastomosed with a 3-0PDS suture. Adequate hemostasis was achieved and the incision was thoroughly irrigated before layer-by-layer closure. The lower jaw was fixed with a No.10 suture and the neck was positioned in a forward flexed position. Intraoperative bleeding was minimal and blood oxygen saturation remained above 95 percent throughout the procedure.
Following the surgical procedure, the patient was admitted to the ICU for ongoing treatment while still intubated. The following day, the patient regained full consciousness and was able to breathe spontaneously without any shortness of breath, asthma, or surgical complications(Figure2 b). Subsequent examination using an electronic bronchoscope revealed that the patient’s airway was unobstructed, and no significant narrowing was observed. Following extubation, the patient did not experience any discomfort such as difficulty in breathing.
When the patient's condition stabilized, he was transferred to the general respiratory ward for further treatment and evaluation of his pancreatic disease. Currently, the patient’s pancreatic abscess has been completely drained, and a re-examination has shown significant improvement. The peripancreatic drainage tube was removed based on the recommendations of hepatobiliary surgeons. Subsequent treatment proceeded smoothly. Histopathological examination of the resected specimen showed chronic mucosal inflammation with squamous metaplasia, obvious fibrous connective tissue hyperplasia, and several trabecular bone formations on the lateral side of the cricoid cartilage, however no tumors were found(Figure1).
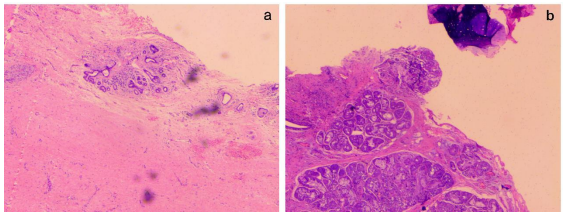
Figure 1. Pathological examination showed chronic mucosal inflammation with squamous metaplasia, obvious fibrous connective tissue hyperplasia, and several trabecular bone formations on the lateral side of the cricoid cartilage, but no tumor was found.
During a follow-up examination conducted 5 months after the surgery, no new narrowing of the airway was detected, and there was a significant improvement in tracheal stenosis compared to the preoperative condition (Figure2 c).
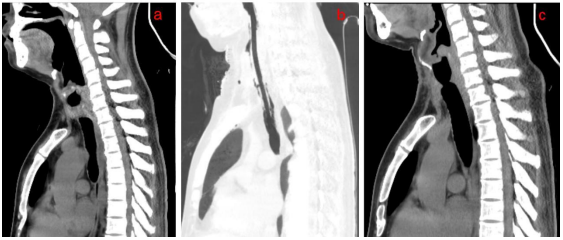
Figure 2. (a)A CT examination on admission revealed significant narrowing of the trachea (below cricoid cartilage level). (b)A post-operative CT examination revealed that the trachea was intubated, the extent of tracheal stenosis was reduced compared to before, and there was new edema and drainage tube shadowing in the soft tissue of the anterior neck. (c)A CT examination 5 months after surgery showed that the trachea (level below the cricoid cartilage) was slightly narrow, which was significantly better than before surgery, and the edema of the anterior cervical soft tissue subsided
Discussion
This case report describes a patient who developed severe tracheal stenosis two months after undergoing tracheal intubation, mechanical ventilation, and surgical treatment for severe acute pancreatitis. The occurrence of severe tracheal stenosis during the subsequent treatment of acute pancreatitis raises questions about the potential connection between the two conditions. AP is an acute inflammatory process characterized by the self-digestion of pancreatic tissue.1-3 The primary systemic complications include systemic inflammatory response syndrome (SIRS), sepsis, multiple organ dysfunction syndrome (MODS), intra-abdominal hypertension (IAH), and abdominal compartment syndrome (ACS). Local complications were mainly related to fluid accumulation in the pancreas peri-pancreas and tissue necrosis. Other complications include gastrointestinal bleeding, abdominal bleeding, biliary obstruction, intestinal obstruction, and intestinal fistula, etc.1,3,9 TS is an obstructive upper airway disease that typically results from repeated damage and repair of the tracheal mucosa and proliferation of granulation tissue.4,6 Various causes can lead to TS, including tracheotomy, tracheal intubation, tracheal trauma or surgery, inhalation injury, infectious causes, and immune-related factors (such as granulomatosis with polyangiitis, systemic lupus erythematosus, relapsing polychondritis, sarcoidosis, and IgG4-related disease). Prolonged mechanical ventilation with endotracheal intubation is the most common cause of TS.4,6,10,11 Major risk factors include diabetes mellitus, prolonged intubation, the use of large types of catheters, recurrent respiratory tract infections, advanced age, gastroesophageal reflux, steroid treatment, etc.11-13 The patient reported in this case had complications involving multiple systems of the body, including the respiratory system. Although he had undergone tracheal intubation, the development of such severe stenosis following intubation was extremely rare. We considered the possibility that pancreatitis could contribute to or worsen the tracheal stenosis. In a literature review, we came across a case report by Yasuo describing a patient with tracheal stenosis due to autoimmune pancreatitis. Bronchial biopsy revealed diffuse infiltration of plasma cells, lymphocytes, and fibrotic eosinophils. Immunostaining revealed infiltration of several IgG4-positive plasma cells, ruling out the possibility of coexisting sarcoidosis and the significant impact of steroid therapy.14 This finding suggests a possible direct relationship between autoimmune pancreatitis and tracheal stenosis. The repair process of tracheal injury is a highly coordinated wound healing process, and comorbidity and critical illness can disrupt its balance and lead to abnormal scar formation. Currently, there is no evidence of direct relationship between acute pancreatitis and tracheal stenosis. However, the systemic inflammatory response triggered by pancreatitis, along with the resulting multi-organ damage including the respiratory system, and the increased blood glucose levels due to impaired islet function, may indirectly contribute to the occurrence and worsening of tracheal stenosis. This case suggests a potential connection between pancreatitis and tracheal stenosis that warrants further confirmation.
The primary symptoms of TS include varying degrees of dyspnea and shortness of breath, accompanied by cough, wheezing, and increased respiratory secretions, which are exacerbated by physical activity.5,15 The patient was admitted to the hospital because of shortness of breath, and a CT examination revealed severe tracheal stenosis. The treatment for TS varies depending on the etiology, location, and severity of the stenosis, with surgery being the main approach. Surgical techniques included airway stenting, balloon dilatation, and tracheal resection. Endoscopic balloon dilation is the main treatment method known for its simplicity, effectiveness, and short procedure duration.16 However, it is typically used in patients with mild stenosis (stage 1 or 2), in early immature lesions or soon after an airway reconstruction procedure to prevent restenosis.17,18 In this particular case, considering the patient’s severe tracheal stenosis, endoscopic balloon dilation was not suitable. Tracheal resection and end-to-end anastomosis (TRE) are the standard treatments for tracheal stenosis, known for their lower restenosis rates compared to endoscopic treatment.17-20 After evaluation, we concluded that TRE was the most appropriate surgical approach.
Hypoxemia and asphyxia are the primary causes of mortality in these patients.15 The key to treatment is ensuring adequate oxygenation, ventilation, and emergency surgical intervention.15,21 Surgical resection of tracheal stenosis cannot be safely performed without adequate ventilation. Conventional airway management techniques, such as nasal oxygenation, mask ventilation, supraglottic airway devices, laryngeal masks, endotracheal intubation, and tracheotomy, are typically suitable for patients with mild airway obstruction.15,22 However, due to the patient’s near-complete tracheal stenosis below the cricoid cartilage, tracheal intubation and tracheotomy carry a significant risk of hemorrhage and asphyxia. Anesthesia induction could result in complete occlusion of the airway, and the application of the appeal method may not guarantee adequate ventilation. In such cases, extracorporeal ECMO may be a suitable option.
ECMO is mainly used to provide continuous extracorporeal respiratory and circulatory support to maintain life in patients with respiratory and/or cardiovascular failure, commonly seen in severe ARDS.7,8 The two main ECMO modes are veno-arterial (VA) ECMO and veno-venous (VV) ECMO. In VA ECMO, venous blood is withdrawn, oxygenated, and returned to the arterial system to provide circulatory and respiratory support, which is a heart-lung replacement mode.8,21,22 Compared to the VA mode, VV ECMO solely offers extracorporeal respiratory support, avoiding the risk of arterial injury and causing fewer hemodynamic disturbances.21,23 The choice of ECMO mainly depends on the urgency and necessity of circulatory support.23 In this case, considering the patient’s intact circulatory function, we opted for VV ECMO. Following the initiation of ECMO, the patient’s oxygen saturation was 100%. However, it dropped upon arrival at the operating room. We suspected recirculation or insufficient blood volume as possible causes, and observed that the oxygen saturation returned to normal after blood transfusion, fluid resuscitation, and flow adjustment. We performed tracheotomy with ECMO support, which resulted in the stabilization of blood oxygen levels following intubation. Considering the potential complications associated with long-term ECMO use (and long-term intubation), such as renal failure requiring continuous hemofiltration, bacterial pneumonia, bleeding, sepsis, hemolysis, liver dysfunction, leg ischemia, and venous thrombosis, we aimed to wean the patient off ECMO as soon as feasible.21 The incidence of complications with ECMO for short periods is relatively low, and early weaning can reduce the likelihood of complications and minimize hospitalization costs.21 The utilization of ECMO in the treatment of tracheal stenosis offers notable advantages. First, it can be employed in cases of severe tracheal stenosis where oxygenation through the trachea is not possible, providing valuable time for strategy formulation and implementing appropriate treatment measures.7,24 Second, it allows for satisfactory oxygenation during tracheotomy, circumventing the risk of bleeding and asphyxia. When conventional ventilation methods are difficult to complete or there are serious risks of uncontrollability, tracheotomy supported by ECMO may represent a reasonable and effective approach.
In summary, we present a case of severe tracheal stenosis following pancreatitis in which acute pancreatitis may indirectly lead to the occurrence and exacerbation of tracheal stenosis. In complex ventilation scenarios, ECMO can guarantee adequate oxygenation, allowing time for appropriate treatment. During the surgery, we performed tracheotomy with ECMO support to ensure proper ventilation. It has been shown that this may be a reasonable approach. In the development of cardiothoracic surgery, surgical risks have been controlled through multidisciplinary collaboration and technological advances, enabling increasingly sophisticated cardiothoracic surgery to be performed safely.25 This case report serves as an example of this evolving trend, which will continue in the future.
We express our gratitude to the patient who kindly provided consent for this case to be presented in this report.
Abbreviation: AP,Acute pancreatitis; TS, Tracheal stenosis; ICU, intensive care unit; ECMO, Extracorporeal membrane oxygenation; VV ECMO, venovenous extracorporeal membrane oxygenation; ARDS, acute respiratory distress syndrome; HR, heart rate; BP, blood pressure; SIRS, systemic inflammatory response syndrome; MODS, multiple organ dysfunction syndrome; IAH, intra-abdominal hypertension; ACS, abdominal compartment syndrome; TRE, Tracheal resection and end-to-end anastomosis ; VA, veno-arterial
Conceptualization:BoHao Yang.
Supervision: Jialong Huang, Yang Hu, Zhichao Ni.
Validation: Fengqing Liao, XiaFei Li, Xi Xia.
Visualization: Yi Zhang.
Writing – original draft: BoHao Yang, Yi Zhang.
Writing – review & editing: Jialong Huang, Fengqing Liao.
Funding Statement:The article didn't receive any forms of financial support.
The Author(s) declare(s) that there is no conflict of interest.
Supporting data can be requested by emailing the corresponding author for reasonable claims.
Ethics approval and consent to participate
Verbal informed consent was obtained from the patient's family for participation.
Verbal informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
