Video Presentation | DOI: https://doi.org/10.31579/2641-0419/240
1 Cardiothoracic Centre, All India Institute of Medical Sciences, New Delhi.
2 Department of Cardiothoracic and Vascular Surgery, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh
*Corresponding Author: Ujjwal Kumar Chowdhury, M.Ch, Diplomate NB Professor Department of Cardiothoracic and Vascular Surgery All India Institute of Medical Sciences New Delhi-110029, INDIA.
Citation: Ujjwal K. Chowdhury, Niwin George, Lakshmi Kumari Sankhyan, Shikha Goja, Arindam Choudhury., et all (2022). Total Pericardiectomy for Calcific Constrictive Pericarditis with Extracardiac Intrapericardial Caseating Mass via Median Sternotomy (Holman and Willett’s Approach): A Video Presentation. J. Clinical Cardiology and Cardiovascular Interventions, 5(2); DOI:10.31579/2641-0419/240
Copyright: © 2022 Ujjwal Kumar Chowdhury, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 December 2021 | Accepted: 31 December 2021 | Published: 07 January 2022
Keywords: myopericarditis; crohn’s disease; extra-intestinal
Pericardiectomy is the only accepted curative treatment for chronic constrictive pericarditis and its efficacy in improving symptoms with normalization of hemodynamic in the majority of cases has been established.
Pericardiectomy is the only accepted curative treatment for chronic constrictive pericarditis and its efficacy in improving symptoms with normalization of hemodynamic in the majority of cases has been established. [1-5]
Despite the experience spanning over 100 years, there is no fool-proof formula in the published literature to decide the optimal approach for a given patient. The literature is rife with descriptions of pericardiectomy by either left anterolateral thoracotomy or median sternotomy. Despite the effectiveness of surgery, there are disparate opinions regarding the role of corticosteroids in treating tuberculous pericarditis, timing of operation, surgical approach, and extent of decortication and requirement of Cardiopulmonary Bypass (CPB). [6-10] The efficacy of pericardiocentesis in preventing CCP in pericardial effusion (serous/or haemorrhagic) has been inadequately investigated. [10] The terms “radical”, “total”, “extensive”, “complete”, “subtotal”, “adequate”, “near-total” and partial pericardiectomy have been variably used to describe the procedure, often without precise definition of the limits of pericardial resection. [6-10]
Published reports attest to the unpredictable and variable pattern of CCP and lend support to radical decortication. In 2006, for the sake of uniformity, total pericardiectomy was defined as wide excision of the pericardium with the phrenic nerves defining the posterior extent, the great vessels including the intrapericardial portion of superior vena cava and superior vena cava right atrial junction defining the superior extent, and the diaphragmatic surface, including the inferior vena cava right atrial junction defining the inferior extent of the pericardial resection. [2] Constricting layers of the epicardium were removed whenever possible and the atria and venae cavae were decorticated in all cases in this study group. Pericardiectomy was considered partial if both ventricles could not be decorticated completely because of dense my pericardial adhesions or calcification. [2] Radical pericardiectomy was defined as removal of the entire pericardium over the anterolateral, diaphragmatic surfaces of left ventricle, portion of pericardium posterior to the phrenic nerve and the left ventricle and the anterior and diaphragmatic surfaces of right ventricle until the atrioventricular groove leaving behind intact left and right phrenic pedicles. [2]
Secondly, the importance of unrecognized constricting epicardial (visceral pericardial) peel was described by Harrington in 1944 and successful pericardiectomy requires decortication of the ventricular epicardium and relief of all constricting layers. [7] In a study, the normalization of pressure volume loop was used as an indicator of operative success of pericardiectomy.[12]
In 2006, we compared two surgical approaches for the treatment of chronic constrictive pericarditis i.e., median sternotomy and conventional left anterolateral thoracotomy in 395 patients. The surgical approach was primarily based on surgeon’s preference and remained uniform.2 However, the median sternotomy approach was preferred in the following conditions: (1) annular CCP, (2) extracardiac intrapericardial mass, (3) presence of a gradient between the superior or inferior venae cavae and right atrium of 2 mmHg or greater, (4) calcific pericardial patch compressing the RA and right ventricular outflow tract, (5) previous open heart surgery, (6) circumferential ‘cocoon’ calcification of the pericardium, and (7) recurrent chronic constrictive pericarditis after partial pericardiectomy.2 We demonstrated that the maximum benefit occurs after total pericardiectomy which is best achieved through a median sternotomy and is very difficult through a conventional left anterolateral thoracotomy.[2]
However, a left anterolateral thoracotomy was the preferred approach in cases of purulent pericarditis and effusive constrictive pericarditis is because of the presence of concomitant pyothorax and the concerns of sternal infection.[2]
Despite total pericardiectomy, the operative mortality rate was 7.6% in our series and 6% to 19% in several large series published after 1985. [9,10,13-15] Careful analysis of the published literature reveals the incidence of low cardiac output syndrome to be between 28% to 69% following total pericardiectomy. [9,10,13-15]
In an effort to further decrease the hospital mortality and postoperative low cardiac output syndrome, the author performed several technical modifications of the left anterolateral thoracotomy approach to achieve further radical excision of the pericardium extending posterior to the phrenic nerve and diaphragmatic pericardium without utilizing cardiopulmonary bypass.[16] In 2008, we published our preliminary experience with this technique of radical pericardiectomy via modified left anterolateral thoracotomy without utilizing cardiopulmonary bypass and detailed the surgical steps with operative outcomes.[17]
In 2021, we addressed the long-term outcomes of a series of 127 consecutive patients aged 29.4±16.1 years (range 4-72 years) who underwent total pericardiectomy via modified left anterolateral thoracotomy without utilizing cardiopulmonary bypass. We demonstrated that using several technical modifications, it is possible to perform radical pericardiectomy via modified anterolateral thoracotomy particularly removing the constricting pericardium over the anterolateral, diaphragmatic surfaces of left ventricle including the portion posterior to left phrenic nerve and anterior diaphragmatic surfaces of the right ventricle until the atrioventricular groove. Our approach is associated with early normalization of hemodynamic, further reduction of operative mortality, low cardiac output syndrome and excellent long-term results without requiring reoperation. Routine use of cardiopulmonary bypass during pericardiectomy is not necessary in the majority of patients undergoing pericardiectomy.[18]
In 2021, on recommendation from STS, USA, the definition of radical pericardiectomy was revised. Radical pericardiectomy is more defined in terms of relation to oncologic situations where draining lymphatics/lymph nodes are removed as well. However, radical pericardiectomy is something that is never possible because it requires removal of all 3 layers of pericardium, which are fibrous and serous with 2 components: parietal and visceral epicardium; this is not possible in real life.[18]
We report herein the surgical technique on a 26-years-old male patient diagnosed with chronic calcific constrictive pericarditis with large extracardiac intrapericardial caseating mass in New York Heart Association class IV with massive ascites who underwent total pericardiectomy via median sternotomy without using cardiopulmonary bypass.
Patient was placed in supine position and an indwelling peritoneal dialysis catheter was inserted before surgery for gradual drainage of massive ascetic fluid.
Following median sternotomy, the thymus was subtotally excised to expose the pericardium overlying the aorta, and pulmonary artery, taking care not to injure the distended left brachiocephalic vein and the phrenic nerves on both sides.
Subsequently the pleural reflections on both sides were mobilized laterally to obtain a wide width of the pericardium. Both pleural cavities were widely opened to visualize both phrenic nerves and to decompress the pleural effusion. The pericardium was inspected and palpated to determine a soft noncalcified area. It is important to excise the large amount of fat which usually overlies the apex in proximity to the left phrenic nerve.
Cautery was set between 8 and 10 mv during the process of dissection to avoid cautery induced ventricular fibrillation.
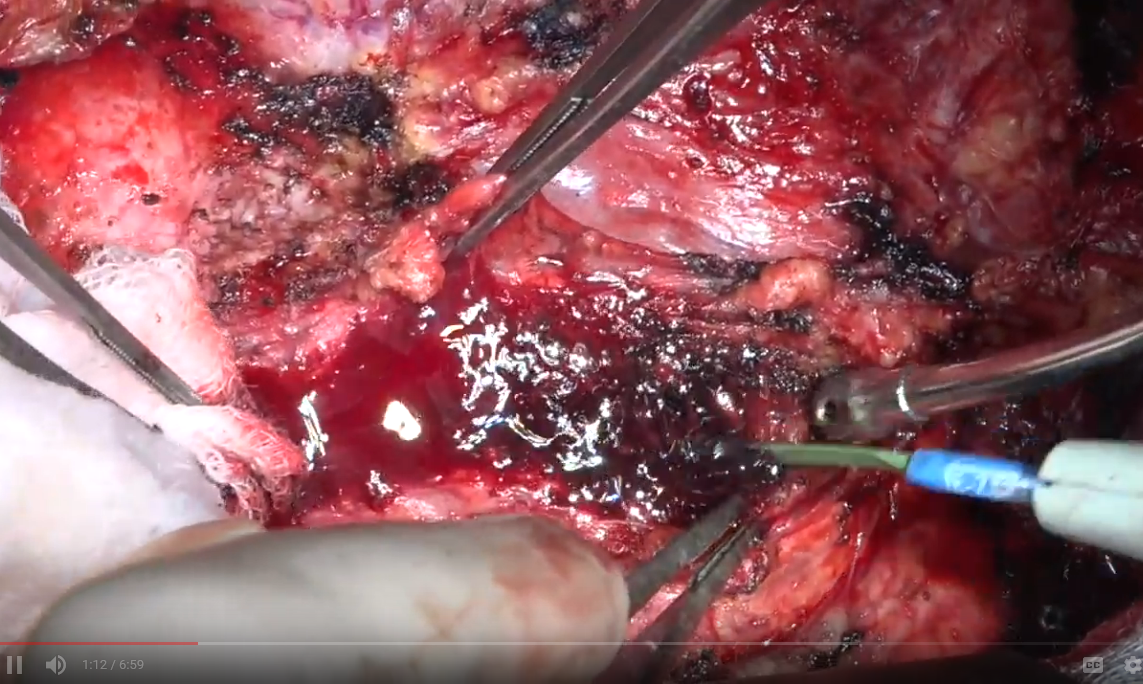
An I-shaped incision was made in the midline over the pericardium to the level of the pulmonary artery superiorly and diaphragm inferiorly. The pericardium was grossly thickened (>1.5 cm) and calcified at places. The mobilization of the pericardium was started at the lower end of the “I” incision on the left side and proceeded upward towards aorta to the lower border of the brachiocephalic vein.
The visceral pericardium was carefully incised until there was clear visualization of the epicardial fat and the coronary vessels. Extreme precautions were taken not to injure the epicardial veins and injury to the cardiac chambers and great vessels.
Multiple silk stay sutures were placed on the edges of the incised pericardium. The pericardium was initially divided at the bottom portion of the diaphragmatic reflection over the right ventricle and lateral pericardial flap was raised superiorly and laterally.
The pericardial flap was divided laterally over the right ventricle at the mid-portion to facilitate mobilization with minimal compression / manipulation of the cardiac chambers / great vessels, thereby maintaining stable hemodynamic. The posterior extent of dissection was approximately 1cm anterior to the left phrenic nerve.
Subsequently, a plane was developed between the diaphragm and the diaphragmatic pericardium. Three to four silk stay sutures were placed on the edges of the diaphragmatic pericardium dividing into two halves.
Dissection was done between the pericardium and the posterolateral left ventricular wall and along the inferior walls of the left and right ventricles. Posterolaterally, the pericardium posterior to the left phrenic nerve down to the left-sided pulmonary veins was dissected and excised, thus freeing the left ventricular apex.
Next the dissection proceeded laterally on the right side in a similar fashion as was done on the left side. The right pericardial flap was divided in the mid-portion and carefully dissected avoiding injury to the underlying right atrium, superior and inferior cavoatrial junctions. The posterior extent of the dissection line was approximately 1cm anterior to the right phrenic nerve.
The diaphragmatic pericardium on the right side was dissected off the diaphragm avoiding injury to the dilated and thinned inferior caval vein. The pericardial and pleural cavities were irrigated with normal saline. Two ventricular pacing wires were electively placed.
Postoperative recovery was uneventful. He was extubated 6 hours after surgery. He required dopamine 7.5µg/kg/min, dobutamine 10µg/kg/min and nitroglycerine 0.5µg/kg/min for a period of 96 hours. The right atrial pressure decreased from 30mmHg (preoperative) to 4-5mmHg in the immediate postoperative period. At 36 months of follow-up he was in New York Heart Association class I in normal sinus rhythm without any ascites.
Total pericardiectomy is associated with lower perioperative and late mortality, and confers significant long-term advantage by providing superior hemodynamic.
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of the article.
The authors received no financial support for the research, authorship and/or publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,