
Research Article | DOI: https://doi.org/10.31579/2642-9756/128
1 Obstetrics and Gynaecology Department, Faculty of Medicine, Ain Shams University
*Corresponding Author: Fady Makram Zaki Bakhiet. Department of Internal Medicine Grande International Hospital
Citation: Sherif Hanafi Hussain, Amro SalahEldin Elhoussieny, Fady Makram Zaki Bakhiet, Tarek Hesham Elsayed. (2021). Total Laparoscopic Hysterectomy Versus Total Abdominal Hysterectomy Due to Benign Genital Lesions in Obese Patients: Randomized Clinical Trial. J. Women Health Care and Issues. 4(8); DOI:10.31579/2642-9756/128
Copyright: © 2021, Fady Makram Zaki Bakhiet, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 March 2021 | Accepted: 30 June 2021 | Published: 05 October 2021
Keywords: total laparoscopic hysterectomy; total abdominal hysterectomy; obesity; benign gynecological diseases
Background: Hysterectomies are considered as the most common non-obstetric operation which performed in the United States and Western countries, with 23.3% of women aged 18 years or older undergoing the procedure. Abnormal uterine bleeding (45 %), uterine prolapse (14.5 %), endometriosis (11 %), and malignancies of the genital tract (10%) are the most common reasons for hysterectomy. Obesity is the common risk factor for these diseases. Obesity prevalence has doubled since 1980 and has reached ‘epidemic’ levels across the world, challenging health care systems and economies in developed and developing countries. According to the WHO, with 1.3 billion overweight (25 < body mass index [BMI] < 30) people and 600 million obese (BMI > 30) people in the world, the obesity rate exceeds 10% for both genders. In general, open surgery in obese patients has a number of drawbacks and has a budgetary impact. Therefore, the obese patients should undergo laparoscopic hysterectomies which has less adverse impacts on health and economy.
Aim of the Work: The aim of this study is to compare between total laparoscopic hysterectomy (TLH) and total abdominal hysterectomy (TAH) for benign genital diseases in the obese patients as regard to safety in the following parameters i.e. operative blood loss, conversion to laparotomy/return to theatre, postoperative hospital stay, the operative time, need for blood transfusion, organs injuries (bladder/ureter/bowel), postoperative vault hematoma, postoperative febrile disease, surgical site infection and wound dehiscence, postoperative pain and quality of life concerning about urinary, rectal and sexual functions.
Patients and Methods: This study was conducted at Ain Shams University Maternity Hospital. It included 20 obese patients undergoing total laparoscopic hysterectomy (TLH) in group A and another 20 obese patients undergoing total abdominal hysterectomy (TAH) in group B. The study duration was from July 2019 to July 2020.
Results: In this study the obese patients with benign pathology in the genital tract were divided into two groups according to approach of hysterectomy: group A contained 20 TLAs and group B contained 20 TAHs. The comparison between both groups showed statistically insignificant difference (p>0.05) as regard to clinic-demographic characteristics e.g., age, body mass index, parity, medical history, surgical history and indication of hysterectomy. However, TLH had less operative blood loss than TAH (p< 0.001). As well, TLH was less painful than TAH as illustrated by subjective visual pain scale at 6h and 24h after surgery (p< 0.001) and subjective postoperative number of analgesic ampoules (p< 0.001). Although TLH had shorter postoperative hospital stay than TAH (p< 0.001), the operating surgeon consumed significantly more time during the procedure in TLH than TAH (p< 0.001). In contrast, there was no statistically significance difference between both groups regarding to need for blood transfusion, organs injuries (bladder/ureter/ bowel), conversion to laparotomy or re-operation, postoperative vault hematoma, postoperative febrile disease, wound complications (cellulitis/pus/dehiscence/hernia) and quality of life (p>0.05).
Conclusion: The study shows that total laparoscopic hysterectomy is a safe procedure for benign lesions of the genital tract in obese patients. It has physical, technical and economic advantages. Therefore, it can replace total abdominal hysterectomy with no considerable drawbacks.
The surgical removal of the uterus, known as a hysterectomy, can be done in a variety of methods. Vaginal hysterectomy is the oldest known method. Although there are medical documents of vaginal hysterectomy for prolapse dating back to 50 BC, the first planned hysterectomy was done by KonradLangenbeck, Surgeon General of the Hannovarian army. The first abdominal hysterectomy was performed in 1809 by Ephraim McDowell for a woman of five who had a huge ovarian lump on her kitchen table. Then, Harry Reich in Pennsylvania conducted the first laparoscopic hysterectomy in 1988 [1].
Today, minimally invasive hysterectomy (MIH) techniques offer less discomfort, a shorter hospital stay, faster recovery, and smaller scars. These procedures include laparoscopic supracervical hysterectomy (LSH), total laparoscopic hysterectomy (TLH), laparoscopically-assisted vaginal hysterectomy (LAVH). vaginal hysterectomy (VH) and Robotic-assisted hysterectomy (RAH) [2].
The surgical approach of hysterectomy is influenced by patient characteristics e.g. the reason for hysterectomy, uterine size, descent of the uterus, presence of diseased tissues surrounding the uterus, previous surgery in the pelvic region, obesity, history of pregnancy, the possibility of endometriosis, or the need for an oophorectomy [3].
When vaginal surgery is not possible, the laparoscopic surgery has several advantages; however, it takes longer time [3] to abdominal hysterectomy, total laparoscopic hysterectomy has a short inpatient treatment duration and a quicker return to normal activities; plus, it allows the possibility to diagnose and treat other pelvic diseases. However, it necessitates a high level of laparoscopic surgical expertise and there is an increased length of surgery [4] (King et al., 2016).
For obese persons, the laparoscopic technique is the preferable method [5] (Blikkendaal et al., 2015) particularly in light of the rising prevalence of obesity in recent decades; in Europe fluctuating between 6 and 37 % [6], and in the United States, the prevalence of BMI ≥35 kg/m2 remained relatively
The aim of this study is to compare between total laparoscopic hysterectomy (TLH) and total abdominal hysterectomy (TAH) for benign genital diseases in the obese patients as regard to safety in the following parameters i.e. operative blood loss,conversion to laparotomy/return to theatre, postoperative hospital stay, the operative time, need for blood transfusion, organs injuries (bladder/ureter/bowel), postoperative vault hematoma, postoperative febrile disease, surgical site infection and wound dehiscence, postoperative pain and quality of life concerning about urinary, rectal and sexual functions.
Patients And Methods
Inclusion and exclusion criteria: During the pre-selection phase (after admission into the Hospital) inclusion and exclusion criteria were applied.
Inclusion Criteria: All obese women (BMI equals or is greater than 30) with benign lesion of the genital tract (fibroid uterus, endometrial hyperplasia without atypia, non-dysfunctional uterine bleeding, uterine prolapse) and aged between 35 and 60 years
Exclusion Criteria: Gynecological malignancy, Chronic diseases (e.g. hypertension, diabetes mellitus), Bleeding tendency (e.g. coagulopathies, thrombocytopenia), any medical condition worsened by pneumoperitoneum or Trendelenburg position e.g. cardiac or pulmonary diseases.
All women included in the study were subjected to the following:
1. Verbal consent: had been obtained.
2. Careful and detailed history: for fulfillment of the inclusion and exclusion criteria including:
3. Examination of the women:
General examination:
more into the study
Abdominal examination:
Pelvic examination
Bimanual examination
4. Transvaginal ultrasound:
5. Cervical smear: All patients scheduled for hysterectomy had a cervical smear done at the Diagnostic Unit for Early Cancer Detection at Ain Shams University Maternity Hospital to exclude cervical microinvasion and atypical hyperplasia.
6. Counselling:
All patients were advised regarding the benefits and drawbacks of both procedures.
7. Blood preparation:2 units of whole blood were prepared for each patient undergoing hysterectomy either abdominal or laparoscopic.
8. Endometrial biobsy: to exclude atypia in endometrial hyperplasia
9. Routine preoperative laboratory investigations:
1.Intraoperative blood loss: through assessment of blood loss in TAH by measuring the suction volume and swab weight by the following equation: The amount of blood loss (ml) = [ (weight of the used towels and gauzes– weight of the towels and gauzes prior to the surgery) + the volume sucked in the suction bottle in ml ] provided that conversion of weight of towels and gauzes by (gm) to volume by (ml) by equation (1000 gm = 962 ml) [8] (Michael, 2004). The assessment of blood loss in TLH is by measuring the suction volume.
2.The operating time: which reflects difficulty of the procedure. It was calculated from the time of entry of primary trocar in case of TLH, and from the time of creating the skin incision in case of TAH until the last cutaneous closure sutures.
3.Intra-operative injuries: bowel, bladder or ureter injuries.
4.Need for blood transfusion.
5.Return to theater: need for laparotomy or re-operation
6. Postoperative vault hematoma: detected by postoperative 48-hours transvaginal ultrasonography
7.Postoperative febrile illness (postoperative fever): refers to an elevated body temperature (≥ 38.5°C) occurring after the surgical procedure during hospitalization.
8.Postoperativepain: assessed using a linear 10-cm visual analogue scale, ranging from 0 (no pain) to 10 (unbearable pain), at 6 and 24 hours after surgery. Besides, the type and number of postoperative analgesic ampoules should be mentioned.
9.Duration of hospital stay: The case of delayed discharge should be documented.
10. Wound complications: sepsis, cellulitis, dehiscence.
11. Quality of life: Abnormal rectal, urinary or sexual function at 3 months postoperatively
* EvaluationOf The Outcomes:
Intraoperative gravimetric assessment of measured blood loss
Data collection: The above-mentioned data were collected in a data sheet and the operative details were recorded. The women had been received the normal care of the post-operative management by the attending health professional. Statistical analysis was blinded to group allocation to avoid research bias.
Ethical considerations:
Ethics: The study had got approval from Ethics & Research Committee (ERC), Ob/Gyn department, Faculty of Medicine, Ain Shams University. The clinical research study conducted in accordance with the current approved clinical protocol and relevant policies, requirements and regulations of the Ain shams University Maternity Hospital.
Consent procedure: All of the patients were given the opportunity to give their informed consents. The investigator made an appropriate informed consent process in place to ensure that potential research subjects or their authorized representatives were fully informed about the nature and aim of the clinical study, the potential risks and benefits of study participation, and their rights during the study. The investigator obtained the written signed informed consent of each subject or their authorized representative before performing any specific procedures. The original signed form of informed consent was kept by the investigator.
Subject confidentiality: To maintain subject confidentiality, all evaluation forms, reports and other records did not includ unique personal data.
The collected data revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (SPSS 15.0.1 for windows; SPSS Inc, Chicago, 2001). Data was presented as mean and standard deviation (± SD) for quantitative parametric data, and median and interquartile range for quantitative non-parametric data. Frequency and percentage were used for presenting qualitative data. Suitable analysis was done according to the type of data obtained. Student T test or Mann Whitney test was used to analyze quantitative data while chi square test and fisher exact test was used to analyze qualitative data. The collected data revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (SPSS 15.0.1 for windows; SPSS Inc, Chicago, 2001). Data was presented as mean and standard deviation (± SD) for quantitative parametric data, and median and interquartile range for quantitative non-parametric data. Frequency and percentage were used for presenting qualitative data. Suitable analysis was done according to the type of data obtained. Student T test or Mann Whitney test was used to analyze quantitative data while chi square test and fisher exact test was used to analyze qualitative data.
The data of 40- obese- women study group who had hysterectomy with/without salpingoophorectomy due to benign lesions of the genital tract was statistically analyzed and compared regarding to demographic data, surgical and medical history, perioperative blood loss, the operating time, visceral injuries (bowel/bladder/ ureter), need for blood transfusion, need for laparotomy, vault hematoma, postoperative fever (temperature ≥ 38.5°C), postoperative pain, duration of hospital stay, wound complications (sepsis/cellulitis/dehiscence), and quality of life (rectal, urinary and sexual function).
Patient demographic characteristics in both groups showed no statistically significant difference as regard to age (means of TLH group 49.9 years &TAH group 50.6 years, p=0.698), parity (medians of TLH group 2.5 &TAH group 3.00, p=0.068) and body mass index (means of TLH group 33.13kg/m2&TAH group 32.92kg/m2, p=0.746).Plus, the medical and surgical histories were of no statistical significance (p>0.05).
As regard to the hysterectomy indication, the most common etiology for hysterectoctomy was fibroid which represented 15 cases (37.5%). Other causes included: postmenopausal bleeding 22.5% (9 cases), endometrial hyperplasia 12.5% (5 cases), ovarian cyst 12.5% (5 cases), adenomyosis 12.5% (5 cases) and postmenopausal endometrial polyp 2.5 % (1 case). Statistically, however, there was no significant variation among the etiologies distribution between TLH group and TAH group.
Regarding to perioperative blood Loss (ml) through both routes, the study showed that bleeding through abdominal route was markedly more than bleeding through laparoscopic route (the mean of TLH group 292.3 ± 24.75 ml / the mean of TAH group 394.2 ± 75.39) with P value (less then)0.001) indicating a high significant statistical difference.

Table 1: Comparison between Group A (TLH) and Group B (TAH) as regard to perioperative blood Loss (ml)
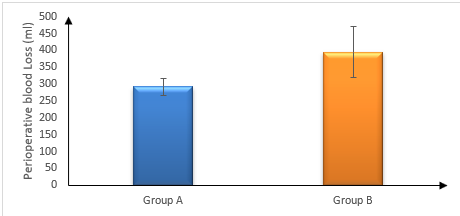
Figure 1: Comparison between Group A (TLH) and Group B (TAH) as regard to perioperative blood Loss (ml)
The operating time of the procedure starting from entry of primary trocar in case of TLH and incising the skin in case of TAH until the last cutaneous closure sutures was compared statistically between both groups. The abdominal route was much easier than the Laparoscopic procedure because the operating time of TLH (the mean 115.2 ± 10.01 min) was more prolonged than the operating time of TAH (the mean 87.85 ± 11.67 min). The P value (<0>
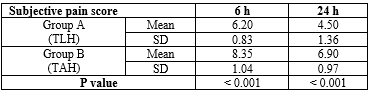
Table 3: Comparison between Group A (TLH) and Group B (TAH) as regard to subjective pain score
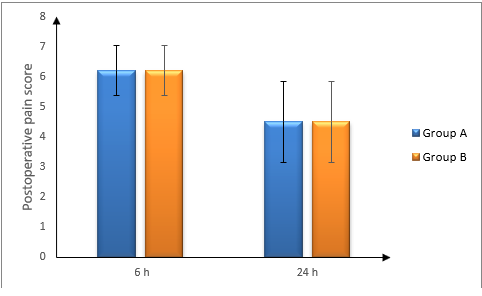
Figure 3: Comparison between Group A (TLH) and Group B (TAH) as regard to postoperative pain score at 6hr and 24 hr after surgery
Also, the study showed statistically significant difference between TLH and TAH as regard to number of analgesic ampoules. The number of analgesic ampoules required to modulate pain due to TLH (the mean 2.15 ± 0.12 ampoules) was significantly less than number of analgesic ampoules used to relieve pain due to TAH (the mean 3.25 ± 0.44 ampoules) with p value <0>
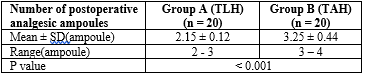
Table 4: Comparison between Group A (TLH) and Group B (TAH) as regard tonumber of postoperative analgesic ampoules
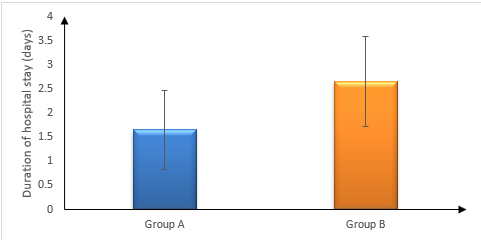
Figure 4: Comparison between Group A (TLH) and Group B (TAH) as regard to duration of hospital stay (days)
The study also statistically showed that patients doing TLH markedly stayed less days in hospital than patients doing TAH (the means 1.65 ± 0.81days, 2.65 ± 0.93 days respectively) with statistically highly significant difference (P value less than 0.001). As a result, the TLH was cost-effective in this prospective.
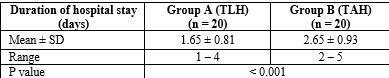
Table 5: Comparison between Group A (TLH) and Group B (TAH) as regard to the duration of hospital stay
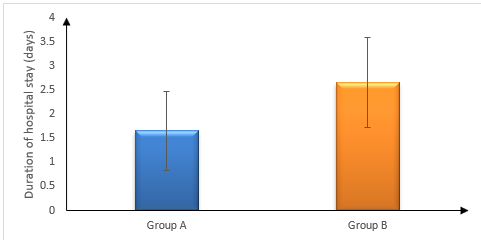
Figure 5: Comparison between Group A (TLH) and Group B (TAH) as regard to duration of hospital stay (days)
However, there was no significant difference between both groups as regard to need for blood transfusion, organs injuries (bladder/ureter/ bowel), conversion to laparotomy or re-operation, postoperative vault hematoma, postoperative febrile disease, wound complications (cellulitis/pus/dehiscence/hernia) and quality of life (p>0.05).
This study was an interventional comparative randomized clinical trial (RCT) conducted at Ain Shams University Maternity Hospital from July 2019 till July 2020. The study group included 40 obese women who attended the Outpatient Gynecological Clinic at Ain Shams University Maternity Hospital and for whom hysterectomy with/without salpingoophorectomy was indicated due to benign lesions of the genital tract. They were randomly divided into two equal groups. Group (A) contained 20 obese women undergoing total laparoscopic hysterectomy (TLA), whereas Group (B) contained 20 obese women undergoing total abdominal hysterectomy (TAH).
Patient demographic characteristics in both groups showed no statistically significant difference as regard to age and body mass index. Also, surgical, medical and obstetric histories showed no significant difference between both groups.
During the conduct of hysterectomy on either group, the both fallopian tubes were removed from all obese patients. However, bilateral oophorectomy was done only for diseased or atrophic ovaries. There was no significant difference between both groups (p value = 0.705).
In the context of our research which showed high significant difference between TLH and TAH in terms of operative blood loss, Colin had performed a meta-analysis of published randomised controlled trials to compare outcomes in total abdominal hysterectomy (TAH) and total laparoscopic hysterectomy (TLH) for benign disease. The results of this meta-analysis match this study results. In Colin's meta-analysis, pooled odds ratios (OR) were calculated for categorical variables using random effects models as per DerSimonian and Laird. Continuous variables were compared by means of weighted mean differences (WMD). TLH was associated with reduced estimated blood loss (WMD -183ml; 95% CI -346ml to -21ml; p=0.03)[9].
The same result was obtained in Sutasanasuang's retrospective comparative study containing 30 TLHs and 30 TAHs due to benign pathology ( the amount of blood loss for TAH 389.9 +/- 125.4 cc and for TAH 275.5 +/- 189.3 cc) [10] . As well, Schindlbeck retrospectively analyzed 43 total laparoscopic hysterectomies (TLH), 103 total abdominal hysterectomies (AH) and 87 vaginal hysterectomies (VH) due to bengin and malignant lesions of the genital tract as regard to perioperative blood loss. The results showed that TLH, in comparison to TAH, had significantly less bleeding [11]. The previous results of Schindlbeck's retrospective analysis match with the outcomes of this prospective clincal trial.
In contrast, BabElSharia University Hospital's prospective randomized controlled trial showed that there is no significant difference between TLH and TAH (the means of blood loss for TLH 184.8±24.6ml and TAH 208.75±21.8 ml with p value 0.711). However, the small sample size of this study targeted uterine tumours which were early-staged malignancy and/or less than 14 weeks (10 cm) [12]
As regard to the operating time, this study result matches with Colin's metanalysis which showed that it was longer operating time in the TLH group (WMD 22min; 95% CI 5-39 min; p=0.01) [9] (Walsh et al., 2009). Besides, Sutasanasuang's retrospective study showed the same result regarding to the operating time (218.4 +/- 79.3 min for TLH & 91.1 +/- 53.6 min for TAH) [10]
Regarding to postoperative pain reflected subjectively by visual pain scale and objectively by analgesic ampoules, the study result are the same of result of Sutasanasuang's retrospective comparative study containing thirty TLH patients and thirty TAH controls with benign uterine lesions, operated in Somdejprasangkharaj 17th Hospital in Suphanburi. The study showed that TLH is significantly less painful than TAH as illustrated in the means of dosage of meperidine (TLH mean 95.4 +/- 43.2 mg vs. TAH mean 2368 +/- 20.7 mg) and pain score (TLH mean 5.4 +/- 0.7 vs. TAH mean 8.7 +/- 1.3) [10]
In general, all studies of the literature considerably agree that duration of hospital stay after TLH is significantly shorter than hospitalisation interval after TAH. Therefore, the result study corresponds to the result of Pooja's study. It prospectively compared between 50 TLHs and 50 TAHs, and showed that the mean length of hospital stay was significantly lower (p< 0>
Also, this study result concerned with intra-operative complications agrees with Wang's meta-analysis of 9 randomized trials performed to investigate the effects of TLH versus TAH, however; it was done for women with early-stage endometrial cancer (RR = 0.98, 95%CI 0.62-1.55, P = 0.919) [14] well, in Masson's retrospective study, urological complications rate of TLH was no significantly higher than TAH [15]
A regard to blood transfusion, the study result does not correspond to Timmons's retrospective 517 charts review of patients who had undergone abdominal, laparoscopic, or vaginal hysterectomy due to benign lesions (blood transfusion for TAH 34/263 (12.92%) and TLH 5/119 (4.2%) with P value =.017). However, there were limitations to Timmons's study which included the retrospective observational character of the study, comparison among all routes of Hysterectomy, and unequality of the medical degrees of operating doctors [16]
It is worthy to mention the result of postoperative vault hematoma in this study corresponds to Shuk-Tak's retrospective analysis of 801 hysterectomized patients over a 3-year period in Pamela Youde Nethersole Eastern Hospital, Hong Kong. The study showed that there was no significant difference between TLH and TAH as regard to postoperative vault hematoma ((TAH 27/456 (5.9%) & TLH 7/122(5.7%) with odds ratio 1.033) [17]
In terms of return to theatre, the study result with Rebecca's retrospective study, carried out over a 5-year period with 296 procedures due to benign genital pathology, which mentioned that there was no significant difference between TLH and TAH as regard to the need for another laparotomy (TLH 3 cases (1.9%) & TAH 4 cases (3.1%) with p value 0.704) [18]
In terms of the requirement for additional laparotomy, the study found no significant difference between TLH and TAH (TLH 3 cases (1.9%) & TAH 4 instances (3.1%) with p value 0.704) [18]
Concerning to the wound complications spectrum, there was no significant difference between both groups. This result matches with the result of Anju who conducted a retrospective study at Indian general hospital to compare between 126 TLHs and 126 TAHs due to benign uterine diseases as regard to wound complications [19]
In addition, the quality of life (urinary, rectal and sexual function) did not change significantly between TLH group and TAH group when the patients had been questioned about the bladder and bowel functions and about sexual intercourse. This result corresponds to the result of a trial in Thailand, conducted by Shins and his colleagues, which compared between total laparoscopic hysterectomy (TLH) and total abdominal hysterectomy (TAH) for benign, pre-malignant and malignant lesions of uterus using Euro-quality of life five dimensions (EQ-5D) questionnaire to evaluate quality of life [20]
The study shows that total laparoscopic hysterectomyis a safe procedure for benign lesions of the genital tract in obese patients. It has physical, technical and economic advantages. It can replace total abdominal hysterectomy with no considerable drawbacks.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
