
Case Report | DOI: https://doi.org/10.31579/2690-1919/522
1Senior Health Officer, Department of Emergency Medicine, Pilgrim Hospital, United Lincolnshire Health NHS Trust (ULHT) United Kingdom.
2Trainee OBGYN year-4, Department of OBGYN, East Midlands deanery United Kingdom.
3Junior Clinical fellow, Department of Emergency Medicine Whittington Hospital United Kingdom.
4Consultant, Department of OBGYN Pilgrim Hospital, United Lincolnshire Health NHS Trust (ULHT) United Kingdom.
*Corresponding Author: Danyal Qureshi, Senior Health Officer, Department of Emergency medicine, Pilgrim Hospital, United Lincolnshire Health NHS Trust (ULHT) United Kingdom.
Citation: Danyal Qureshi, Aditi Kishore Shinde, Dawn Singh, and Ashok Mohanty, (2025), Torsion of Uterine Fibroid – A Diagnostic Dilemma, J Clinical Research and Reports, 19(4); DOI:10.31579/2690-1919/522
Copyright: © 2025, Danyal Qureshi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 March 2025 | Accepted: 16 April 2025 | Published: 28 April 2025
Keywords: COVID-19; immunization; menstrual pattern
A rare case of uterine fibroid torsion was managed successfully in a district general hospital in the United Kingdom. Uterine fibroids are benign tumours derived from uterine smooth muscle cells. The incidence of torsion in a uterine fibroid is less than 0.25%. This condition poses a diagnostic dilemma with potential life-threatening complications like necrosis, gangrene and peritonitis.
We report a 33-year-old lady who presented with acute onset abdominal pain. There was difficulty establishing a diagnosis and surgery was expedited on a high index of suspicion due to non-resolution of symptoms. Exploratory laparotomy with detorsion and myomectomy was done. In addition to relieving the patients’ symptoms, we managed to preserve fertility. A final diagnosis of uterine leiomyomata was confirmed on histopathology.
A low threshold for surgical intervention and timely expert opinion from radiologists is required in patients presenting with acute abdominal pain. The pathognomic feature of a torted uterine fibroid on imaging is called 'dark fan' sign. This is an area poor contrast enhancement in the uterus adjacent to the leiomyoma on CT scan.
Uterine fibroids or leiomyoma, are a benign tumour originating from the lining of the uterus [1] that consists of smooth muscle cell and connective tissue [2] that are hormone dependent [3]. They are the most common benign neoplasm affecting women [4], and can be classified based according to their anatomical location [5].
Leiomyomas have an estimated global incidence of 20-40% [6] and lifetime prevalence of 20- 30% [7]. They however have a greater incidence among certain ethnic groups, for example among Afro-Caribbean women who are 60% more likely to experience these neoplasms [8]. Younas et al. in their study of fibroid management describes that the incidence ratio of fibroids between Caucasian and Afro-Caribbean women is between 3 and 9:1 respectively [3]. Other epidemiological risk factors identified include age at menarche, advanced age, parity, vitamin D deficiency, diet, smoking, and hyper-estrogenic conditions such as polycystic ovarian syndrome, the oral contraceptive pill or hormone replacement therapy [9-12].
Furthermore, certain genetic and epigenetic characteristics make women more prone to uterine fibroids such as a positive family history, where there is a greater risk among sisters [13-17]. Similarly, a genome-wide association study (GWAS) reported a risk of uterine fibroid was 2.5-fold among first-degree relatives in contrast to the general population [18].
Among monozygotic twins, the concordance rate is double to that of dizygotic twins of the same sex, and greater than in first-degree relatives [18, 19]. Additionally, GWAS noted various candidate loci in chromosome regions among African American-22q13.1 (CYTH4); Caucasian-11p15.5 (BETIL), 17q25.3 (FASN, CCDC57 and SLC16A3), 22q13.1 (TNRC6B); and Asian-10q24.33 (OBFC1), 11p15.5 (BET1L), 22q13.1 (TNRC6B) populations [20-23].
This case review explores a rare presentation of leiomyoma torsion and describes a patient’s hospital journey, from diagnosis to management.
A 33-year-old Afro-Caribbean woman presented to the Accident and Emergency (A&E) department with a one-day history of sudden severe abdominal pain, radiating to her back. It was associated with nausea and lethargy. She denied fever, vomiting, vaginal bleeding or discharge. Surgical causes of acute abdomen were excluded, and due to the nature of her pain she was referred to the Gynaecological team for further assessment. Her past medical history is significant for migraines, latent tuberculosis and previous uterine fibroid. She has no past surgical history and had no prior pregnancies.
A computed tomography (CT) scan of the abdomen and pelvis revealed a large heterogeneously enhancing soft tissue attenuation lesion in the lower abdominal pelvic cavity in the midline, abutting the uterus, with the primary differential diagnosis being a large degenerating sub-serosal fibroid.
Magnetic Resonance Imaging (MRI) of the pelvis with contrast showed a well-circumscribed lower abdomen-pelvic mass measuring 10.04cm x 8.30cm x 11.60cm, located anterior- superior to the uterus, indenting the normal urinary bladder. There were at least two intramural fibroids involving the anterior myometrium (1.35 X 0.98cm and 1.23 X 1.0cm) and a single intramural fibroid involving the posterior myometrium (2.28 x 2.1cm). Bilateral ovaries otherwise appeared normal with minimal free fluid seen in the peritoneal cavity. No enlarged lymph nodes were seen in the pelvis. Figures 1-4 demonstrate these findings.
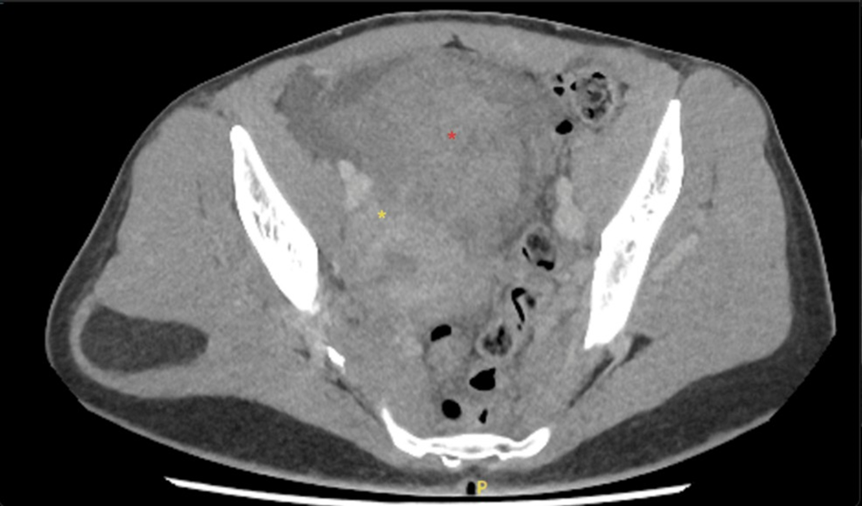
*Yellow: Uterus, *Red: Fibroid
Figure 1: Contrast Computed Tomography axial image of pedunculated fibroid.

*Yellow: Uterus, *Red: Fibroid, *White: Dark fan sign
Figure 2: Contrast Computed Tomography Sagittal images of pedunculated fibroid showing dark fan sign (indicated by*).
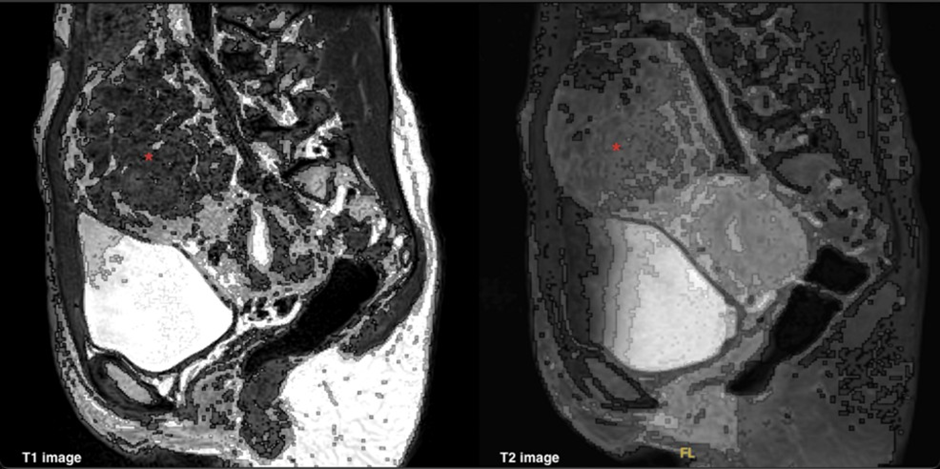
*Red: Torted fibroid
Figure 3: T1 and T2 saggital MRI images for pedunculated uterine fibroid with torsion (indicated by*).
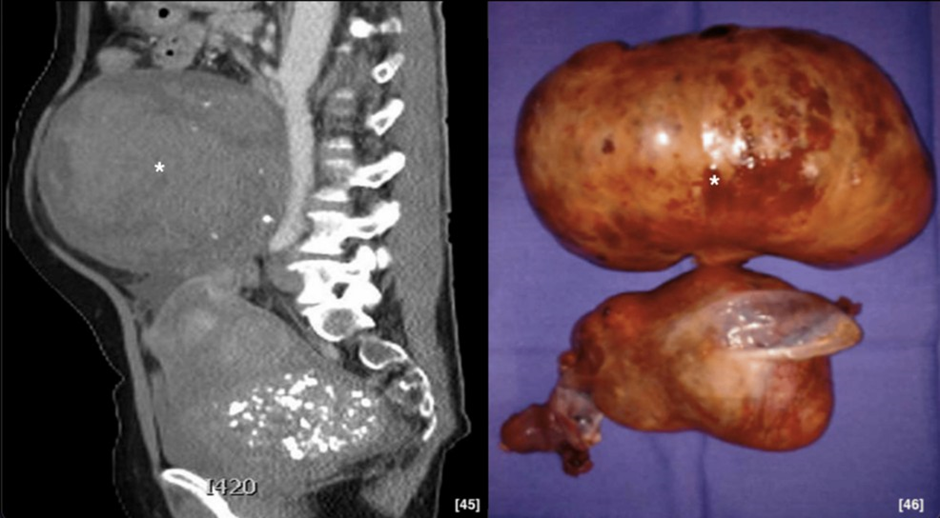
*White: Torted fibroid
Figure 4: Examples of uterine fibroid torsion. Re-printed with permission.
A diagnosis of torsion of pedunculated uterine fibroid was made and emergency laparotomy with myomectomy was performed. Intra-operatively, a 10cm sub-serosal fibroid was found attached on the uterine fundus with a short thick pedicle that was twisted once. The pedicle was clamped, and myomectomy done with continuous closure using vicryl in two layers.
Microscopic examination showed haemorrhagic leiomyoma with necrosis and leucocytic infiltrate. Post-operatively, the patient was managed with analgesia, laxatives, venous thromboembolism prophylaxis. She was discharged safely home on the third day.
The anatomical location of fibroids varies within the uterus. Figure 5 illustrates some locations of fibroid, which can be sub-serosal, sub-mucosal, intramural, and cervical. Sub- serosal fibroids can be further subcategorized into pedunculated and sessile [24].
Additionally, the European Society of Gynaecological endoscopy further classifies sub- mucosal fibroid based upon their involvement within the myometrium [25].

Figure created by author Dr. Aditi Shinde.
Figure 5: Anatomical locations of leiomyoma.
While most uterine fibroids are asymptomatic, their presentation can vary according to its anatomical location within the uterus. Sub-mucosal and intramural fibroids more commonly present with abnormal uterine bleeding. However, sub-serosal and pedunculated fibroids present with mass-effect symptoms such as bladder and bowel dysfunction, or pelvic pain [26].
In a retrospective descriptive study, Ekine et. al. collected the main clinical presentations of 368 women managed for uterine fibroid over a 5-year period [26]. Fibroids can affect fertility as well, however, it depends on size, number and site.
Table 1 depicts potential complications exhibited by leiomyoma and the relevant number of reported cases [27].
| Complication | Percentage of cases(%) |
| Red degeneration | 3% [28] |
| Intra-abdominal haemorrhage | < 1> |
| Torsion | < 0> |
| Infection | < 1> |
| Renal impairment | No collected data [32] |
| Venous thromboembolism | 2.2% [33] |
| Malignant transformation | <1> |
Table 1: Uterine fibroid complication and corresponding reporting rate.
When fibroids present with pain, important complications to consider include red degeneration [27], intra-abdominal haemorrhage [28, 29], torsion [30], infection [31], or malignant transformation [34].
In view of long NHS waiting list, that can be up to five years among 32% of patients [35], it is crucial to recognize these complications and triage appropriately. Emergency surgery should be taken into consideration and expedited if concerning symptoms or complications are identified. By focusing on clinical decision-making algorithms and individualized care, improvements in patient quality of life can be achieved through increasing work productivity by 36.1% and reducing disability lost years by 37.9% [35].
Torsion of fibroid occurs predominantly in sub-serosal fibroids, usually with a thin pedicle. If the pedicle torts, the accessory feeding vessel undergoes venous congestion and ischemic necrosis, causing symptoms of pain. Intermittent torsion and de-torsion of this vessel is responsible for
chronic symptoms. Other forms of resolution include calcification, amputation and intra-abdominal haemorrhage. Sometimes, this can lead to peritonitis and sepsis if neglected. Other rare complications also include renal impairment. If large enough, the fibroid can compress the pelvic ureters leading to hydroureter or hydronephrosis [36,37]. Intra-abdominal haemorrhage can also occur due to rupture of superficial vessels around the fibroid, and patients would present with severe abdominal pain and profound hypovolemic shock [38]. Venous thromboembolism is likely a result of venous stasis exhibited by large fibroids mechanically obstructing vessels in the pelvis and lower extremities [39]. Similarly, increased likelihood of thromboembolism could be a result of polycythaemia and reactive thrombocytosis secondary to menorrhagia [40]. Malignant transformation is the rarest complication with a presumed incidence of between 0.13- 0.29% [41]. These most commonly present as abnormal vaginal bleeding associated with a palpable abdominal mass, weight loss and weakness. Leisohn et. al. discussed how uterine leiomyosarcoma arise from leiomyoma therefore suggesting a degree of malignant transformation of the pre-existing leiomyoma [42].
Clinical decision-making algorithms should be used. Figure 6 reflects how these practices can be implemented in affected women. This can change according to the place of diagnosis, facilities available, clinical expertise and scope for minimally invasive surgery. There is scope for artificial intelligence (AI) algorithms and machine learning for review of images [43].
Figure created by author Dr. Aditi Shinde.
Figure 6: Clinical decision-making algorithm in women presenting with fibroid pain.
If a lady with a known fibroid presents with pain, it is essential to know the dimensions and type of fibroid she has. After clinical examination, an ultrasound, CT scan and MRI pelvis is essential in establishing a diagnosis. The following from table 2 are the features of uterine torsion on imaging and the differential diagnosis that should be considered.
| Imaging | Features [44, 45, 46] | Differential Diagnosis |
| Ultrasound | Normal uterus with heterogeneous echogenicity of pedunculated para- uterine mass. A mild pelvic free fluid colour doppler is demonstrated and shows twisted pedicle with no blood flow within the mass. There would be free fluid in the POD and haemato-peritoneum if associated with intra-abdominal haemorrhage. | Degeneration uncomplicated fibroids are hypo-echoic, calcification seen echoic foci with shadowing. Necrosis or degeneration seen as cystic area |
| CT scan | Inferior-most aspect of the non-enhancing fibroid is identified with surrounding inflammatory change with poor contrast enhancement, thin rim enhancement and a dark fan sign (described as fan-shaped poor contrast enhancement area of the uterus adjacent to the leiomyoma) | Fibroids with degeneration, has a central area of necrosis. Usually, the peripheral contrast enhancement would be preserved. |
| MRI | T1: intermediate to high signal intensity related to haemorrhagic necrosis, T2: peripheral low signal and central high signal intensity, T1 with contrast: no enhancement. | T1 irregular, T1 hyperintense rim around a centrally located myoma suggests red degeneration, which is caused by venous thrombosis. High T2 intensity. |
Table 2: Imaging features for uterine fibroid.
This case report demonstrates a rare acute presentation of a uterine fibroid which was successfully triaged and managed by a local unit. The implication of a missed diagnosis would be potentially life threatening and fertility impairing in this woman.
Key themes include preservation of fertility and utilization of an algorithmic approach to diagnosis. We learned we can reduce waiting times to surgery by accurately recognizing torsion on imaging.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
