
Research Article | DOI: https://doi.org/10.31579/jnmir/006
1 Apramitha Innovations Private Limited, Hyderabad, India.
2 Department of Dermatology, Venereology, Leprology (DVL) Gandhi Medical College and Hospital, Secunderabad, India.
*Corresponding Author: Srikanth Kalakoti, Apramitha Innovations Private Limited, Hyderabad, India.
Citation: Srikanth Kalakoti, G. Narasimharao Netha. Topical Application of Apremilast in the Treatment of Mild to Moderate Psoriasis, J. New Medical Innovations and Research, 2(1): DOI: 10.31579/jnmir/006
Copyright: © 2021 Srikanth Kalakoti. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 December 2020 | Accepted: 10 February 2021 | Published: 22 February 2021
Keywords: psoriasis; mild to moderate psoriasis; apremilast; topical dosage form; PDE4 inhibitor; topical therapy
Background: Psoriasis is a chronic, autoimmune disorder that affects the skin and joints with an approximate global prevalence of 2–3%. Mild to moderate psoriasis is highly prevalent in about 80% of the global psoriatic population (2-3%). Currently available treatment options for mild to moderate psoriasis are topical dosage forms. Though a variety of topical formulations available, they are associated with different side effects. There is an unmet need for a product that can be used for a prolonged period with minimal side effects. Hence, Apremilast gel was developed and clinical proof of concept study (POC) was performed to investigate the efficacy and safety in mild to moderate psoriasis patients.
Methods: A single-center randomized, double-blind, placebo-controlled study was conducted to evaluate the efficacy and safety of apremilast topical gels 2% & 4% w/w, in adult mild to moderate psoriatic patients for 12 weeks. Patients were examined at weeks 0, 2, 4, 8, and 12 weeks to assess the efficacy and safety. At 0 and 8 weeks, blood samples were collected to investigate the pharmacokinetics. The significance in % recovery was calculated statistically.
Results: Both gels exhibited a significant reduction in PASI values when compared with baseline PASI scores. The average percentage inhibition of PASI with test products i.e. 2% and 4% w/w Apremilast topical gels is about 46.8% and 34.6% respectively after 12 weeks of treatment. Both the test products have not shown any adverse effects, hematological & biochemical changes and have exhibited Cmax less than 20ng/ml after 6 hours of application.
Conclusion: Results have shown that topically applied apremilast could be an effective and safe option for the management of mild to moderate psoriasis.
Psoriasis is a common, chronic, inflammatory dermatosis seen in practice. The disease is characterized by erythematous, well-demarcated plaques and rounded scales which look like silvery mica [1]. Pruritus may also present in certain cases. Lesions are usually symmetrical and occur on the extensor surfaces such as the elbows knees and on scalp [2]. Psoriasis associated with pruritus results in frequent scratching and contributes substantial psychological, social, and quality of life problems to patients and their families [3]. The current therapy only suppresses the disease symptoms and recurrence is common after stopping the treatment [4, 5]. The disease may undergo spontaneous remission. The treatment of psoriasis depends on the type, the location, and the extent of the lesions [6]. Drugs used in the management of psoriasis include topical emollients, keratolytic agents such as salicylic acid; cytostatic agents such as coal tar, dithranol, glucocorticoids; vitamin D analogs such as calcipotriol; systemic agents etretinate, immunosuppressants such as methotrexate, cyclosporine, mycophenolate; biological agents T cell activation inhibitors such as efalizumab, alefacept; TNF-alpha inhibitors etanercept, infliximab and systemic glucocorticoids [7]. Mild to moderate cases of psoriasis may not warrant any systemic drug therapy, since drugs used in the systemic route can produce toxicity [8]. Topical treatments are commonly prescribed to alleviate psoriasis symptoms, reduce inflammation, and prevent flares. But no new molecules have been approved for the topical treatment of psoriasis in the past few years and treatment guidelines recommend the use of topical corticosteroids, vitamin D analogs, or both.
Corticosteroids are the first-line treatment in the management of psoriasis irrespective of the disease type (mild, moderate or severe) because of their high beneficial levels and are available in a variety of dosage forms including ointment, cream, gel, spray, foam, lotion, etc. But are associated with various side effects such as atrophy, telangiectases, striae, traumatic purpura, perioral dermatitis, hypertrichosis, etc [9].
Vitamin D analogs are another kind of widely accepted topical preparations to manage psoriasis. These manage psoriasis by inhibiting the keratinocyte growth, promote keratinocyte differentiation, and decrease inflammation in psoriatic lesions via vitamin D receptors on keratinocytes and T lymphocytes [10, 11]. Adverse effects such as irritation, hypercalcemia, etc are surfaced with these agents. The studies reported that skin irritation was prominent in sensitive areas such as the face, etc and around 20% of the population reported skin irritation in those sensitive areas [12, 13].
Despite their efficacy, these topical agents are associated with a variety of limitations in their use as a result of application site reactions and safety concerns with long-term use. Hence, novel topical therapies that may potentially improve upon the risk-benefit profile of current treatment options are needed.
Phosphodiesterase 4 (PDE4) is a key regulator of inflammatory cytokine production in psoriasis by blocking the degradation of cyclic adenosine monophosphate [14]. PDE4 activity is increased in circulating inflammatory cells of patients with psoriasis and the inhibition of PDE4 in monocytes in vitro has demonstrated a reduction in the release of pro-inflammatory cytokines [15]. The oral PDE4 inhibitor, apremilast was recently approved for the treatment of psoriatic arthritis and moderate to severe psoriasis [16]. Apremilast inhibits the PDE4 which leads to an increase in the levels of the cyclic adenosine monophosphate, a naturally occurring intracellular secondary messenger that acts as a modulator of inflammatory responses. This leads to the decreasing production of the pro-inflammatory mediators, such as tumor necrosis factor (TNF)-α, interleukin (IL)-23, and interferon-gamma, and increasing production of anti-inflammatory mediators, such as IL-10 [17-19].
Apremilast oral tablets require dose titration to avoid gastrointestinal side effects (nausea and diarrhea) precipitated with the inhibition of PDE4 in non-target tissues [8]. A topical PDE4 inhibitor formulation could address the need for targeted inflammation in skin disease while avoiding undesirable side effects warranted by broad systemic exposure. Hence, an attempt has been made to develop the Apremilast, PDE4 inhibitor, topical gel to treat mild to moderate psoriasis. The gel will appear white to off-white viscous in nature and consists of different inactive ingredients like carbopol, dimethyl sulfoxide, propylene glycol, glycerin, methyl and propyl parabens, ethanol, etc. A prototype clinical proof of concept study was performed to evaluate the efficacy and safety of apremilast topical gel, 2% and 4% in patients aged more than 18 years with mild to moderate psoriasis.
Although systemic exposure to apremilast upon topical administration may vary with the percentage of body surface area that gets exposed to the medication, the severity of the disease lesions, and skin condition, it was objected to delivering the zero or minimal systemic concentrations. This novel topical dosage form of apremilast exhibited the drug release to sufficient to elicit pharmacological action and minimized the concentration in the systemic circulation which then helped in minimizing side effects associated with oral apremilast tablets.
Study design
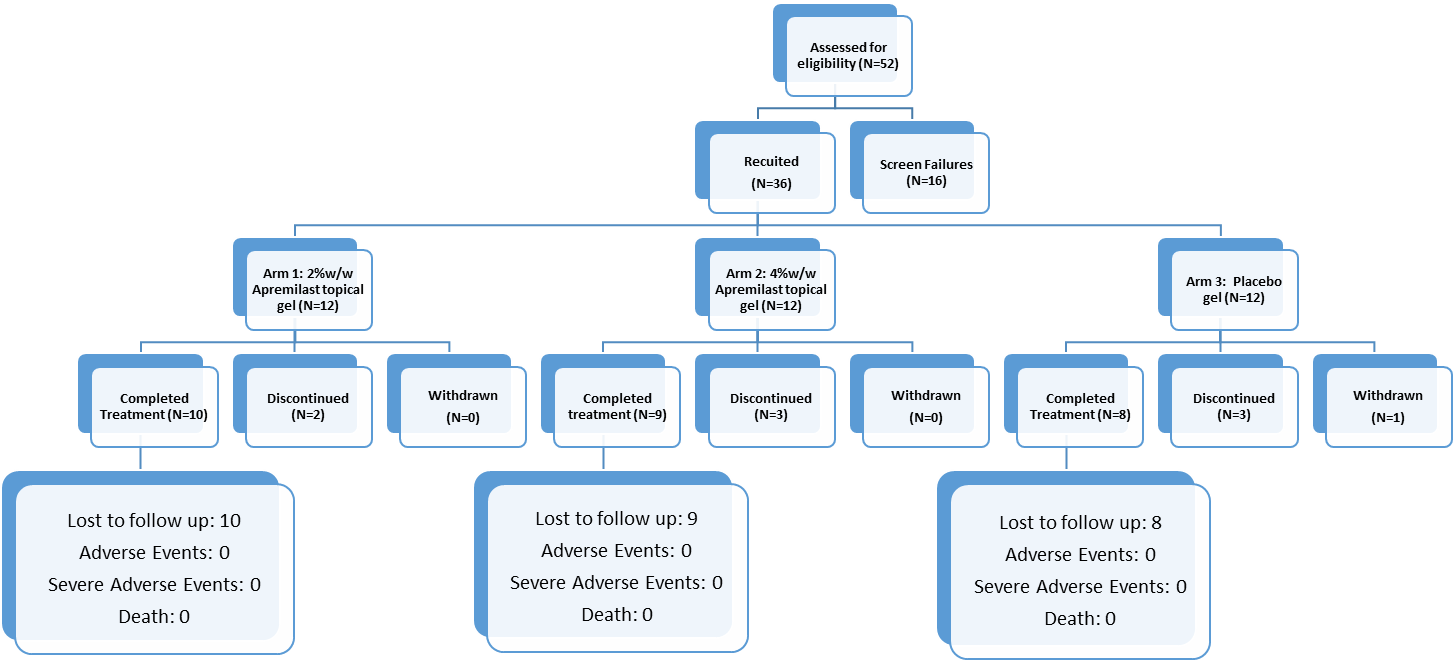
The efficacy and safety of Apremilast Topical Gels, 2%, 4% w/w and placebo, in patients with mild to moderate psoriasis were evaluated in a 12-week, Randomized, double-blind, placebo-controlled, three-arm parallel study conducted in 36 volunteers at Gandhi Medical College, Secunderabad, India. The institutional review board approved all study protocols, consent/assent forms, and relevant supporting data. No participant (principal investigator, study staff, participants, parents/guardians, etc) knew the treatment assignment, and blinding was maintained throughout clinical management, data management, and statistical evaluation. The study consisted of a screening visit, a washout period of 14 days, a baseline/randomization visit (0 weeks), and study assessments at weeks 2, 4, 8, and 12. Flow Diagram of the Study is given in figure 1.

Ethical issues
This study was conducted in compliance with the Declaration of Helsinki and the study protocol was reviewed and approved by the Institutional Ethics Committee, Gandhi Medical College & Hospital, Secunderabad, India (DCGI Regd No: ECR/180/Inst/AP/2013/RR-16, Dt.21.06.2017) and the registered no: IEC/GMC/2018/12, Dt. 30.03.2018. The purpose of the study was clearly illustrated to each patient and collected the consent in written from each patient.
Patient’s inclusion and exclusion criteria
A total of 36 patients with mild to moderate psoriasis (Psoriasis Area Severity Index (PASI) < 10) were included in the study. A randomization schedule was prepared using software SAS, Version 9.2, and volunteers are allocated to the individual groups as per the schedule. The inclusion and exclusion criteria of the patients are as follows.
Patient’s inclusion criteria
Patient’s exclusion criteria
Intervention
Eligible patients gave written consent and underwent treatment with Apremilast/ Placebo topical gel by applying on the affected area twice daily for 12 weeks. Concurrent use of any topical and oral anti psoriasis medications was not allowed during the study.
Apremilast gel treatment
On the day of randomization, the baseline area (psoriasis affected area) was determined by taking the photographs and PASI scores were recorded under the supervision of the principal investigator. Patients were asked to apply a layer of gel on psoriasis affected area twice daily throughout 12 week study period, to apply test drug as needed, and to newly identified psoriatic lesions that appeared after day 1. PI also instructed to subjects to visit bi-weekly or monthly (Week 2, 4, 8 and12) for reviewing the efficacy and safety as per the schedule.
Evaluation
Study assessments i.e. efficacy and safety were performed at weeks 2, 4, 8, and 12 of treatment. The PASI scores were recorded at all visits under the supervision of the principal investigator. Pharmacokinetics of topically administered apremilast was studied by collecting and analyzing the blood samples from the few patients of all three arms on week 0 and week 8. Blood samples collected at 0 hr (pre-dose), 1hr, 1.50 hr, 2 hr, 2.50 hr, 3 hr, 4 hr, and 6hrs after the morning application of the formulation at the investigator’s clinic. The plasma samples are analyzed using a bioanalytical method developed in LC-MS/MS.
Clinical laboratory testings (hematology, biochemistry, and urinalysis) and vital signs were recorded at the time of randomization and after completion of treatment whereas AEs, SAEs, and physical examinations were monitored at all visits during the treatment period. The baseline patients and disease characteristics are presented in Figure 2.
Efficacy
The primary efficacy endpoint is to assess the mean percentage change from baseline in PASI at Week 8 and 12. Reduction in PASI scores with 2% and 4% gels by 50%, 75%, and 90% are computed by comparing with baseline PASI score after 12 weeks of treatment. Signs of psoriasis were measured throughout the treatment period on investigator visit days of weeks 2, 4, 8, and 12.
The secondary efficacy endpoints are checking the safety and tolerability of the gels throughout the study period and also measuring the systemic exposure of apremilast in a subset of patients at weeks 0 and 8.
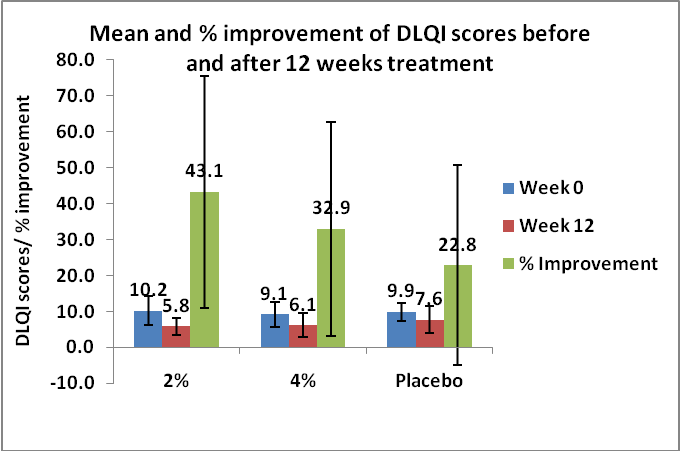
Dermatology Life Quality Index (DLQI) was also considered as one of the measures to assess the efficacy of the developed apremilast topical gels, 2%, 4%, and placebo. DLQI scale was recorded before and after the treatment with the apremilast topical gels and placebo. The results are presented in figure 3.

Safety
The Primary Safety evaluations included adverse events (AEs), vital signs, X-ray, electrocardiography (ECG), and clinical laboratory parameters including hematological and biochemical limits.
Safety was evaluated by monitoring AEs, clinical laboratory testings (hematology, biochemistry, and urinalysis), vital signs, and physical examinations. Adverse events were categorized based on the severity and relationship to the study drug. Adverse Events that occurred post-treatment (events that occurred after the first dose of medication and up to 14 days post-treatment) were also recorded. The appearance of newer lesions post-randomization was not captured as AEs but captured separately in CRFs.
Statistical analysis
Statistical analysis of clinical efficacy of apremilast topical gels was carried out with Wilcoxon rank-sum test and the differences were considered as statistically significant when p < 0.05. In order to verify the homogeneity of the three groups, age and baseline disease intensity (baseline PASI scores) between the groups were compared. Baseline PASI scores of 2%, 4%, and placebo groups were compared with PASI scores observed after 12 weeks of treatment.
The % population achieved PASI 50, 75, and 90 with apremilast topical gel was compared with Phase II and Phase III clinical trials data of apremilast oral tablets intended for moderate to severe psoriasis available in the literature.
A total of 52 volunteers were scrutinized, 36 of whom were recruited and were randomized into three groups, 2%, 4%, and placebo groups, at a ratio of 12: 12: 12. 16 volunteers did not meet the inclusion criteria and were excluded.
Of the 12 patients in 2% Apremilast topical gel arm, 10 completed the treatment period of 12 weeks and also responded in the follow-up period (28 days) and 2 did not complete the study. Of the 12 patients in 4% Apremilast topical gel arm, 9 completed the treatment period of 12 weeks and also responded in the follow-up period (28 days) and 3 did not complete the study. Of the 12 patients in the placebo gel arm, 8 completed the treatment period of 12 weeks and also responded in the follow-up period (28 days), 3 did not complete the study and one was withdrawn from the study as he did not respond to the treatment. The patient disposition details are presented in figure 2.
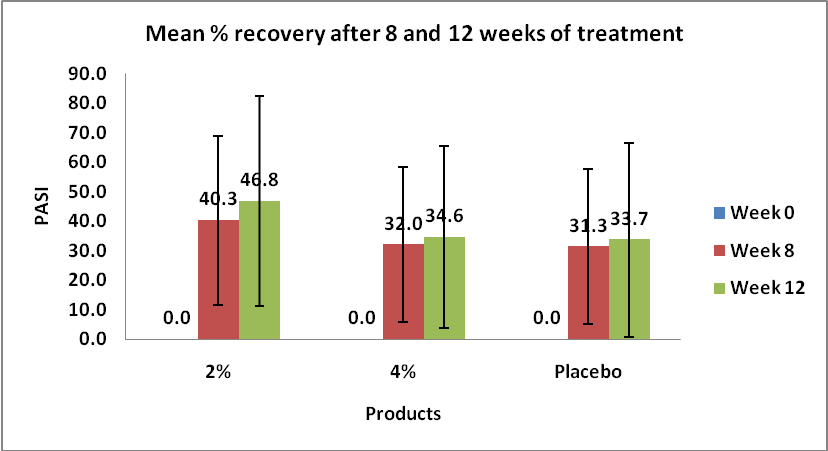
A significant reduction in PASI scores was observed with test products after 12 weeks of treatment when compared with the baseline PASI scores. The mean % recovery with 2% and 4% gels are 46.8% and 34.6% respectively. The percentage of patients who exhibited PASI 50, PASI 75, and PASI 90 with 2% apremilast topical gel are 60.0%, 40.0%, and 10.0% respectively whereas with 4% Apremilast topical gel are 33.3%, 11.1%, and 11.1% respectively. The % recovery with 2% and 4% gels approximately similar and the variation in the PASI with 2% and 4% gels maybe because of variation in the initial PASI scores. The data presented in Figures 4 and 5.

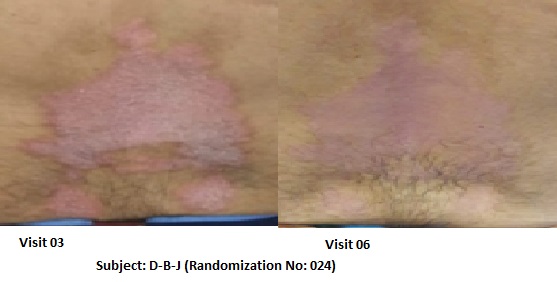
Figures 6 and 7 are the pictorial presentations of the percentage recovery before and after treatment. The mean % improvement of DLQI with 2% and 4% gels are 43.1% and 32.9% respectively. The data presented in figure 6.
During the study period and after completion of treatment, patients were examined for different adverse events, serious adverse events, physical examinations and vital signs.
None of the test products including placebo have shown any side effects like irritation, redness, itching or swelling throughout the study period. No hematological and biochemical changes noticed in the subjects after completion of treatment when compared with an initial assessment. No adverse events and serious adverse events (SAEs) were reported with three products (Table 1).
Product | Apremilast Topical Gel | Apremilast Tablets | ||||
Strength | 2%, 4% w/w and Placebo | 30mg | ||||
Indication | Mild to moderate psoriasis | Moderate to severe psoriasis | ||||
Route of administration | Topical | Oral | ||||
Treatment period | 12 weeks | 16 weeks | ||||
Dosage form | Topical Gel | Oral tablets | ||||
Phase of the study | POC | Phase II | Phase II | Phase III | ||
No of subjects | 12 | 12 | 12 | 85 | 88 | 562 |
scores obtained | Actual values* | Literature | ||||
Code of the Product | 2% | 4% | Placebo | Japan | US & Canada | 8 different countries including US & Canada |
PASI50 (achieving 50) | 60.0 | 33.3 | 12.5 | 29.2 | 35.2 | 41.7 |
PASI75 (achieving 75) | 40.0 | 11.1 | 12.5 | 21.1 | 35.2 | 27.8 |
PASI90 (achieving90) | 10.0 | 11.1 | 0 | 12.9 | 10.2 | 9.4 |
Reported adverse events (%) | ||||||
Nasopharyngitis | 0 | 0 | 0 | 11.8 | 5.7 | 7.3 |
Diarrhoea | 0 | 0 | 0 | 9.4 | 13.6 | 18.8 |
Abdominal discomfort | 0 | 0 | 0 | 7.1 | NR | NR |
Psoriasis | 0 | 0 | 0 | 4.7 | 0 | NR |
Nausea | 0 | 0 | 0 | NR | 19.3 | 15.7 |
Tension Headache | 0 | 0 | 0 | NR | 15.9 | 5.5 |
upper respiratory tract infection | 0 | 0 | 0 | NR | 15.9 | 10.2 |
Reported severe adverse events (%) | ||||||
SAE (%) | 0 | 0 | 0 | 0 | 4.5 | 2.1 |
NR-Not reported
# data presented in terms of percentages (%)
Table 1: PASI score changes in volunteers used test formulations (Apremilast Topical Gels 2%, 4% and placebo, BID) for 12 weeks from topical route to treat mild to moderate psoriasis.
At weeks 0 and 8 of treatment, blood samples collected from a subset of patients and were analyzed for plasma concentrations of apremilast to assess the systemic exposure levels from both gels (Table 2). An average Cmax of 6.5ng/ml and 3.5 ng/ml on the day of randomization and 4.25 ng/ml and 6.82 ng/ml on week 8 of plasma concentrations of apremilast found with 2% and 4% gels respectively. The absorbed drug from both gels is too less which indicates the maximum amount of drug retaining in the skin layers and eliciting the effect. This could be the reason for zero AEs and SAEs.
Clinical laboratory evaluation was also assessed before and after treatment by the principle investigator. There was no significant change in clinical laboratory parameters in all patients. The mean clinical laboratory results of the subjects who completed 12 weeks of treatment are reported in Tables 2 and 3.
S No | Test | Normal Range | Before | After | ||
Range | Average | Range | Average | |||
1 | Haemoglobin | 13-17 g/dl | 11-14 | 14 | 10-17 | 13 |
2 | PCV/HCT | 40-50% | 33-48 | 41 | 32-50 | 39 |
3 | Total RBC count | 4.5-5.5mill/cumm | 3.6-5.8 | 4.8 | 3.4-6.5 | 4.6 |
4 | Total WBC count | 4000-10000 cells/cumm | 5100-12600 | 8088 | 4900-25600 | 8475 |
5 | Platelet count | 1.5-4.1 lakhs/cumm | 1.6-4.3 | 2.9 | 1.6-4.2 | 2.8 |
6 | Neutrophils | 40-80% | 42-79 | 60 | 46-86 | 64 |
7 | Lymphocytes | 20-40% | 16-43 | 29 | 8-42 | 27 |
8 | Eosinophils | 1-6% | 1-11 | 3 | 0-7 | 2 |
9 | Monocytes | 2-10% | 4-10 | 7 | 2-10 | 6 |
10 | Basophils | 0-2% | 0-2 | 1 | 0-1 | 0 |
Table 2: Summary of Haematology results of all the subjects | ||||||
S No | Test | Normal Range | Before | After | ||
Range | Average | Range | Average | |||
1 | Total bilirubin | 0.3-1.2 mg/dl | 0.4-2.7 | 0.7 | 0.2-2.3 | 0.7 |
2 | Direct bilirubin | <0.2 mg/dl | 0.1-0.3 | 0.1 | 0.1-0.3 | 0.1 |
3 | Indirect bilirubin | 0-0.8 mg/dl | 0.3-2.4 | 0.6 | 0.1-2.0 | 0.6 |
4 | ALT (SGPT) | <50 IU/L | 9-49 | 24.7 | 9.0-76.0 | 25.6 |
5 | AST (SGOT) | <50 IU/L | 16-44 | 25.3 | 17-57.0 | 27.6 |
6 | Alkaline phosphate | 30-120 IU/L | 56-158 | 95.4 | 56-159 | 98.2 |
7 | Total protein | 6.6-8.3 g/dl | 6.6-7.5 | 7.5 | 6.4-8.4 | 7.4 |
8 | Albumin | 3.4-5 g/dl | 3.6-5 | 4.3 | 3.7-4.9 | 4.2 |
9 | Globulin | 1.8-3.8 g/dl | 2.4-4.2 | 3.1 | 2.3-4.1 | 3.2 |
10 | A/G ratio | 0.9-1.8 | 0.9-2 | 1.4 | 1.0-1.9 | 1.4 |
11 | Random plasma glucose | 70-140 mg/dl | 76-181.3 | 99.5 | 64-239 | 104.9 |
12 | Serum creatinine | 0.67-1.17 mg/dl | 0.3-1 | 0.7 | 0.4-1.0 | 0.7 |
13 | Blood urea | 17-43 mg/dl | 9-36 | 20.3 | Oct-30 | 18.7 |
14 | Uric acid | 3.5-7.2 mg/dl | 2.8-8.2 | 5.2 | 3.5-7.6 | 5.3 |
Table 3: Summary of Biochemistry results of all the subjects
The p values substantiated that there is homogeneity in the age and initial PASI scores between the active gels and placebo gel groups (non-significant variation). This indicates that there is no influence of age and initial PASI scores on % recovery. The statistically significant % recovery was observed, based on p-values, with 2% gel product and no significant recovery observed with 4% gel product placebo gel indicating that test product having clinical efficacy. The p values are reported in Table 4.
S No | Treatments | p-value calculated using Wilcoxon rank-sum test with continuity correction | Remarks |
Age | |||
1 | 2% Vs Placebo | 0.0836 | Non-significant |
2 | 4% Vs Placebo | 0.7027 | Non-significant |
PASI before Initiating the study | |||
1 | 2%Vs Placebo | 0.130 | Non-significant |
2 | 4%Vs Placebo | 0.141 | Non-significant |
Comparison of baseline PASI vs PASI after 12 weeks of treatment (3rd visit PASI vs 7th visit PASI) | |||
1 | 2% | 0.038 | Significant |
2 | 4% | 0.064 | Non-significant |
3 | Placebo | 0.092 | Non-significant |
Table 4: Significance levels (p values) between the products based Wilcoxon rank-sum test with continuity correction.
Based on the mean % change in PASI, AEs, SAEs, pharmacokinetic data, and on comparing the oral apremilast tablets data, it was concluded that both test products 2% and 4% gels were effective in the treatment of mild to moderate psoriasis.
Apremilast topical gel, a novel PDE4 inhibitor, significantly reduced the signs and symptoms of mild to moderate psoriasis in patients. Its positive efficacy profile was based on 1) decrease in disease severity 2) reduction in psoriasis signs and symptoms; and 3) early and sustained improvement with no side effects. This novel topical dosage form showed improved quality of life by decreasing the psoriasis signs and disruption of itch-scratch cycle.
The significant efficacy of topical apremilast versus placebo was observed in the study. In treating patients with psoriasis, a topical treatment should ideally disturb the inflammatory process and provide protective benefits including improving the skin barrier to reduce antigen access and increasing skin hydration by preventing transdermal water loss. As such topical drug placebos have physiological cutaneous effects, adding to the drug effect in improving the outcome for patients. The incorporation of apremilast into the placebo significantly improved the efficacy in treating psoriasis.
The % recovery (PASI 50, PASI 75, and PASI 90) achieved with topical apremilast gel was compared with % recovery (PASI 50, PASI 75, and PASI 90) achieved with oral apremilast Tablets in Phase II and Phase III clinical trial data. Apremilast tablets, 30 mg (OTEZLA), are indicated for the treatment of adult patients with moderate to severe plaque psoriasis who are candidates for phototherapy or systemic therapy. Although the study duration and indication are slightly different, the data were compared to assess the effectiveness of the topical gel.
Phase II clinical trials oral apremilast tablets carried out in Japan and US&Canada with oral apremilast tablets reported that 29.2 and 35.2% of volunteers have achieved PASI 50. Similarly, phase III clinical trials organized in 8 different countries exhibited that the PASI 50 was achieved by 41.7% of volunteers. While PASI 50 achieved with 2% and 4% apremilast topical gels (60.0% and 33.3%) are comparable with PASI 50 data obtained in clinical trials carried out with oral apremilast tablets. Although there is variation in the treatment period between topical gel (12 weeks) and oral tablets (16 weeks), the 2% and 4% topical gels have shown as good recovery as that of oral apremilast tablets approximately. The efficacy of both gels (2% and 4% gels) may further increase either on increasing the number of subjects or increasing the treatment period to 16 weeks and it may be higher when compared with oral apremilast tablets.
No adverse events and serious adverse events (SAEs) were reported with three products whereas the oral apremilast tablets reported many AEs and SAEs during 16 weeks of treatment (Table 5).
Visit | Week 0 (Visit 3) | ||||||||
Parameter | Tmax (hrs) | Cmax (ng/ml) | AUC (hr*ng/mL) | ||||||
Formulation | 2% | 4% | Placebo | 2% | 4% | Placebo | 2% | 4% | Placebo |
N | 8 | 7 | 6 | 8 | 7 | 6 | 8 | 7 | 1 |
Mean | 4.8 | 5.4 | 0.7 | 6.5 | 3.5 | 0.9 | 11.5 | 7.1 | 0.3 |
SD | 1.7 | 1 | 1.6 | 5.2 | 2.3 | 0.2 | 9.2 | 5.4 | - |
Range | 2.0-6.0 | 4.0-6.0 | 0.0-4.0 | 1.1-13.9 | 0.6-7.2 | 0.0-0.5 | 2.9-30.0 | 0.6-15.2 | 0.3-0.3 |
Geo.mean | 4.5 | 5.3 | - | 4.5 | 2.7 | - | 8.6 | 4.9 | 0.3 |
Visit | Week 8 (Visit 6) | ||||||||
N | 4 | 4 | 7 | 4 | 4 | 7 | 4 | 3 | 2 |
Mean | 4.3 | 4.5 | 1.4 | 4.3 | 6.8 | 0.5 | 14.1 | 36.1 | 5.2 |
SD | 2.0 | 3.0 | 2.5 | 1.8 | 7.7 | 0.9 | 9.1 | 25.4 | 6.9 |
Range | 2.5-6.0 | 0.0-6.0 | 0.0-6.0 | 1.9-5.8 | 0.0-17.1 | 0.00-2.5 | 5.8-26.9 | 10.2-60.9 | 0.4-10.2 |
Geo.mean | 3.9 | -- | -- | 3.9 | -- | -- | 12.1 | 28.5 | 1.9 |
Table 5: Pharmacokinetic data of Apremilast topical gels and placebo at weeks 0 and 8.
Because of severe adverse side effects and restricted long-term use of topical corticosteroids and topical vitamin D analogs, a safe and effective topical alternate is needed to treat mild to moderate psoriasis. Topical apremilast gel has low systemic absorption reducing the risk of systemic side effects, making it an encouraging treatment alternate to exiting topical therapies. Twice daily application of apremilast gels for 12 weeks demonstrated a favorable safety profile in the study based on (a) low or no incidence of treatment-related adverse events, (b) no serious treatment-related adverse events, (c) low discontinuation rates, (d) no change in hematological or biochemical parameter changes, and (e) no change in vital signs. These efficacy and safety profiles of the novel topical formulation of apremilast gel allow localized therapy at the site of inflammation and reducing the risk of systemic side effects observed with oral apremilast and other PDE4 inhibitors
No adverse events reported with topical apremilast gel including the gastrointestinal adverse events observed with oral apremilast tablets. No subject reported cutaneous AEs such as skin atrophy. Application site irritation is a commonly reported side effect with topical corticosteroids and topical vitamin D analogs. Although a direct comparison study with these agents is not performed, apremilast gel demonstrated a very low incidence of application site irritation or itching. Overall, twice daily application of apremilast topical gel to all areas of the body for 12 weeks treatment demonstrated favorable safety and efficacy profiles.
Topical apremilast gel signifies a first in class non-steroidal topical treatment that inhibits overactive PDE4 in psoriasis to reduce local signs and symptoms that drives exacerbation of the disease. The anti-inflammatory effect on psoriasis pathology is clear, and topical apremilast also provided early and sustained improvement in reducing the red, raised, inflamed patches of skin. The mechanism through which PDE4 regulates red, raised, inflamed patches of the skin is not well understood but is believed to be partially an indirect result of reducing inflammation.
Apremilast topical gel represents a promising new option for patients with mild to moderate psoriasis based on the favorable safety and efficacy profiles. Further, studies need to explore to confirm the potential of topical apremilast gel in patients with impaired renal function.
Apremilast topical gel decreased the disease severity by subsiding the signs and symptoms of psoriasis. The gel product also demonstrated a favorable safety profile in which none of the patients have reported any adverse events. No patients have stopped the medication due to serious adverse effects. Treatment with topical apremilast was well tolerated. In addition, no clinically meaningful differences were observed in the patient’s vital signs, electrocardiograms, and clinical laboratory parameters between treatment groups. Overall, apremilast topical gel targets the principal mechanism of the disease and has the prospective to meritoriously treat mild to moderate psoriasis without the limitations of current treatment options.
The authors are indebted to the patients that participated in the study. The authors would like to thanks the support given by the Management and staff of Gandhi Medical College & Hospital, Hyderabad, India.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
