
case report | DOI: https://doi.org/10.31579/2690-4861/687
Hospital da Senhora da Oliveira, Guimarães, Portugal
*Corresponding Author: Leite Letícia Marques, Hospital da Senhora da Oliveira, Guimarães, Portugal.
Citation: Leite L. Marques, Silva Sara, Ribeiro Elisabete, Bessa I. Mendes, (2025), Tongue Deviation as a Manifestation of Paraganglioma, International Journal of Clinical Case Reports and Reviews, 23(1); DOI:10.31579/2690-4861/687
Copyright: © 2025, Leite Letícia Marques. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2024 | Accepted: 23 January 2025 | Published: 01 February 2025
Keywords: neuroendocrine tumor; hypoglossal
Cervical paragangliomas are typically of parasympathetic origin, asymptomatic until they cause compression of surrounding tissues and nerves. The presented clinical case represents a paraganglioma diagnosed after hypoglossal nerve palsy.
Early diagnosis and genetic testing allow for earlier treatment and individualized follow-up, as well as enabling the screening of family members and integrating them into an appropriate screening program.
Paraganglioma is a neuroendocrine tumor originating from the paravertebral ganglia of the sympathetic nervous system or from the parasympathetic ganglia, most commonly in the vagus and glossopharyngeal nerves present in the neck and skull base. Paragangliomas are classified as catecholamine-secreting and non-catecholamine-secreting. Catecholamine-secreting paragangliomas have nonspecific symptoms, including paroxysmal hypertension, headache, tachycardia, diaphoresis, and anxiety. Parasympathetic paragangliomas, which are frequently non-secreting, present symptoms resulting from the mass effect on surrounding tissues and nerves.
We present the clinical case of a 43-year-old woman with no relevant personal medical history, who had a progressive increase in a right lateral cervical swelling over the course of one year. She also presented with ipsilateral tongue deviation over the last 15 days. On physical examination, a mass was noted below the mandibular angle and right carotid triangle, measuring 5 cm x 3.5 cm, with irregular contours, firm consistency, adherent to the underlying tissues, non-tender on palpation, without warmth or redness. The tongue protruded with deviation to the right and fasciculations on the right side (figure 1). There was difficulty in tongue mobility, such as curling it and laterally moving it to the left.

Figure 1: Tong deviation to the right and fasciculations on the right side (hypoglossal nerve palsy)
A computed tomography (CT) scan of the neck was performed, which showed the presence of an expansive, enhancing mass measuring 4.5 x 3 cm, centered in the carotid space, without a cleavage plane with the carotid artery or internal jugular vein. The mass had superior internal extension, partially occupying the parapharyngeal space and was inseparable from the right pharyngeal wall (figure 2).
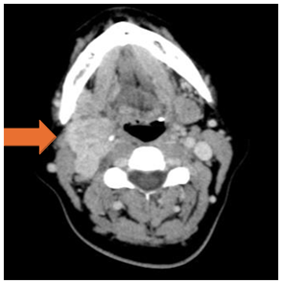
Figure 2: Mass centered in the right carotid space (orange arrow).
The cervical magnetic resonance imaging (MRI) revealed a mass measuring 4.5 x 5.6 cm, with a "salt-and-pepper" signal on T1 and T2, hypervascular, with probable origin from the carotid body. The internal jugular vein was obliterated by the lesion, and both the internal and external carotid arteries were surrounded by the mass.
Urinary and plasma metanephrines and catecholamines were negative, as well as vanillylmandelic acid and chromogranin A.
As a complementary study, a thoraco-abdominal-pelvic CT scan was performed, which showed multiple bilateral pulmonary nodular lesions, with a maximum diameter of 6 mm, suggestive of metastases. The Gallium-68-DOTA-TOC positron emission tomography (PET) scan revealed abnormal uptake with abnormal overexpression of somatostatin receptors in the right lateral cervical mass (image 3), in the pulmonary nodules, and in bilateral mediastinal-hilar lymph nodes.
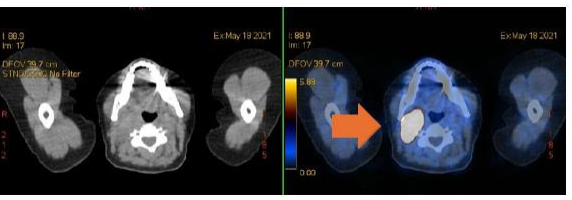
Figure 3: Abnormal uptake with abnormal overexpression of somatostatin receptors in the right lateral cervical mass in the Gallium-68-DOTA-TOC PET (orange arrow).
The patient was referred to the Oncology consultation with a diagnosis of metastatic non- secretory paraganglioma, with a positive genetic test for the SDHB mutation. Initially, she underwent partial embolization of the paraganglioma. She also started therapy with somatostatin analogs. After 4 years, she maintains clinical and radiological stability. During the follow-up period, a family genetic study was performed, where a brother tested positive for the SDHB mutation.
A thorough clinical, biochemical, radiological, and morphological evaluation is essential in the diagnosis of paraganglioma. Genetic analysis has become particularly important in recentyears due to its prognostic and therapeutic value. The SDHB mutation is associated with 40% of metastatic paragangliomas, indicating a worse prognosis and a higher risk of neoplasms. When this mutation is detected or a hereditary syndrome is established with more cases in thefamily, more regular screenings can be performed, leading to earlier diagnoses and treatments. [1].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
