
case report | DOI: https://doi.org/10.31579/2690-4861/587
1Department of Cardiac Surgery, LMU Hospital, Munich, Germany.
2Department of Vascular Surgery, LMU Hospital, Munich, Germany.
*Corresponding Author: Caroline Radner, Department of Cardiac Surgery LMU Hospital Munich Marchioninistrasse 15 81377 Munich, Germany.
Citation: Caroline Radner, Maja Hanuna, Linda Grefen, Christian Hagl, Nikolaos Tsilimparis, et al, (2024), To stent or not to stent – a Case Report on Left Ventricular assist Device outflow Graft Stenosis, International Journal of Clinical Case Reports and Reviews, 19(5); DOI:10.31579/2690-4861/587
Copyright: © 2024, Caroline Radner. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 October 2024 | Accepted: 29 October 2024 | Published: 21 November 2024
Keywords: lvad; endovascular treatment options; outflow graft stenosis
Left ventricular assist devices (LVADs) have evolved from a bridge to heart transplantation to a more common destination therapy for end-stage heart failure. Complications such as outflow graft stenosis, with a reported probability of 6% at 5 years post-LVAD support, pose significant challenges. Emergent surgical decompression or cardiac transplant are typical therapies, with few reports on outflow graft stenting, none involving the BeGraft® aortic stent.
A 68-year-old man with a HeartMate 3TM LVAD presented with recurrent low-flow alarms two years post-implantation. CT angiography revealed high-grade outflow graft stenosis near the ascending aorta. Intervention involved percutaneous femoral access, deployment of a BeGraft Aortic stent, and subsequent observation in the intensive care unit (ICU). Post-intervention CT angiography showed patent outflow graft, with discharge occurring after eight days without complications.
Endovascular techniques offer low-risk, high-survival solutions for complex LVAD-related complications, like outflow graft stenosis. Our case highlights successful use of the BeGraft® aortic stent, offering high radial force and post-dilation options. Careful patient selection and evaluation are essential for optimal outcomes in endovascular treatment of outflow graft stenosis.
Left ventricular assist devices (LVADs), which were initially thought of as a device to bridge to a heart transplantation in end-stage heart failure, have become more commonly accepted as suitable destination therapy. With long-term support and rising patient numbers with extended support time, complications are surfacing. Several potential problems like kinking, thrombus formation, infection and, more dangerous, progressive stenosis of the outflow graft, with a probability of 6% at 5 years of LVAD support, have been described [1,2]. These stenoses have been postulated to arise from deposition of gelatinous protein-rich or thrombofibrinous biodebris from blood contents leaking through the prosthesis wall [3]. This leads to impaired perfusion and subsequently thrombus formation as well as ventricular unloading [2].
The therapy most commonly described for outflow graft stenosis is emergent surgical decompression and, as a last resort, urgent cardiac transplant. There are, however, quite a few reports of outflow graft stenting to relieve the problem, but none of them with the BeGraft® aortic stent [1]. The probability of stenosis recurrence is 0% at 2 years, but up to 10% at 3 years post-intervention. In this report, we describe a safe and effective approach for managing outflow graft stenosis and present detailed outcomes associated with this method.
A 68-year-old man, who had received a HeartMate 3TM LVAD, by Abbott ®, for mixed dilated-ischemic cardiomyopathy in 2021, presented to the emergency room 2 years after LVAD placement with recurrent low-flow alarms. Lab test showed slight anemia (11.8g/dl), thrombocytopenia (135G/l), elevated LDH (412U/l), elevated proBNP (2444pg/ml) and INR [2.3] and quick (30%) within the therapeutic range. CT angiography showed a high-grade stenosis of the outflow graft close to the ascending aorta (see Figure 1A, C). After admission the low-flow alarms became increasingly frequent and within 48 hours, the patient presented with a continuous LVAD flow of < 1>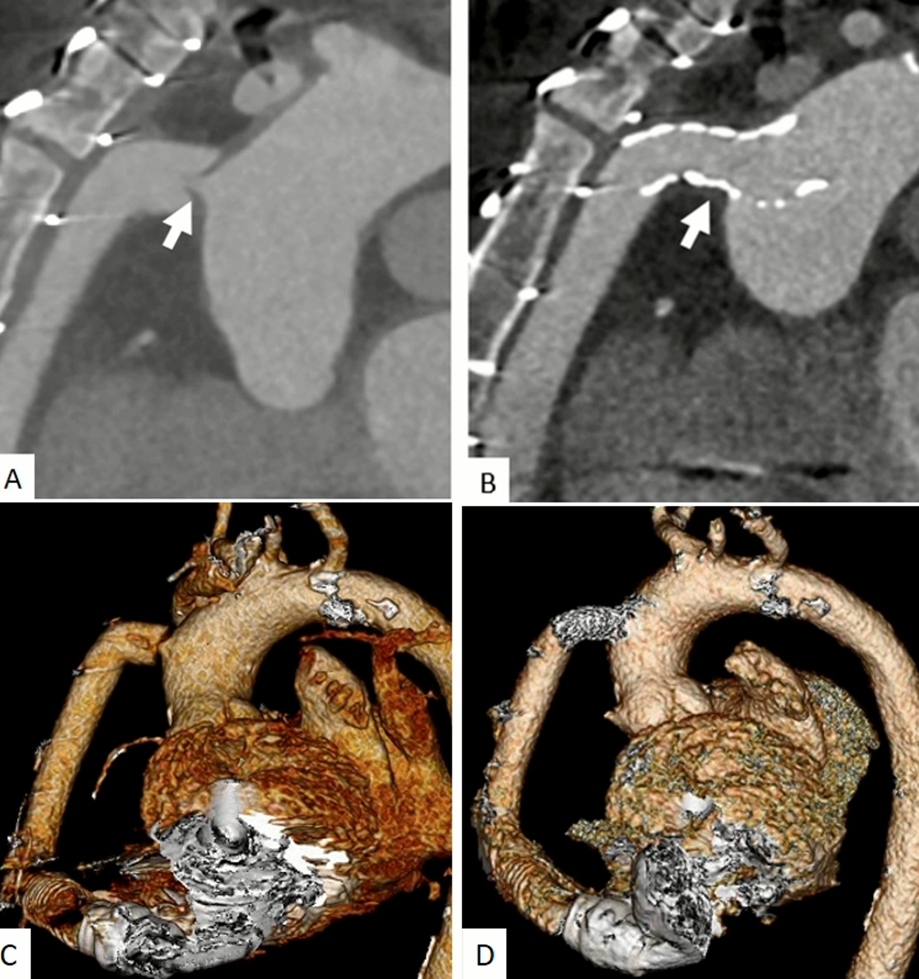
The intervention was performed under local anesthesia. Bilateral ultrasound guided percutaneous femoral access was performed. Through the left femoral artery, a 5Fr sheath was introduced and an angiographic catheter was placed into the ascending aorta. Through the right femoral artery, a 12Fr 80cm sheath was inserted and positioned. A Berenstein II catheter was used to cannulate the outflow graft and an Amplatz Extra Stiff guidewire was advanced for stability. The stenosis was passed with the 12Fr sheath and a 14x59mm BeGraft Aortic stent was deployed at position of the stenosis (see Figure 1B) and dilated with a 32mm Coda Balloon (Cook Medical) after stent implantation. An increase in LVAD flow up to 5 liters per minute, a stable power consumption of 3.5 Watts and speed of 5200rpm was observed immediately. The accesses were closed with a Proglide® Vascular Closure Device in standard fashion. The patient spent two days on the ICU for observation.
A final CT angiography after the intervention showed a patent outflow graft (see Figure 1B, D), and the patient was discharged 8 days later without any more alarms or changes in flow rate.
With the increasing adoption of endovascular techniques in clinical practice, they have become essential tools for addressing complex issues that would otherwise require high-risk and complicated surgical interventions.
The occurrence of pump thrombosis in HeartMate 3TM has been noted to be lower compared to HeartMate 2TM, but remains a significant concern. A comprehensive, multicenter study by Wert et al., involving 2108 patients from 17 centers, revealed an outflow graft stenosis incidence of up to 2.9%. These stenoses were attributed to factors such as twisting, kinking, or anastomosis stenosis due to suboptimal surgical techniques, but predominantly intraluminal thrombus formation caused by a gelatinous substance, or extraluminal compression. Similar to our observed case, approximately one-third of patients experienced low-flow alerts approximately 2-3 years post-implantation. In most cases, surgical intervention, removing the gelatinous coating responsible for the obstruction, was the treatment of choice, with only one-third of patients undergoing stenting or dilatation of the outflow graft [4].
It is important to note that we have observed two different types of outflow graft stenoses: dynamic and non-dynamic. In this case, the patient´s outflow graft stenosis was gradually worsening with a last significant drop of LVAD flow the night before the intervention. We have, however, seen other cases with dynamic, “valvular”-like components where the patients experienced differences in flow rates during the day. Therefore, it is highly important to treat after evaluating clinical signs, like reduction in LVAD flow and subsequently hypotension and symptoms like lightheadedness and dizziness, as seen in the patient described above.
Although a few different cases of outflow graft stenting have been described, little has been said about the type of stent used for the procedure. VICI VENOUS® or PALMAZ-SCHATZ® balloon-expandable stents have been mentioned previously because of their higher radial force, but not described in detail [5]. In our case, the new, off-label use of the BeGraft® aortic stent proved most successful because of the high radial force and post-dilation option.
We conclude with the recommendation that endovascular treatment of outflow graft stenosis is a safe and effective low-risk high-survival option in patients that are carefully evaluated. As a single case study, however, the findings may not be generalizable to broader patient populations and should be interpreted with caution. Further studies are necessary to validate these observations in larger cohorts.
Conceptualization: C.R, M.H., L.G. and C.M., data curation: M.H., L.G., C.H. and N.T., writing: C.R., C.F. and M.H., supervision: C.H, N.T. and C.M.. All authors have agreed to the published version.
N.P. declares a conflict of interest with Bentley Innomed, Hechingen, Germany regarding institutional grants and speaking fees. The other authors declare that they have no conflict of interest and that no funding supported this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
