
Research Article | DOI: https://doi.org/10.31579/2641-0419/379
1 University of Michigan Hospital, 1500 E Medical Center Dr, Ann Arbor, MI 48109
2 Stony Brook University Hospital, 101 Nicolls Rd, Stony Brook, NY 11794
*Corresponding Author: Mohammed Al-Sadawi, University of Michigan Hospital, 1500 E Medical Center Dr, Ann Arbor, MI 48109.
Citation: Mohammed Al-Sadawi, Michael Tao, Simrat Dhaliwal, Ravi Masson, William Lawson, et al, (2024), Timing of Coronary Angiography for Patients Without ST-Segment Elevation After Cardiac Arrest: A Systematic review and Meta-Analysis. J. Clinical Cardiology and Cardiovascular Interventions, 7(1); DOI:10.31579/2641-0419/379
Copyright: © 2024, Mohammed Al-Sadawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2023 | Accepted: 25 December 2023 | Published: 05 January 2024
Keywords: percutanmus translumiinal coronary angioplasty; coronary artery perforation; coronary artery rupture
Background/Aim: Although early coronary angiography (CAG) is currently recommended in patients with out of hospital cardiac arrest (OHCA) with ST segment elevation on electrocardiogram (EKG), the benefits in OHCA patients without ST segment elevation is unclear. The purpose of this meta-analysis is to evaluate the association between timing of CAG and clinical outcomes in patients with OHCA without ST segment elevation on EKG.
Methods: We performed a literature search for studies reporting an association between timing of CAG and study endpoints. The primary endpoint was all-cause mortality. The secondary endpoints neurological outcome and need for dialysis. The search included the following databases: Ovid MEDLINE, EMBASE, Web of Science, and Google Scholar. The search was not restricted to time or publication status.
Results: A total of 17 studies with 8118 participants (3447 with early CAG vs 4671 with late/no CAG) were included. The mean duration of follow-up was 138 days. Early CAG showed a trend toward reduction in all-cause mortality but this was not statistically significant (OR 0.83, 95% CI 0.60-1.14; p=0.25). Early CAG showed a trend toward favorable neurological outcome but this was not statistically significant (OR 0.75, 95% CI 0.48-1.18; p=0.21. Early CAG was not associated with increased risk for acute renal failure requiring hemodialysis (HD) (OR 1.0, 95% CI 0.73-1.38; p=0.99). Subgroup analysis by time to CAG demonstrated that early CAG was associated with increased all-cause mortality if performed immediately (OR 1.3, 95% CI 1.02-1.66; p=0.03), but decreased all-cause mortality if performed within 6 hours or within 24 hours (OR 0.73, 95% CI 0.58-0.90; p<0.01; OR 0.34, 95% CI 0.14-0.79; p=0.01).
Conclusions: Early CAG in patients presenting after OHCA without ST segment elevation may be beneficial compared to late/no CAG if performed after initial patient stabilization.
ACS : acute coronary syndrome
ARF : acute renal failure
CAG : coronary angiography
OHCA : Out-of-hospital cardiac arrest
STEMI : ST- elevation myocardial infarction
Out-of-hospital cardiac arrest (OHCA) is a global public health challenge, affecting approximately 3.8 million individuals annually [1]. Mortality rates are estimated to be greater than 50% and only 10% of patients are expected to experience favorable neurological outcomes [2, 3]. Acute coronary syndrome (ACS), specifically ST- elevation myocardial infarction, accounts for a large proportion of cases presenting as OHCA [4]. The occluded culprit lesion results in significant myocardial injury, which in turns leads to cardiac arrest, as well as increased risk of rearrest and adverse cardiovascular outcomes [5].
It is rationalized that alleviating the obstruction may assist in salvaging the myocardium and improve survival and outcomes. However, selection of optimal OHCA patients for revascularization to alleviate the obstructive lesion remains a contentious challenge. For years, early revascularization in STEMI patients is standard of care, representing Class I guidelines from the American Heart Association/American College of Cardiology [6]. Class IIa guidelines recommend coronary angiography (CAG) in patients without ST elevations without an obvious noncardiac etiology [6]. Nevertheless, the usefulness of revascularization in patients without ST elevations remains controversial as these patients are less likely to experience acute coronary artery lesions [7]. Thus, OHCA without ST elevations poses clinical and therapeutic challenges to physicians.
A direct comparison of early CAG in OHCA without ST elevations to outcomes may assist in clinical management. In this paper, we summarize the evidence linking a diagnosis of OHCA without ST elevations to all-cause mortality, neurologic recovery, and risk of acute renal failure (ARF). Moreover, we summarize the impact of immediate vs delayed CAG on all-cause mortality.
Data Search
This systematic review was performed in adherence to the guidelines of the PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-analyses). The review was performed using a preset protocol in December 2022. The primary endpoint was mortality. Secondary endpoints included Secondary endpoints included arrhythmias, neurological outcomes, and renal replacement therapy. We performed a database search for studies reporting on the association between timing of CAG and outcomes and safety endpoints in patients with non ST elevation cardiac arrest.
Search Strategy
A systematic search was conducted using Ovid MEDLINE, EMBASE, Scopus, Web of Science, and Google Scholar for relevant literature that reported the association between timing of CAG and outcomes and safety endpoints in patients with non ST elevation cardiac arrest. Two independent reviewers performed an electronic search using the following keywords: “early coronary angiography”, "coronary angiography", “outcomes”, “outcome”, “mortality”, and “Prediction”. The references of the screened studies, systematic reviews, review articles, and meta-analyses were manually reviewed for potential studies. After identifying relevant studies, the full texts of the selected articles were examined by both reviewers based on preplanned inclusion criteria. Disagreements were resolved by consensus.
Study Selection
Studies were selected using the PICO [8] (patient/population, intervention, comparison and outcomes) format to include those that studied patients with cardiac arrest with non-ST elevation myocardial infarction (Population), comparing early coronary angiography (Intervention) to delayed coronary angiography (Comparison), and assessing for all-cause mortality, arrhythmias, neurological outcomes, renal replacement therapy (Outcomes). Studies that did not separate ST elevation and non-ST elevation populations were excluded.
Data Extraction
Two reviewers (RM and MT) independently extracted the study data using a predefined data extraction sheet. Variables that were extracted from the studies included: Lead author, year of publication, study design, total patients on each group, risk factors, mean follow-up, mean age, and gender.
Statistical analysis
Meta-analysis was performed using Cochrane Review Manager (RevMan) software, version 5. We used a random-effects model to examine the association between strain imaging and outcomes, which were presented with an odds ratio (OR) with 95% confidence interval (CI). The extent of heterogeneity was determined by I2 (ranging from 0% to 100%). Statistical significance was considered with a P-value < 0.05 and all tests were 2-sided.
Literature Search and Study Selection
We identified 398 eligible studies from our literature search. After screening all studies, 28 eligible studies were selected for full text review. 17 studies were identified to be eligible for meta-analysis for the planned outcomes. Details of the selection process is presented in (Figure 1).
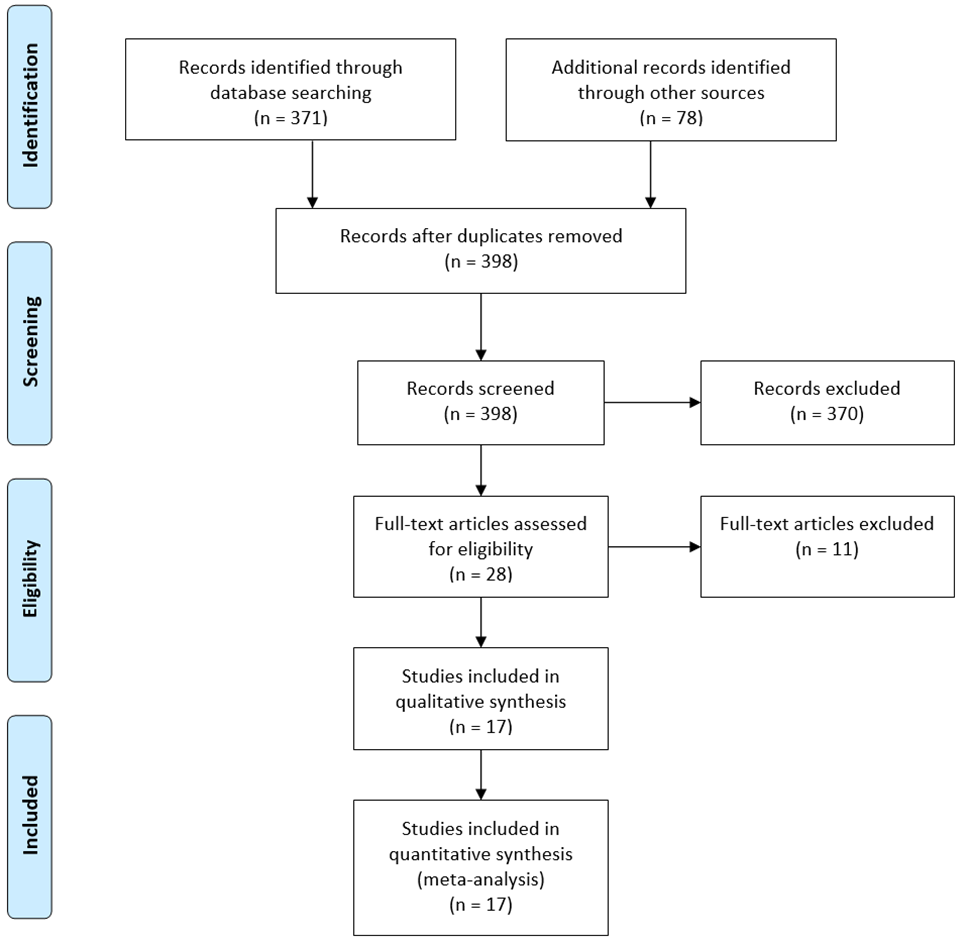
Figure 1: Prisma Flow Chart.
Flow diagram depicts study selection for inclusion in the meta-analysis according to the PRISMA statement for reporting systematic reviews and meta-analyses.
Study and Patient Characteristics
A total of 17 studies with 8118 participants (3447 with early CAG vs 4671 with late/no CAG) were included. The mean duration of follow-up was 138 days. Mean age was 62 years and 25% were females. Details of baseline demographic data is presented in (Table 1).
| Name | Year | Type | Follow-up (days) | Age (year) | Gender (%male) | Initial VT/VF | Initial PEA/asystole % | Early Total | Late Total | Late Total CAG | Early Time to CAG (Hours) | Late Time to CAG (Hours) |
| Bro-Jeppesen | 2012 | Pro | 30 | 61 | 80 | 184 | 60 | 82 | 162 | 57 | <12> | >12 |
| Hollenbeck | 2014 | Retro | 176 | 60 | 71 | 269 | 0 | 122 | 147 | 41 | <24> | >24 |
| Dankiewicz | 2015 | Pro | 426 | 66 | 79 | 409 | 135 | 252 | 292 | 94 | <6> | >6 |
| Kern | 2015 | Retro | X | 61 | 71 | 174 | 48 | 183 | 365 | 64 | <2> | >2 |
| Kleissner | 2015 | Pro | 180 | 58 | 79 | 73 | 26 | 25 | 74 | 31 | <2> | >2 |
| Garcia | 2016 | Pro | X | 55 | 77 | 303 | 0 | 130 | 73 | 32 | <6> | >6 |
| Patterson | 2017 | Pro | 30 | 61 | 86 | 36 | 0 | 18 | 18 | 14 | immediate | >48 |
| Shin | 2017 | Pro | X | 63 | 71 | 213 | 388 | 138 | 469 | 0 | <24> | X |
| Elfwen | 2018 | Retro | 30 | 66 | 79 | 799 | 0 | 275 | 524 | 166 | <24> | >24 |
| Elfwen | 2019 | Pro | 7 | 70 | 68 | 42 | 32 | 38 | 40 | 12 | Immediate | >24 |
| Kim | 2019 | Retro | 30 | 57 | 75 | 104 | 123 | 112 | 115 | 115 | Immediate | >2 |
| Lemkes | 2019 | Pro | 90 | 65 | 79 | 538 | 0 | 265 | 265 | 172 | <2> | >2 |
| Kern | 2020 | Pro | 180 | 65 | 79 | 75 | 23 | 49 | 50 | 24 | <2> | >6 |
| Desch | 2021 | Pro | 30 | 70 | 70 | 268 | 215 | 253 | 265 | 165 | Immediate | >24 |
| Song | 2021 | Pro | 180 | 59 | 73 | 339 | 339 | 231 | 447 | 104 | <6> | >6 |
| Hauw-Berlemont | 2022 | RCT | 180 | 65 | 70 | 88 | 183 | 126 | 138 | 74 | immediate | >48 |
| Janssens | 2022 | Retro | 360 | 63 | 70 | 1009 | 184 | 1148 | 1227 | 600 | <12> | >12 |
Early CAG showed a trend toward reduction in all-cause mortality but this was not statistically significant (OR 0.83, 95% CI 0.60-1.14; p=0.25) (Figure 2).
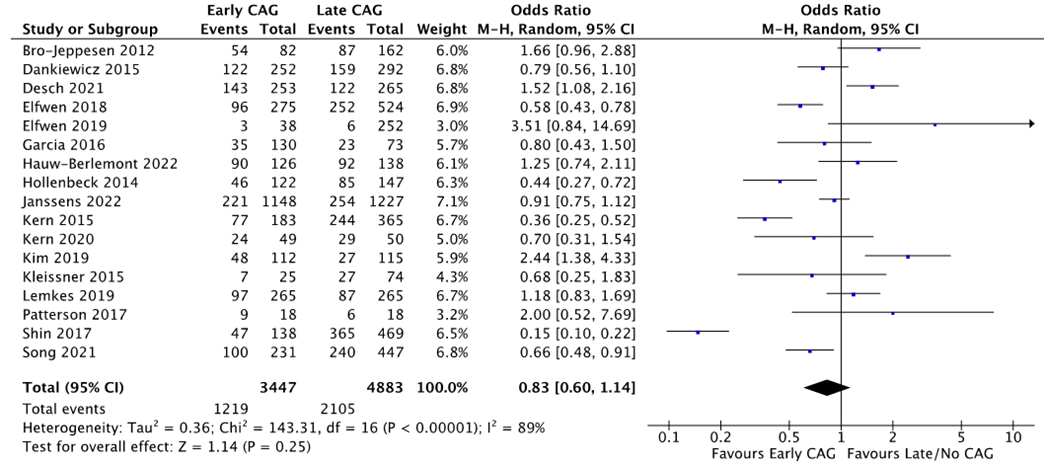
Figure 2: Association of Early vs Late/No CAG with All-Cause Mortality
Early CAG showed a trend toward favorable neurological outcome but this was not statistically significant (OR 0.75, 95% CI 0.48-1.18; p=0.21) (Figure 3).
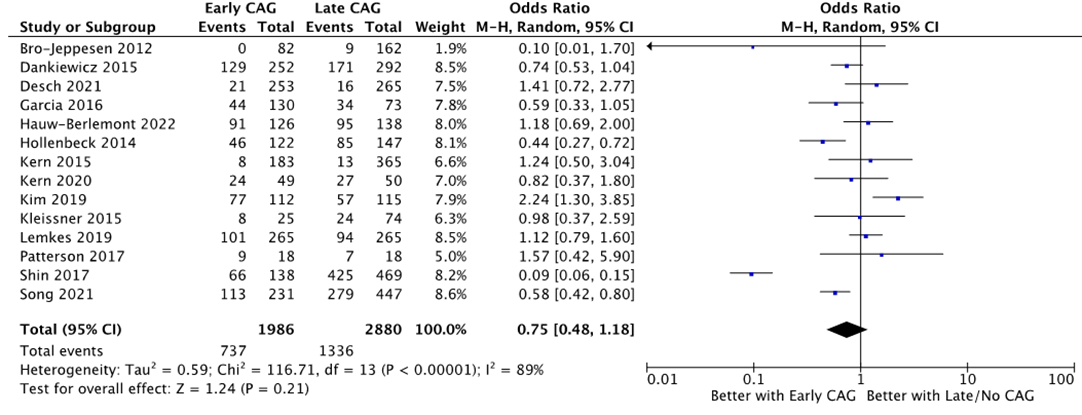
Figure 3: Association of Early vs Late/No CAG with Neurological Outcome
Early CAG was not associated with increased risk for acute renal failure requiring hemodialysis (HD) (OR 1.0, 95% CI 0.73-1.38; p=0.99). (Figure 4)
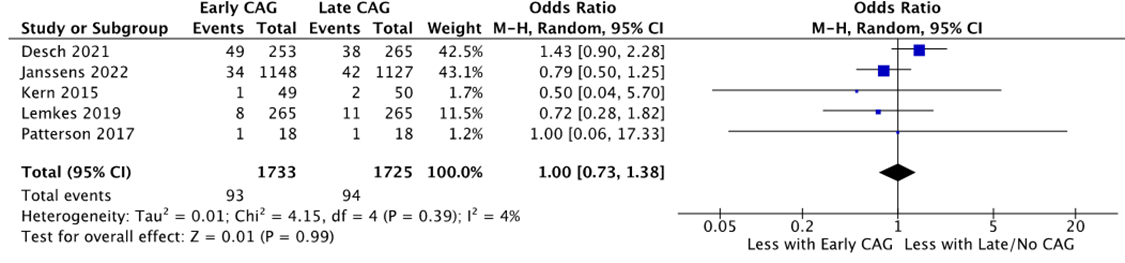
Figure 4: Association of Early vs Late/No CAG with Need for HD
Subgroup analysis by time to CAG demonstrated that early CAG was associated with increased all-cause mortality if performed immediately (OR 1.3, 95% CI 1.02-1.66; p=0.03), but decreased all-cause mortality if performed within 6 hours or within 24 hours (OR 0.73, 95% CI 0.58-0.90; p<0 p=0.01)>

Figure 5: Subanalysis to test association Between Immediate CAG and All-Cause Mortality, CAG < 6>
This systematic review and meta-analysis evaluated the role of CAG, in patients with OHCA without ST elevations, on outcomes. We found early CAG is associated with a trend toward reduction in all-cause mortality and favorable neurological outcomes, however, immediate CAG is associated with increased risk of all-cause mortality, which is in drastic contrast to delaying CAG to 6-24 hours.
Acute coronary artery occlusion remains the leading cause of OHCA, representing 70-80% of cases [9, 10]. However, in patients presenting in cardiac arrest without ST elevations, the beneficial role of CAG is conflicting. The results of our study supported the findings in the largest randomized trial, to date, evaluating this topic, Coronary Angiography After Cardiac Arrest (COACT) trial, which neither demonstrated significant improvements in morality, nor safety concerns, such as ARF, for early angiography [11]. These results may partially be explained by OHCA patients without ST elevations are less likely to experience significantly obstructive coronary lesions. Given these irregular, non-significant stenotic lesions, it is more difficult to achieve successful outcomes with CAG because TIMI blood flow is not drastically affected, and CAG does not successfully salvage at-risk myocardium [12].
Another potential explanation for the lack of significance seen with regards to outcomes, especially favorable neurologic recovery, is post-cardiac arrest syndrome. Post cardiac arrest syndrome is classified as multiorgan failure as a result of ischemic reperfusion injury, which drastically affects the brain, resulting in neurologic injury. Death from neurologic injury in OHCA patients is three times more likely than from a cardiac etiology [11, 13]. Thus, it is possible a trend towards, but not significant, neurologic improvement was seen in CAG patients because most patients died from neurologic complications and were excluded from statistical analysis.
Moreover, cardiac arrest is marked by decreased cardiac output and elevated afterload, both of which may contribute to hypotension, vasoconstriction of afferent arterioles, and ultimately decreased renal perfusion. OHCA patients often require vasopressors to maintain a blood pressure that is compatible with life, which results in further vasoconstriction. This vicious cycle is perpetuated which likely leads to a progressive decline in renal function. ARF has been closely linked to the intensity of ischemia–reperfusion injury after OHCA [14-17]. Thus, CAG may not result in an increased risk of ARF requiring HD because OHCA patients are already at a baseline risk for ARF given the adverse event. On the other hand, immediate CAG was significantly associated with increased all-cause mortality, while delaying a CAG to 6-24 hours was associated with a reduction in all-cause mortality. This is likely secondary to optimization of hemodynamics. Hypotension, as stated above, is poorly tolerated in OHCA patients because of the reduction in organ perfusion [18]. Gaieski et al explored the benefits of early hemodynamic stabilization post-cardiac arrest with titration of fluids, vasopressors, and mechanical support [19]. Their study was underpowered and unable to evaluate survival benefits; however, they emphasized the importance of further assessing benefits of patient stabilization prior to intervention.
This issue was discussed in other meta-analyses, Abusnina et al. [20] reviewed 6 randomised controlled trials for patients wih OHCA and reported that early CAG is not associated with reduced 30-day mortality when compared to patients who underwent delayed CAG.We discussed that in our work as most of these trial did CAG within the first 6 hours which showed no benefits, however, we showed that doing it afterwards was assocoiated with better outcomes that delayed approach.
Our review has several limitations. First, the studies experienced significant heterogenicity, especially regarding all-cause mortality and neurologic outcomes. Secondly, not all studies specified the degree of obstruction seen on CAG, which made it difficult to distinguish results based on obstructive vs nonobstructive coronary artery disease, Third, only a few studies distinguished the type of mortality. Fourth, our study was limited to all-cause mortality, neurologic recovery and ARF; however, future studies may benefit by focusing on quality of life and other cardiovascular outcomes post-OHCA.
Our present systematic review and meta-analysis has important clinical implications. OHCA patients without ST elevations who undergo CAG experience a trend toward, but not significant, reduction in all-cause mortality and improvement in neurologic outcomes without an increased risk of ARF requiring HD. This is likely due to these patients experiencing nonobstructive coronary artery lesions which do not benefit from revascularization. Despite the encouraging results of this recent meta-analysis, several questions regarding this form of therapy remain unanswered, particularly the effect of early mechanical support in addition to CAG. We require more evidence before we can extend these findings (and recommendations) to patients.
Our review has several limitations. First, the studies experienced significant heterogenicity, especially regarding all-cause mortality and neurologic outcomes. Secondly, not all studies specified the degree of obstruction seen on CAG, which made it difficult to distinguish results based on obstructive vs nonobstructive coronary artery disease, Third, only a few studies distinguished the type of mortality. Fourth, our study was limited to all-cause mortality, neurologic recovery and ARF; however, future studies may benefit by focusing on quality of life and other cardiovascular outcomes post-OHCA.
None
The authors report no relevant conflicts of interest.
The systematic review was conducted with a protocol in accordance with the Preferred Reporting of Items for Systematic reviews and Meta-Analyses (PRISMA) statement.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
