
Case Report | DOI: https://doi.org/10.31579/2690-4861/051
*Corresponding Author: Pankaj Bansal, Mayo Clinic Health System. 1400 Bellinger Street, Eau Claire, WI.
Citation: Austin C, Pankaj B, Bhavin S, Amandeep G. (2020) Timeline of COVID-19 and its therapeutics in the United States. International Journal of Clinical Case Reports and Reviews. 3(3); DOI: 10.31579/2690-4861/051
Copyright: © 2020 Pankaj Bansal, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 August 2020 | Accepted: 04 September 2020 | Published: 07 September 2020
Keywords: covid-19, United States
The novel coronavirus was first discovered and reported in December 2019. Later termed the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-COv-2) virus, rapid spread was detected in China. Overtime, SARS-COv-2 spread to various other countries requiring swift intervention on a global scale. As infection spread, several therapeutics have been investigated for Coronavirus Disease- 2019 (COVID-19), including remdesivir, lopinavir/ritonavir, hydroxychloroquine, dexamethasone, etc. Furthermore, rapid investigation and construction of several potential vaccines have begun, some of which are in late stage testing. We present a concise timeline representing the evolution of COVID-19, therapeutic trials, and vaccine development. Ultimately, evident by the overall poor efficacy of several medications investigated so far, vaccination success remains the most likely effective step to combat COVID-19.
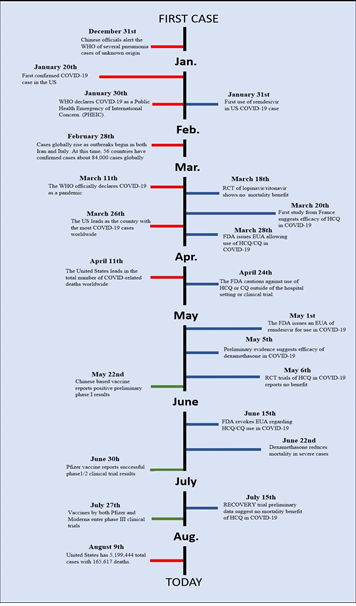
The world is going through unprecedented times as the novel Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) virus has continued its spread globally. It was in December 2019 that China alerted the World Health Organization (WHO) of a cluster of cases of pneumonia of unknown origin in the Wuhan in Hubei province [1]. While it was initially postulated that the human-to-human transmission may not exist, within a few days, the WHO confirmed the human-to-human transmission of the virus. Thailand reported the first imported case outside China on January 13th, 2020. On January 20th, the first case of 2019 novel coronavirus (2019-nCoV) was reported in the United States [2]. By January 30th, China had reported more than 9,000 cases with more than 200 deaths, and cases were reported from several other countries including Thailand, Japan, Taiwan, Singapore, Vietnam, Nepal, Finland, Italy, South Korea, India, Australia, France, Malaysia, and Canada [1]. It was on January 30th that the WHO declared the 2019-nCoV as a public health emergency of international concern [1].
The first mortality in the United States was reported on February 6th, 2020 from California [3]. On February 11 2020, the WHO announced the formal name Coronavirus Disease- 2019 (COVID-19) [4]. While the initial caseload and deaths were mostly in China, by the end of February 2020, Iran and European countries including Italy and France started reporting rising numbers of cases and deaths from COVID-19. By March 1st, most cases in the United States were from Washington State, and new cases were being reported from other states including New York. On March 11th, the WHO declared COVID-19 a pandemic and on March 13th, the United States declared the pandemic to be a national emergency [1].
The caseload in the United States crossed 100 on March 3rd 2020, and by March 19th 2020, the cases had surpassed 10,000 and on March 26th 2020, the United States overtook China to become the country with the most number of cases worldwide with more than 86,000 cases. It took less than a week to surpass 200,000 cases in the United States, and most of the cases were being reported from the New York area. On April 11th, 2020, with more than 19,000 deaths reported, the United States became the country with most deaths worldwide and by the end of April 2020, there were more than 1 million cases of COVID-19 in the United States [1]. This number steadily climbed in the United States and world eventually reaching 1,507,773 cases and 90,113 deaths in the United States, and 4,722,319 cases and 313,268 deaths worldwide by May 17th 2020 [5, 6]. Since April 2020, the United States has been the world leader in both the number of cases, as well as the number of deaths.5 As of August 5th 2020, when comparing the case-fatality ratios, the United States places 24 with the United Kingdom taking the lead. When investigating per capita death rates, the United States places ninth with Belgium placing first [7]. As of August 9th, the United States had 5,199,444 total cases with 165,617 deaths (Figure 1) [8, 9].
To date, there is no definitely proven effective therapeutic option for COVID-19. Initial attempts by scientists across the world have focused on finding therapeutic options already approved for another indication, and antiviral agents including lopinavir/ritonavir gained popularity owing to the in vitro efficacy against the Sudden Acute Respiratory Syndrome Coronavirus (SARS-CoV) and potential efficacy shown previously against Middle Eastern Respiratory Syndrome Coronavirus (MERS-CoV) and Sudden Acute Respiratory Syndrome (SARS). However, further clinical trials failed to show any efficacy of lopinavir/ritonavir in COVID-19 [10, 11]
Similarly, antimalarial agents including chloroquine and hydroxychloroquine were one of the initial agents that gained interest as a therapeutic option after data from in-vitro studies and a cohort study from France showed potential antiviral efficacy [12]. The President of the United States in a press release famously cited this study [13], and antimalarial agents gained fame as potential game-changers. However, more well-performed studies and randomized controlled clinical trials soon followed and did not show any benefit of chloroquine or hydroxychloroquine in COVID-19, and the FDA retracted the emergency authorization for use of hydroxychloroquine in COVID-19 in June 2020 [11, 14-16]
One of the antiviral agents that has shown promise is remdesivir, a broad-spectrum antiviral agent. While initially developed for the treatment of hepatitis C, remdesivir has shown activity against SARS and MERS in past in vitro assays [17, 18]. This sparked investigation for a possible role in COVID-19. This medication was used on the first known COVID-19 case of the United States.19 After successful evidence showing moderate benefit especially in shortening the length of hospital stay in patients admitted with COVID-19, the FDA issued an emergency use authorization for remdesivir. It is currently the only drug still granted this approval for use in COVID-19 [17, 20-22].
COVID-19 is associated with excessive uncontrolled release of proinflammatory cytokines in severe cases, and several anti-inflammatory and immunomodulatory agents have been investigated, with trials ongoing on others. Data from the Rheumatology COVID registry revealed that patients who are already on moderate to high doses of corticosteroids have a higher risk of more severe COVID-19 infection [23, 24]. However, when used in more severe cases already needing oxygen, dexamethasone was shown to reduce mortality [25, 26]. Initial and preliminary data on other anti-inflammatory and immunomodulatory agents including interleukin-6 and interleukin-1 inhibitors (tocilizumab and anakinra respectively) have shown promising results, with further trials ongoing. Sarilumab, another interleukin-6 inhibitor did not show any benefit in COVID-19, while trials on colchicine, baricitinib, and anti-tumor necrosis factor medications are ongoing [27-29].
With no definite therapeutic agent still available, the hopes to overcome the pandemic rely mostly on a safe and effective vaccine. The goal of vaccination is to stimulate a protective immune response using viral genetics, proteins, or entire inactivated virions. Initial investigation of vaccines began rapidly, and several pharmaceutical companies have reached various stages of clinical trials by now. Many vaccine candidates have been established in all various roles described. Notably, Chinese based vaccines demonstrated a positive preliminary phase 1 results as early as May 22nd. Other vaccines followed closely with their own successful preliminary positive results. At this time, few vaccine candidates have entered phase III clinical trials [30-35]. possible viral mutations could interfere with the overall effectiveness of future vaccines, and further ongoing research about the viral evolution will be critical to investigate this complicating factor [36].
The United States-based Moderna vaccine that is mRNA based entered phase III in July 2020. Another mRNA based vaccine from the United States-based Pfizer/BioNTech has reached Phase II/III. China-based Sinopharm and Sinovac biotech have entered phase III with their vaccines using attenuated whole-virus inoculation, while the China based CanSinoBio and AstraZeneca have entered phase III with their viral vector based vaccines [30-35]. It may not be until 2021 that an effective and safe vaccine may be available for widespread use, and with no definite therapeutic option available. To date, the only way to mitigate the virus is by prevention precautions and social distancing.
Conclusion
Currently, no medications have sufficiently stood out as an outstanding therapeutic option for COVID-19, and trials on several potential vaccine candidates are ongoing worldwide, with a hope for a successful vaccine available for widespread use by 2021. Implementing prevention precautions remains as the primary method for limiting the spread of SARS-CoV-2.
Author contributions
All authors have made substantial contributions to the creation of this manuscript including writing the initial manuscript, literature review, and reviewing, and revising the final version. The final manuscript has been reviewed and approved by all authors.
Financial disclosure and conflict of interest statement
We confirm that the authors have no financial disclosures, competing interests, and conflict of interest. The study has not received any financial support or other benefits from commercial sources for the work reported on in the manuscript. The manuscript represents the original work of the authors and identical or similar work has not been published or submitted for publication elsewhere.
Data sharing statement
There is no data in this work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
