
Research Article | DOI: https://doi.org/10.31579/2641-0419/259
1 Department of Cardiology, 981 Hospital of Joint Logistics Support Force, Chengde, Hebei 067000, P. R. China.
2 Department of Cardiology, Xijing Hospital, Airforce Military Medical University, Xi'an, Shaanxi 710032, P. R. China.
3 Department of Health Statistics, The Airforce Military Medical University, Xi'an, Shaanxi 710032, P. R. China.
4 Department of Cardiology, The First Affiliated Hospital of Xi'an Medical University, Xi'an, Shannxi 710077, P. R. China.
5 Department of Cardiology, No.971 Hospital of the PLA Navy, Qingdao, Shandong 266071, P. R. China.
6 Cadet Brigade, School of Basic Medicine, Airforce Military Medical University, Xi'an, Shannxi 710032, P.R. China.
Department of Naval Medicine, Naval Medical University, Shanghai 200433, P. R. China.
8 Department of Pharmacogenomics, The Airforce Military Medical University, Xi'an, Shaanxi 710032, P. R. China.
9 Department of Cardiology, Hanyin County People's Hospital, Ankang, Shaanxi 725100, P. R. China
10 School of Basic Medicine, Airforce Military Medical University, Xi'an, Shannxi 710032, P.R. China.
#Peng Han, Ying Liang, and Suining Xu contributed equally to this work.
*Corresponding Author: Kun Lian, Xijing Hospital, Airforce Military Medical University, China, Chengxiang Li, Xijing Hospital, Airforce Military Medical University, China and Qingyi Wang, School of Basic Medicine, Airforce Military Medical University, China.
Citation: Peng Han, Ying Liang, Suining Xu, Shuai Zhao, Yan Chen. et all (2022). Ticagrelor Versus Clopidogrel in the treatment of Elderly Chinese Chronic Total Occlusion Patients Undergoing Percutaneous Coronary Intervention. J. Clinical Cardiology and Cardiovascular Interventions, 5(4); DOI:10.31579/2641-0419/259
Copyright: © 2022 Kun Lian, Chengxiang Li and Qingyi Wang, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 March 2022 | Accepted: 14 March 2022 | Published: 21 March 2022
Keywords: ticagrelor; clopidogrel; aged cto patients; percutaneous coronary intervention; chronic total occlusion
Background: Taking thrombosis and bleeding risks into consideration, little real world study data is available to dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) in elderly Chinese chronic total occlusion (CTO) patients.
Objective: This study was designed to investigate the effectiveness and safety of Ticagrelor in comparison with Clopidogrel as an add-on therapy to Aspirin for elderly Chinese CTO patients who underwent elective PCI.
Materials and Methods: We retrospectively enrolled 504 CTO patients (aged ≥75 years) who received PCI from December 2009 to May 2020 and DAPT for up to 12 months. The effectiveness endpoints were evaluated by major adverse cardiac events (MACE) including all-cause death, nonfatal myocardial infarction (MI) and clinically driven revascularization. The safety endpoints were recorded as the incidence of Bleeding Academic Research Consortium (BARC) bleeding.
Results: Patients in Clopidogrel group, as was evidenced in our study, were older, and had a higher percentage of BMI, diastolic blood pressure and HDL-C than those in Ticagrelor group. Clopidogrel group had a lower percentage of hyperlipidemia, prior PCI, glucose, TG and LDL-C. No significant difference was found as to the Angiographic and procedural characteristics (P>0.05 for all). After 12 months' follow-up, the incidence of MACE (12.19% vs. 11.04%, P=0.763) and bleeding (9.38% vs. 13.64%, P=0.205) showed no significant difference. After clinical characteristics balanced matching by inverse probability of treatment weighting (IPTW) model, we found that Ticagrelor had an unfavorable effect on reducing the incidence of bleeding with the IPTW model (IPTW-OR, 1.81, 95% CI: 1.18-2.76, P=0.006).
Conclusions: Clopidogrel and Ticagrelor present similar effectiveness and safety to elderly Chinese CTO-PCI patients, yet Ticagrelor should be prescribed with caution to patients with a high bleeding risk.
Coronary chronic total occlusion (CTO) is observed in approximately 15-25% of coronary artery disease (CAD) patients who underwent prior coronary angiography [1,2]. Guidelines recommend selective percutaneous coronary intervention (PCI) to CTO patients to improve their symptoms and quality of life, as well as survival rates [3,4]. Intensive dual antiplatelet therapy (DAPT) is recommended for CTO-PCI patients to reduce potential thrombosis induced by complex lesions and frequent stent placement of CTO [5,6]. Tough continuous antiplatelet therapy is also associated with increased bleeding, more concern is given for delivering DAPT medication to elderly CTO-PCI patients to balance bleeding and ischemia, as the elderly population over 75 years has a much higher risk of bleeding. Nevertheless, given that traditional clinical randomized controlled trials seldom had elderly CTO patients as their subjects, data on elderly CTO-PCI patients’ DAPT is scarcely available.
As the most commonly used DAPT drugs, Ticagrelor has faster action and stronger antiplatelet effect, and its effect is reversible compared with Clopidogrel [7]. Chinese CTO-PCI patients were reportedly showed lower MACE incidence and higher bleeding incidence after receiving normal dose of Ticagrelor, compared with Clopidogrel in Chinese CTO-PCI patients [8],. Unfortunately, no data concerning the elderly patients was found.
Considering the profound potential value of identifying how different DAPT strategies affect elderly CTO-PCI patients, this study was designed to investigate the effectiveness and safety of Ticagrelor in comparison with Clopidogrel as an add-on therapy to Aspirin for elderly Chinese CTO patients who received PCI.
Study design
This study was conducted in the Department of Cardiology, Xijing Hospital from December 2009 to May 2020 and aimed to compare the effectiveness and safety of Ticagrelor versus Clopidogrel in elderly Chinese CTO patients who underwent elective PCI with drug-eluting stents (DES). PCI success was assessed by the interventional cardiologist performing the procedure. The study protocol was approved by the Ethics Committee of Air Force Medical University (KY20172019-1). Written informed consents were obtained from all participants.
Study participants
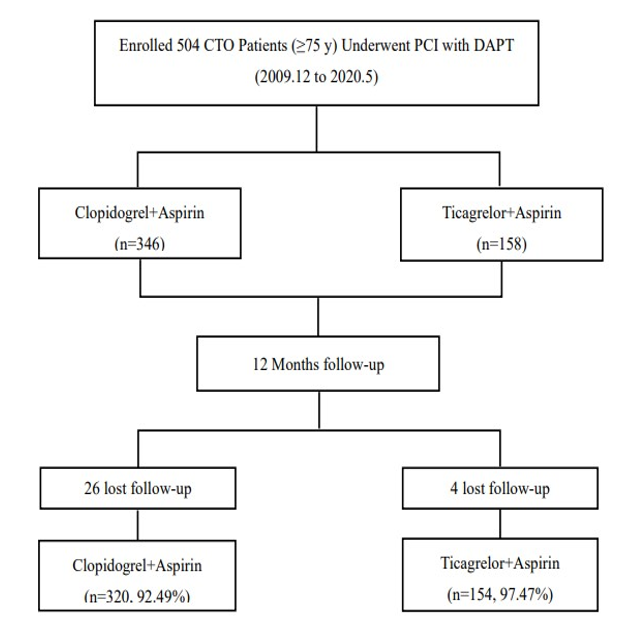
From December 2009 to May 2020, a total of 504 CTO patients who successfully underwent elective PCI were prescribed DAPT for up to 12 months, and were retrospectively enrolled in the study. Among the 504 patients, with 30 lost in follow-up, eventually 474 patients were included in this study. These patients were initiated on DAPT prior to PCI, among whom 320 took Clopidogrel with a 300mg loading dose followed by a dose of 75 mg daily, while the other 154 patients took Ticagrelor with a loading dose of 180 mg followed by a dose of 90 mg twice daily. All the patients took Aspirin at a dose of 100 mg daily. Inclusion criteria included: 1) were aged ≥75 years old; 2) validated with CTO by coronary angiography; 3) received PCI successfully; 4) signed the informed consent. Exclusion criteria included: 1) underwent conservative oral anticoagulation therapy; 2) exhibited PCI contraindications; 3) displayed P2Y12 inhibitors contraindications; 4) with high risk of bleeding diathesis or coagulation disorder; 5) diagnosed with dialysis-dependent renal failure or liver cirrhosis; 6) refused to participate in this study by the patient. Clinical baseline, angiographic and procedural data were collected and recorded.
Study endpoints and definitions
Clinical follow-up was carried out by telephone interviews and outpatient visits. The follow-up period started from the date of DAPT use after PCI and ended when any study outcome first occurred or at 12 months after PCI. Inpatient observation and outpatient visits were scheduled for patients being regularly followed up in our hospital, while telephone calls were made for patients without regular medical follow-up. The incidence of end points was collected in medical records by a predefined questionnaire, in which health status, physical examinations, vital signs as well as laboratory assessments were simultaneously recorded. The effectiveness endpoints in this study were evaluated by the occurrence of MACE, i.e., the composite of all-cause death, nonfatal MI and clinically driven revascularization. All-cause death was defined as death from any cause, which was ascertained without adjudication [9].
CTO was defined as angiographic evidence of total occlusion with complete interruption of anterograde blood flow (Thrombolysis In Myocardial Infarction (TIMI) flow grade 0) with an estimated duration of>3 months via previous angiograms, angina symptoms and a history of MI [2]. Coronary arteries measured were proximal left main artery (LM), left anterior descending artery (LAD), left circumflex artery (LCX) and right coronary artery (RCA). The diagnosis of MI was based on the Fourth Universal Definition of MI [10]. Clinically driven revascularization was defined as any reintervention because of symptoms [11]. The safety endpoints were evaluated by the incidence of bleeding: Bleeding Academic Research Consortium (BARC) type 1, 2, 3, or 5 [12]. Type 1 is inactive bleeding. Type 2 is active bleeding requiring evaluation or intervention by medical personnel, which differs from Type 3, Type 5 and bleeding related to coronary artery bypass graft. Type 3 is heavy bleeding as well as intracranial bleeding with significant hemoglobin reduction to 5g/dl, which requires blood transfusion. For Type 5, it refers to potential or qualitative fatal bleeding. The major bleeding events, which are the equivalent of BARC 3 and 5, include gastrointestinal bleeding, intracranial hemorrhage, hemoglobin decrease of ≥3 g/dL, significant bleeding requiring blood transfusion, and fatal bleeding [13].
Statistical analysis
This is a single-center, retrospective cohort study. Continuous variable was described as mean ± SD or median and interquartile spacing, and categorical variable as number (percentage). Differences in continuous and categorical variables between groups were analyzed with Mann–Whitney U-test and Chi-square test respectively, and P< 0>
Clinical baseline, angiographic and procedural baseline characteristics
In this study, a total of 504 CTO patients (≥75 years) were prescribed with DAPT for 12 months after PCI from December 2009 to May 2020. During this period of time (12 months after PCI), 30 patients were lost to follow-up, and in the end 474 CTO patients were included in the study (Figure 1).
In terms of clinical baseline characteristics, compared with the patients in Ticagrelor group, those in Clopidogrel group were older (80.45±4.23 vs. 79.18±3.59, P=0.001) and had a higher percentage of BMI (24.14±3.49 vs. 22.82±4.75, P=0.003), more elevated diastolic blood pressure (74.53±10.16 vs. 71.82±9.85, P=0.007) and higher HDL-C (1.92±0.87 vs. 1.05±0.29, P<0>P<0> P=0.003), and they had lower glucose (24.14±3.49 vs. 22.82±4.75, P=0.003), TG (1.31±0.78 vs. 1.48±0.85, P=0.037) and LDL-C (1.22±0.71 vs. 1.96±0.75, P<0>P>0.05 for all) (Table 1).
| Variable | Clopidogrel (n=320) | Ticagrelor (n=154) | P value |
|---|---|---|---|
| Age, years | 80.45±4.23 | 79.18±3.59 | 0.001 |
| Male, % | 230 (71.88) | 115 (74.68) | 0.582 |
| BMI | 24.14±3.49 | 22.82±4.75 | 0.003 |
| Heart rate, beats/min | 73.15 ±12.33 | 72.24±10.74 | 0.437 |
| SBP, mmHg | 130.02±22.71 | 128.39±25.38 | 0.487 |
| DBP, mmHg | 74.53±10.16 | 71.82±9.85 | 0.007 |
| Smoking, % | 87 (27.19) | 33 (21.43) | 0.215 |
| Medical history | |||
| Hypertension, % | 192 (60.00) | 85 (55.19) | 0.322 |
| Diabetes mellitus, % | 90 (28.13) | 48 (31.17) | 0.518 |
| Hyperlipidemia | 72(22.50) | 67 (43.51) | <0> |
| Valvular heart disease, % | 2 (0.63) | 0 | 1.000 |
| Atrial fibrillation, % | 12 (375) | 4 (2.60) | 0.598 |
| Stroke, % | 33 (10.31) | 19 (12.34) | 0.532 |
| Chronic kidney diseases, % | 8 (2.50) | 8 (5.19) | 0.172 |
| Peripheral arterial disease, % | 2 (0.63) | 0 | 1.000 |
| Family history of CAD, % | 0 | 2 (1.30) | 0.105 |
| Prior MI, % | 15 (4.69) | 10 (6.49) | 0.511 |
| Prior PCI, % | 82 (25.63) | 61 (39.61) | 0.003 |
| Prior CABG, % | 8 (2.50) | 2 (1.30) | 0. 511 |
| Laboratory data before PCI | |||
| WBC (109/L) | 6.65±2.19 | 6.87±3.79 | 0.420 |
| RBC (1012/L) | 4.24±0.61 | 4.24±0.53 | 0.946 |
| Hb (g/L) | 131.19±18.45 | 129.87±17.01 | 0.457 |
| PLT (109/L) | 177.32±67.05 | 189.04±60.24 | 0.066 |
| Creatinine (μmol/L) | 108.20±52.01 | 114.93±82.86 | 0.288 |
| Ccr (ml/min) | 49.09±13.88 | 46.40±13.54 | 0.104 |
| BUN (mmol/L) | 5.89±2.20 | 6.06±1.97 | 0.655 |
| UA (μmol/L) | 311.00±289.95 | 313.27±89.20 | 0.930 |
| ALT (U/L) | 20.00 (16.75) | 21.00 (11.00) | 0.578 |
| AST (U/L) | 20.00 (13.00) | 16.00 (12.85) | 0.177 |
| Alb (g/L) | 38.49±4.99 | 37.96±3.94 | 0.363 |
| Glu (mmol/L) | 6.19±2.42 | 6.97±3.04 | 0.007 |
| TC (mmol/L) | 3.64±1.07 | 3.52±0.89 | 0.236 |
| TG (mmol/L) | 1.31±0.78 | 1.48±0.85 | 0.037 |
| LDL-C(mmol/L) | 1.22±0.71 | 1.96±0.75 | <0> |
| HDL-C(mmol/L) | 1.92±0.87 | 1.05±0.29 | <0> |
| NT-proBNP (pg/ml) | 598.30 (1415.98) | 661.50 (2065.50) | 0.229 |
| LVEF (%) | 52.17±9.36 | 51.12±9.29 | 0.303 |
Abbreviations: CAD, coronary artery disease; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; BMI, Body Mass Index; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cell; RBC, red blood cell; Hb, Hemoglobin; PLT, blood platelet; Ccr, creatinine clearance; BUN, blood urea nitrogen; UA, uric acid; ALT, alanine amiotransferase; AST, aspartate aminotransferase; Alb, albumin; Glu, Glucose; TC, triglyceride; TG, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction.
Table 1: Clinical baseline characteristics (n=474)
For CTO lesion characteristics, no significant differences were found as to the CTO lesions of coronary arteries (LM, LAD, RCA, and LCX), number of treated vessels, number of stents or total stent length (P>0.05 for all) (Table 2).
| Variable | Clopidogrel (n=320) | Ticagrelor (n=154) | P value |
|---|---|---|---|
| CTO Lesion characteristics, % | |||
| LM | 2 (0.63) | 0 | 1.000 |
| RCA | 149 (46.56) | 76 (49.35) | 0.624 |
| LAD | 158 (49.38) | 71 (46.10) | 0.556 |
| LCX | 96 (30.00) | 53 (34.42) | 0.343 |
| Number of treated CTO vessels, % | |||
| 1 | 308 (96.25) | 144 (93.51) | 0.242 |
| 2 | 12 (3.75) | 9 (5.84) | 0.342 |
| 3 | 0 | 1 (0.65) | 0.325 |
| Number of stents | 2.42±1.16 | 2.40±1.15 | 0.842 |
| Total stent length, mm | 61.13±34.18 | 61.36±36.55 | 0.948 |
Abbreviations: CTO, chronic total occlusion; LM, left main; LAD, left anterior descending; RCA, right coronary artery; LCX, left circumflex.
Table 2. Angiographic and procedural characteristics
Clinical outcomes on follow-up
After 12 months’ follow-up, the incidence of MACE was 12.19% in Clopidogrel group and 11.04% in Ticagrelor group (P>0.05), the individual components in the two groups were not significantly different either. The total bleeding rate (9.38% vs. 13.64%) and BARC 1 bleeding (8.13% vs. 12.99%) of Clopidogrel group were lower than those of Ticagrelor group, but with no statistical significance (P>0.05) (Table 3).
| Variable | Clopidogrel (n=320) | Ticagrelor (n=154) | P value |
|---|---|---|---|
| MACE, % | 39 (12.19) | 17 (11.04) | 0.763 |
| All-cause death, % | 35 (10.94) | 17 (11.04) | 1.000 |
| Nonfatal myocardial infarction, % | 1 (0.31) | 2 (1.30) | 0.248 |
| Clinically driven revascularization, % | 3 (0.94) | 0 | 0.554 |
| Bleeding, % | 30 (9.38) | 21 (13.64) | 0.205 |
| BARC 1, % | 26 (8.13) | 20 (12.99) | 0.100 |
| BARC 2, % | 2 (0.63) | 0 | 1.000 |
| BARC 3, % | 0 | 0 | |
| BARC 5, % | 2 (0.63) | 1 (0.65) | 1.000 |
Table 3: Efficacy and safety points
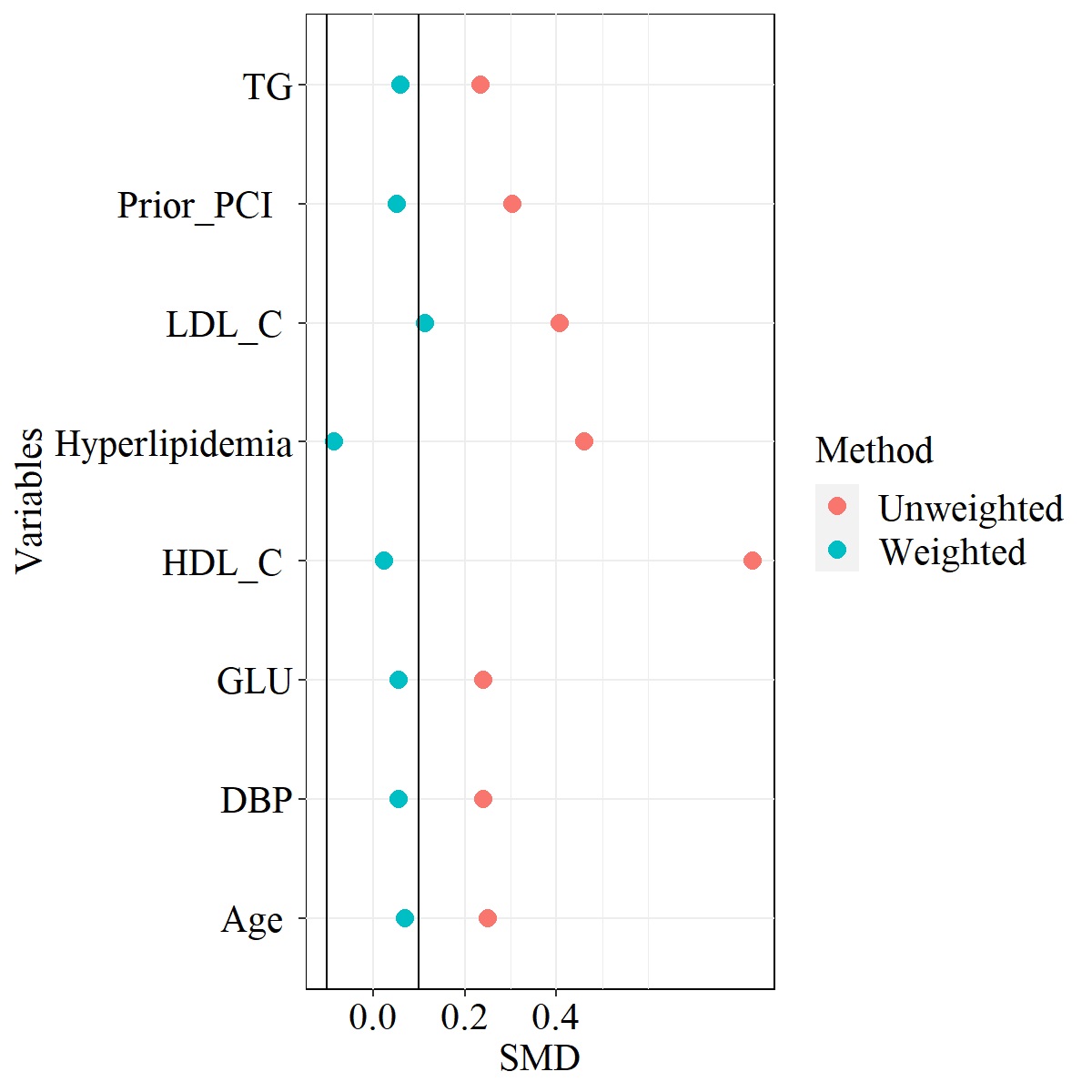
Considering that the factors that might be related to bleeding were not balanced, the IPTW model was used to balance the clinical characteristics from the two groups (Figure 2).
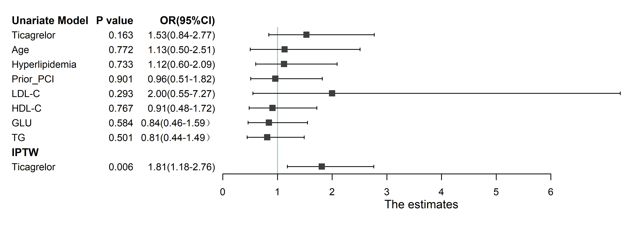
The characteristics were significantly balanced after matching, and it was found that compared with Clopidogrel, Ticagrelor had an adverse impact on the reduction of the incidence of bleeding with the IPTW model (IPTW-OR: 1.81, 95% CI: 1.18-2.76, P=0.006) (Figure 3).
PCI has been applied to CTO at high success rates [14], but CTO-PCI patients presented with higher ischemic incidence because of more complex lesions. Therefore, prolonged DAPT duration is usually recommended for these patients [2,5]. Elderly CTO-PCI patients are also exposed to high risks of bleeding [15], which makes it vitally important to balance both thrombose and hemorrhage for CTO-PCI patients to ensure a desirable prognosis. Previous studies indicated that clinical improvement showed up, regardless whether the DAPT duration was >12 months or not after PCI in CTO patients [16,17]. Considering the reasons above, the duration of DAPT in this study was determined as 12 months. DAPT, which comprises aspirin and a P2Y12 inhibitor, reduces coronary ischemic events after PCI by preventing both stent thrombosis and non-culprit segments thrombosis via antiplatelet aggregation. As P2Y12 inhibitors recommended by many guidelines, Ticagrelor and Clopidogrel can prevent adenosine diphosphate (ADP) dependent activation of platelet aggregation by binding to the P2Y12 receptor [5, 6].
According to the results of the PLATO trial, compared with Clopidogrel, Ticagrelor showed a lower incidence of endpoint events including cardiovascular death, MI and stroke (9.8% vs. 11.7%, P<0>P=0.43) [18,19].In the ESTATE study that enrolled Taiwan acute coronary syndrome (ACS) patients, the patients who took Ticagrelor had a lower incidence of MI, stroke, or vascular death endpoints with marginal statistical significance (7.1% vs. 11.6%, P=0.07), than those taking Clopidogrel, and the incidence of all bleeding was similar (19.6% vs. 14.3%, P=0.13) [20]. Among these studies, more than 80% patients received invasive therapies (PCI or coronary artery bypass grafting (CABG)). The PLATO trial contained 587 Chinese patients (3.1%) and also 2878 elderly patients (15.45%) [18,19], and the ESTATE study included 269 (28.99%) Chinese patients older than 75 years [20]. In these studies, data concerning CTO patients was absent, and Chinese elderly patients accounted only for a small number of the subjects enrolled. Consequently, these studies could hardly represent Chinese elderly CTO population.
In the present study, all the patients were aged ≥75 years and underwent PCI with DES. After 12-month DAPT, the incidence of MACE in Ticagrelor group was lower than that in Clopidogrel group (11.04% vs. 12.19%), but the incidences of overall bleeding (13.64% vs. 9.38%) and BARC 1 bleeding (12.99% vs. 8.13%) were higher in Ticagrelor group, with no statistical significance for all the differences. After balancing clinical characteristics of the two groups, the difference of bleeding incidence was found to be statistically significant. This indicates that Ticagrelor has similar effect in reducing MACE but higher bleeding risk for Chinese elderly CTO-PCI patients. Thus, Ticagrelor showed similar effectiveness but worse safety in comparison with Clopidogrel in our study.
Clopidogrel was reported to have similar MACE but higher bleeding incidence than Ticagrelor for patients after PCI [21-23]. An “East Asian paradox” was known for pointing out that East Asian patients have lower ischemic but higher bleeding risk after PCI [24]. In the PHILO trial which targeted mostly Japanese patients, compared with Clopidogrel, Ticagrelor was found associated with higher incidence of overall bleeding events (23.8% vs. 14.7%, hazard ratio (HR): 1.72; 95% CI: 1.23-2.40) and minor bleeding events (15.2% vs. 9.2%, HR: 1.75; 95% CI: 1.15-2.67), and the incidence of ischemic events (the composite of MI, stroke or vascular-cause death) is not significantly different (9.0% vs. 6.3%, HR: 1.47; 95% CI: 0.88-2.44) [25]. The TICAKOREA trial indicated that Ticagrelor group had higher incidence of clinically significant bleeding (11.7% vs. 5.3%, P=0.002) and minor bleeding (5.2% vs. 1.3%, P=0.02) than the Clopidogrel group, and the incidence of cardiovascular death, MI and stroke was not significantly different between the two groups (9.2% vs. 5.8%, P=0.07) [26]. The Kamir-NIH study based on East Asian population showed that Ticagrelor reduced the risk of ischemic event with statistical significance (8.6% vs. 11.9%, P=0.018), but it had a significantly higher bleeding risk than Clopidogrel (10.8% vs. 4.8%, P<0>
Some study had data concerning DATP of CTO-PCI patients, however, no subjects ofDATP of CTO-PCI patients who aged ≥75 years was reported. In the GF-APT registry, stable coronary artery disease patients who undergoing complex PCI got higher risk of MACEs (11.2% vs. 8.6%) and similar risk of major bleeding (0.6% vs. 0.9%) after 12-months use of Clopidogrel compared with Ticagrelor, and Ticagrelor had higher minor bleeding risk (1.2% vs. 3.4%), 34.1% of the patients in the study were CTOs [28]. This supports our result that Ticagrelor medication has a higher incidence of minor bleeding. One research into Chinese CTO patients who underwent PCI compared the incidences of overall MACE, major bleeding and minor bleeding in normal Ticagrelor dose group and Clopidogrel group, which were (7.3% vs. 14.2%), (4.1% vs. 0.6%) and (23.4% vs. 11.9%), respectively [8]. This indicates that normal dose Ticagrelor triggered lower incidence of MACE but higher bleeding incidence compared with Clopidogrel for Chinese CTO patients. According to the POPular AGE study involving 1002 patients aged ≥70 years with non-ST-elevation acute coronary syndrome (NSTE-ACS), the primary bleeding incidence was higher in Ticagrelor group (24% vs. 18%, P=0.02), and no significant differences was detected in the incidence of cardiovascular death, MI, and stroke between the two groups (11% vs. 12%, P=0.71) [29], which are align with the conclusion that Clopidogrel tend to induce high bleeding risks in elderly NSTE-ACS patients. The MACE incidence in the POPular AGE study largely coincided with that in our study, whereas the MACE incidence of Ticagrelor group in other studies is lower than that in our study. This might be attributed to the greater complexity of lesions of elderly CTO patients, which leads to higher MACE risks. The bleeding incidence in Ticagrelor group in our study is higher than those in the TICAKOREA trial, Kamir-NIH study and GF-APT registry but is lower than incidences in other studies. This may be partly due to the research bias brought by small sample size as well as the differences of baseline and procedure characteristics between the groups that might affect the comparison of the endpoints.
Taken together, DAPT after PCI can benefit aged CTO-PCI patients, and Ticagrelor showed similar MACE but higher incidence of bleeding, especially minor bleeding (BARC 1 bleeding) in contrast to Clopidogrel. As the bleeding events were not clinically relevant, Clopidogrel and Ticagrelor are considered with similar effectiveness and safety in elderly Chinese CTO-PCI patients. However, Ticagrelor should be prescribed cautiously to patients with a high bleeding risk. This study shed lights in potential clinical application of Clopidogrel and Ticagrelor. Still, a further prospective, multi-center and large-scale trials are required to verify the effectiveness and safety of Ticagrelor and Clopidogrel in elderly CTO patients who underwent PCI.
The study still maintains a few limitations. As a single center retrospective study but with a small sample size, the selection bias was hardly avoidable and the methodological biases exist. Additionally, cardiovascular death was not identified and separately analyzed in our follow-up, with the CTO score, opening techniques or the occurrence of stroke, not considered. More, analysis of effectiveness end points wasn’t adjusted accordingly, given the unavailability of nonfatal MI date and clinically driven revascularization. Lastly, therapeutic agents such as β-blocker were not included in this study, and neither did we evaluate the major adverse effects of P2Y12 inhibitors including dyspnea, hyperuricemia, and asymptomatic heart block.
This clinical study demonstrated that Clopidogrel and Ticagrelor have similar effectiveness and safety to elderly Chinese CTO-PCI patients in improving their prognosis, yet Ticagrelor should be prescribed with caution to eliminate potential bleeding.
DAPT: dual antiplatelet therapy; PCI: percutaneous coronary intervention; CTO: chronic total occlusion; MACE: major adverse cardiac event; MI: myocardial infarction; BARC: Bleeding Academic Research Consortium; IPTW: inverse probability of treatment weighting; CAD: coronary artery disease; MI: myocardial infarction; DES: drug-eluting stents; TIMI: Thrombolysis In Myocardial Infarction; LM: left main artery;LAD: left anterior descending artery; LCX: left circumflex artery; RCA: right coronary artery; BARC: Bleeding Academic Research Consortium; DBP: diastolic blood pressure; Glu: glucose; TG: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholestero; SMD: standardized mean differences; IPTW: inverse probability of treatment weighting; ADP: adenosine diphosphate; ACS: acute coronary syndrome; CABG: coronary artery bypass grafting; HR: hazard ratio; AMI: acute myocardial infarction; MVD: multivessel disease; NSTE-ACS: non-ST-elevation acute coronary syndrome.
Declarations
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Air Force Medical University (KY20172019-1). Written informed consents were obtained from all participants.
Consent for Publication
The consent was obtained from all authors for publication of this study.
Availability of Data and Materials
The datasets generated and analyzed in the current study are available from the corresponding author on reasonable request.
Funding
This work was supported by Shaanxi Province Key Research and Development Program General Project—Social Development (2018SF-153), Xi’an Science and Technology Project (20YXYJ0003(4)), New Clinical Technology and New Business of Xijing Hospital (XJGX15Y39), Bethune-Merck Diabetes Research Foundation (G2017044).
Conflict of Interest
The authors have no conflicts of interest to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
